Dr. Pepe’s Diploma Casebook: Case 70 – SOLVED!

Dear Friends,
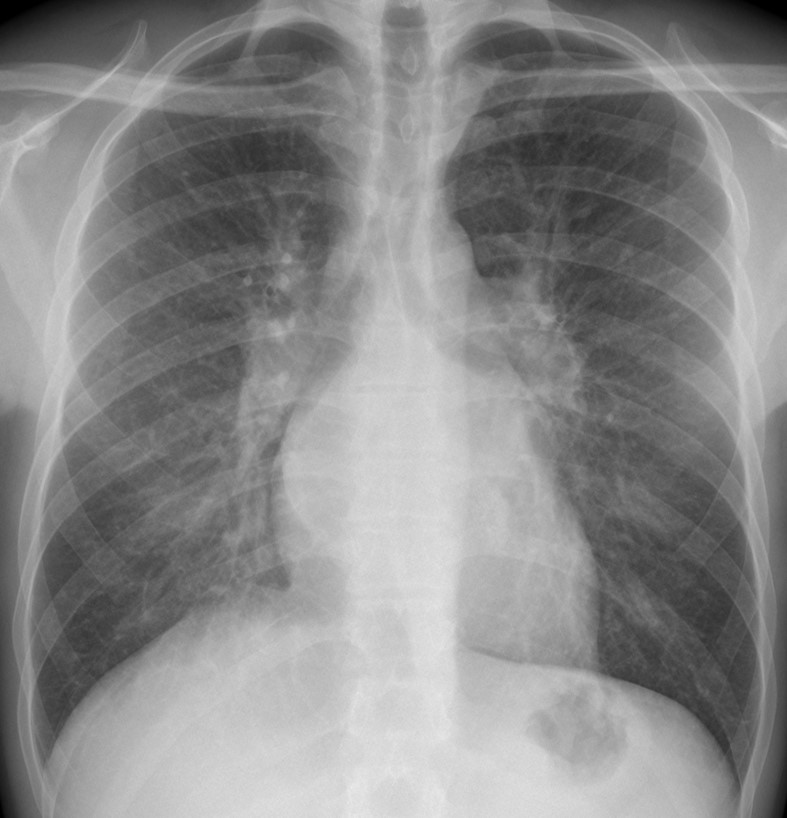
Today I am showing chest radiographs of a 34-year-old male with dyspnea. Check the images below, leave your diagnosis in the comements section and come back on Friday for the answer.
Diagnosis:
1. Mitral disease
2. Pulmonary arterial hypertension
3. Interstitial pneumonia
4. None of the above

Findings: PA radiograph shows redistribution of the pulmonary vessels. The hila are enlarged and blurry. The left atrium and atrial appendage have a double contour (A, white arrows). Calcium is visible in the area of the mitral valve (A,B, red arrows).
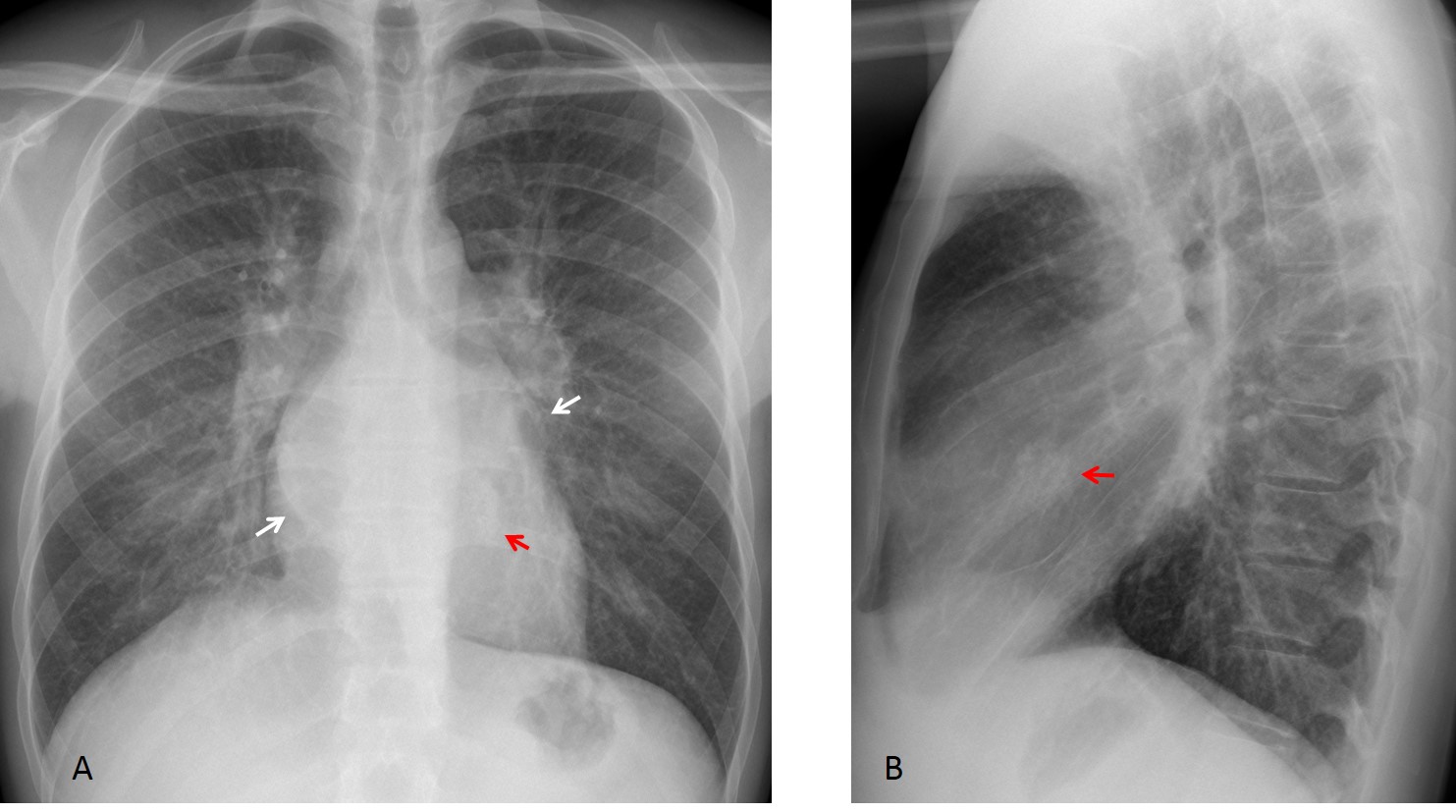
CT confirms the left atrial enlargement (C,D white arrows), as well as calcium in the mitral valve (C,D, red arrows).
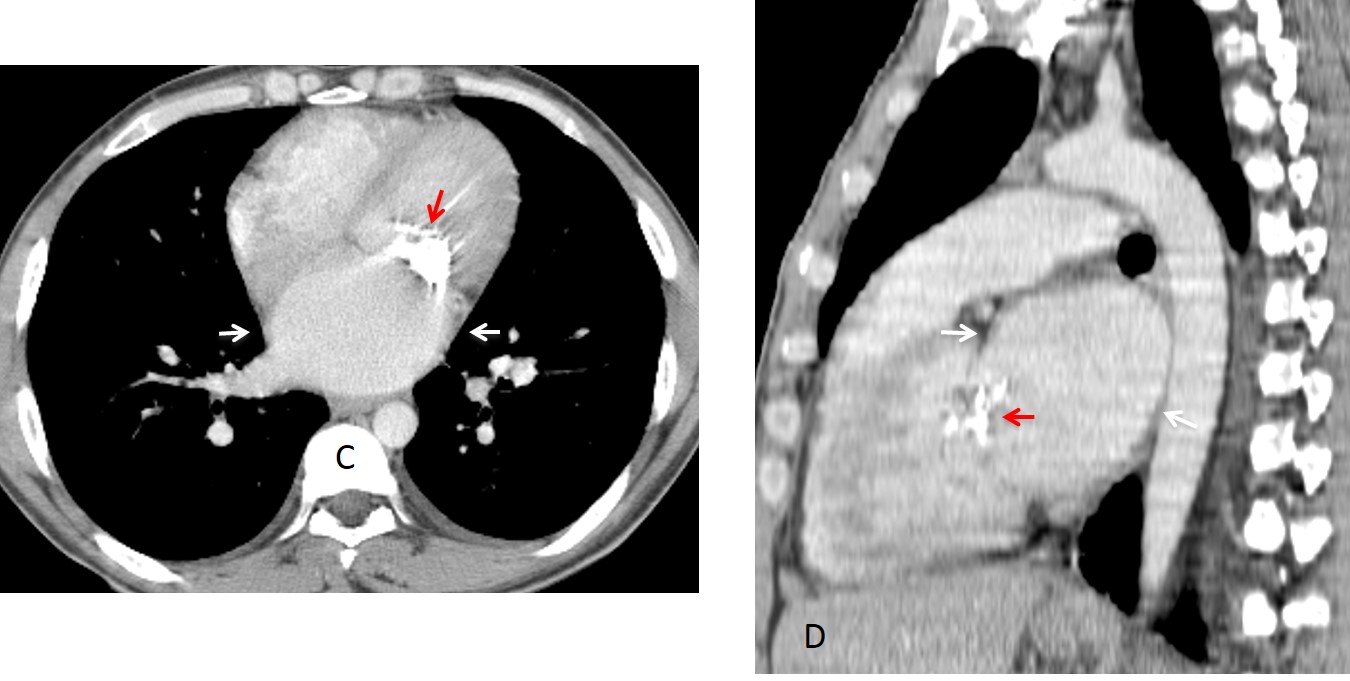
Final diagnosis: calcified mitral stenosis with vascular redistribution.
This case is presented to discuss redistribution pattern of the pulmonary vessels.
In the normal erect PA view, the vessels of the upper lobes are smaller than those of the lower ones (Fig. 1 A). In redistribution, the upper vessels are larger than the lower ones (Fig. 1 B).
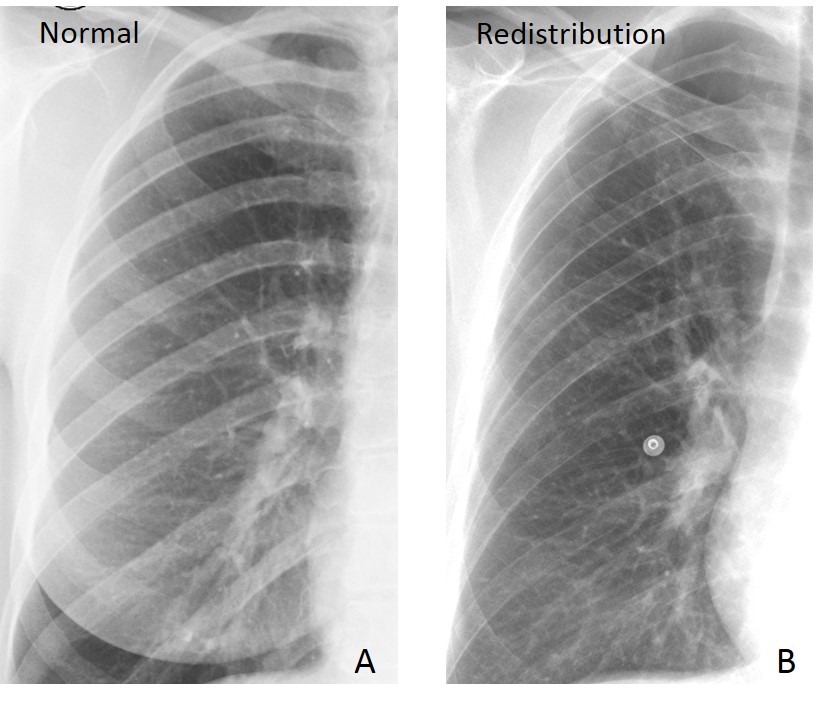
Fig. 1
Fig. 1: Normal vascular pattern (A) and redistribution (B). Note the small upper vessels in A compared with the lower ones. In B, the appearance is reversed. Redistribution is better seen in the right lung because the left lower vessels are obscured by the heart.
I am using the word redistribution as a purely anatomical term, without specifying the etiology. The great majority of cases have a cardiovascular etiology, secondary to increased left atrial pressure, causing the blood to back up into the pulmonary veins. As a consequence, the arteries of the lower lobes constrict, redistributing the flow to the upper vessels, which then appear larger than the lower ones.
Recognising redistribution needs a certain degree of expertise, but it is rewarding because it may reveal a cardiovascular problem before clinical findings are evident.
Although most cases of redistribution have a cardiovascular etiology, obstruction of lower lobe arteries and basal emphysema may give similar findings.
Cardiovascular redistribution can be classified as obstructive or non-obstructive.
The main cause of non-obstructive redistribution is left-sided heart failure. When the left heart fails, blood collects in the pulmonary veins, causing redistribution as an early sign. If failure progresses, pulmonary oedema develops (Fig. 2).
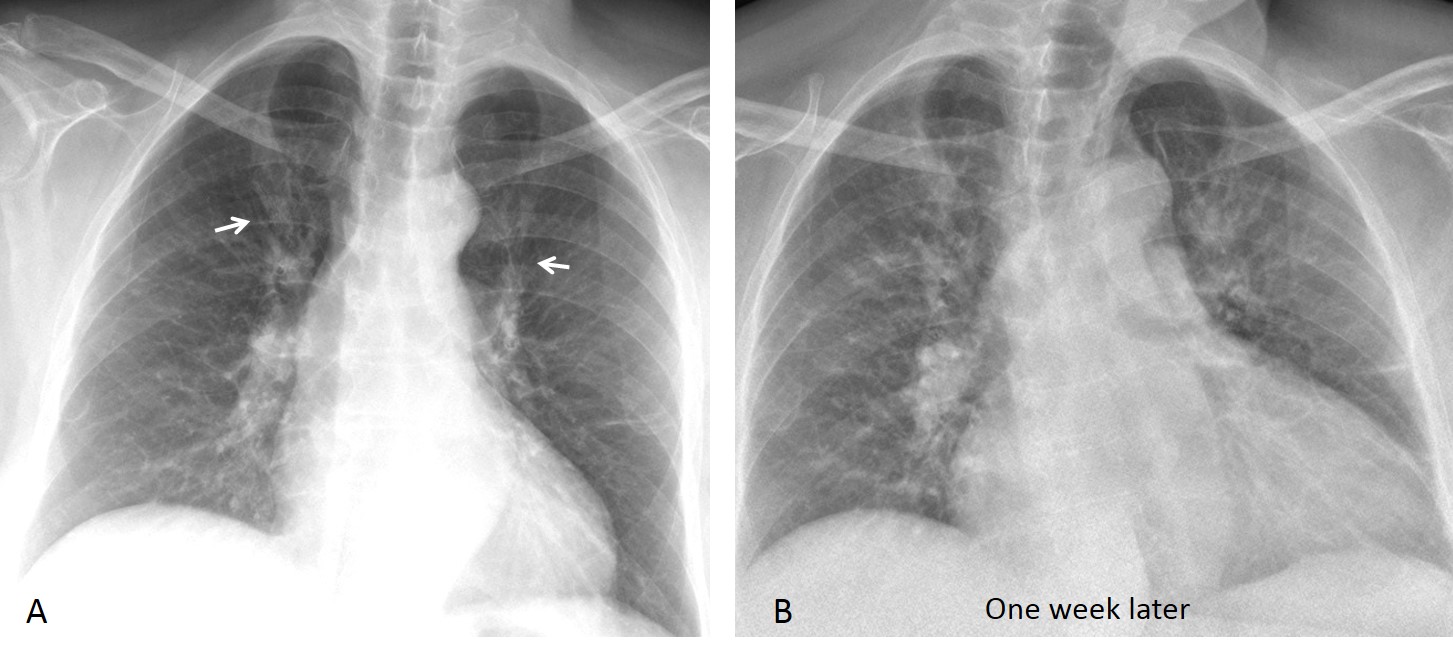
Fig. 2
Fig. 2: 65-year-old man with cardiomyopathy. Initial film shows borderline cardiac enlargement and redistribution (A, arrows). One week later, the heart has enlarged and there is pulmonary oedema (B).
A relatively common cause of non-obstructive redistribution is atrial fibrillation, which occurs in 5% of individuals older than 65. Consider atrial fibrillation when you see left atrial enlargement and vessel redistribution in an elderly patient (Figs. 3 and 4). The diagnosis is important because embolic stroke is a common complication.
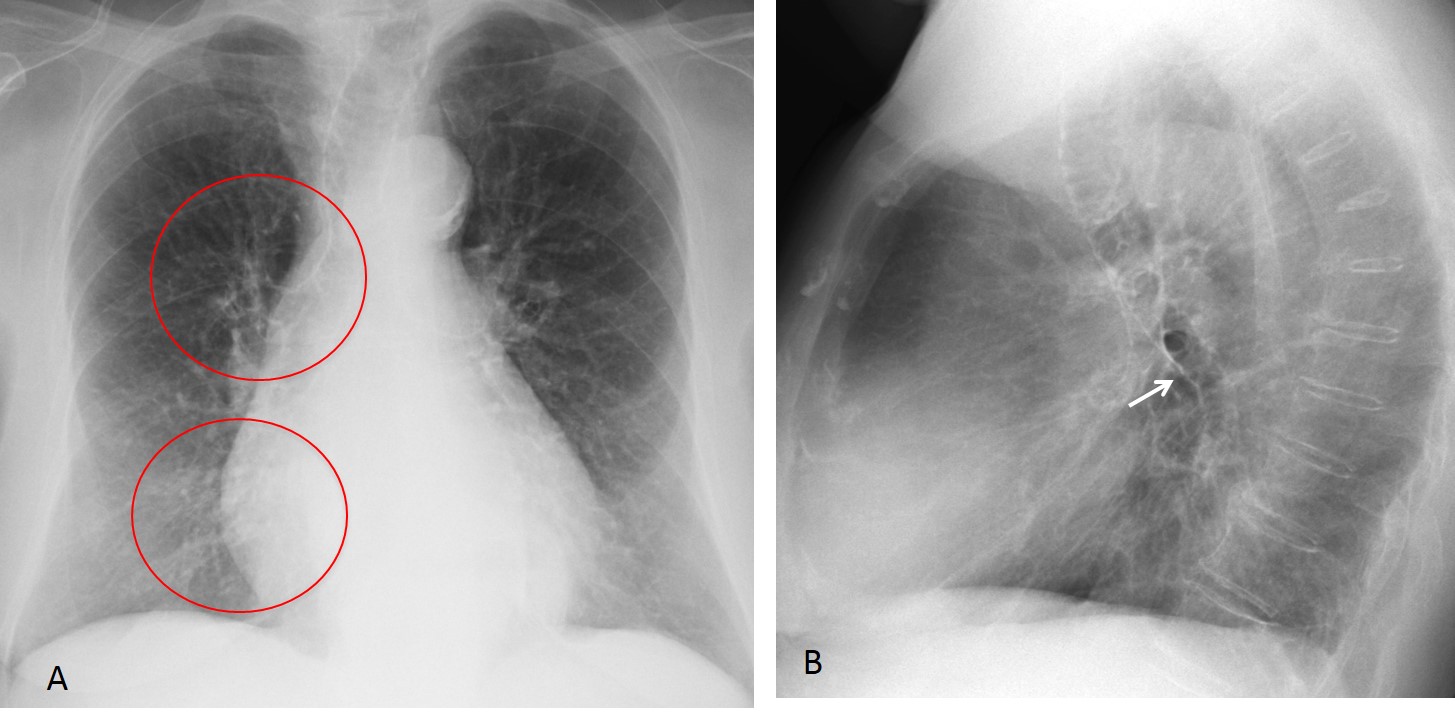
Fig. 3
Fig. 3: 72-year-old woman with dizzy spells. PA chest film shows moderate cardiomegaly and redistribution (A, circles). Lateral view shows posterior displacement of the left bronchus (B, arrow), a sign of atrial enlargement. Diagnosis: atrial fibrillation.
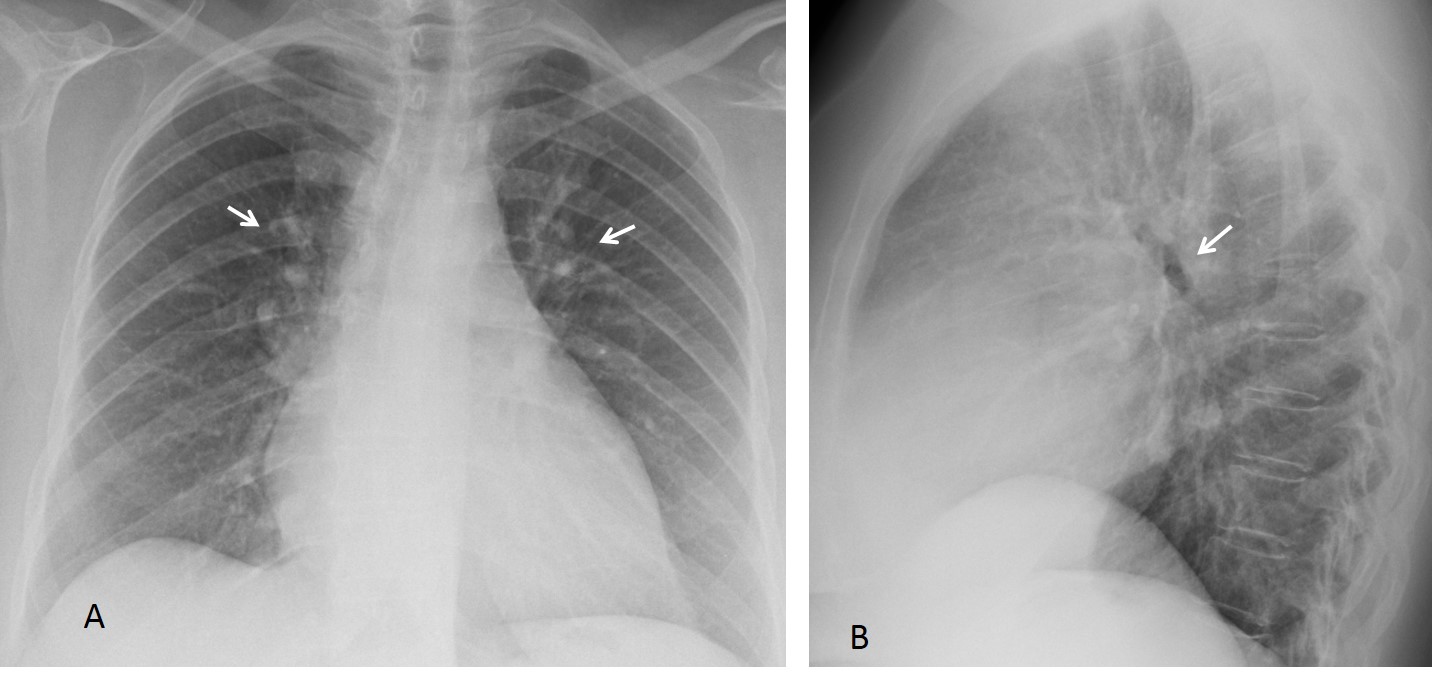
Fig. 4
Fig. 4: 68-year-old woman with moderate cardiomegaly, redistribution (A, arrows) and posterior displacement of left bronchus (B, arrow). Again, atrial fibrillation.
The main causes of obstructive cardiovascular lesions are mitral valve disease, aortic valve stenosis, and aortic coarctation. Rheumatic mitral disease used to be the most frequent obstructive cause of redistribution. It is now uncommon in developed countries, but is still seen in citizens of less favored ones. The findings are well known and are described in Fig. 5.
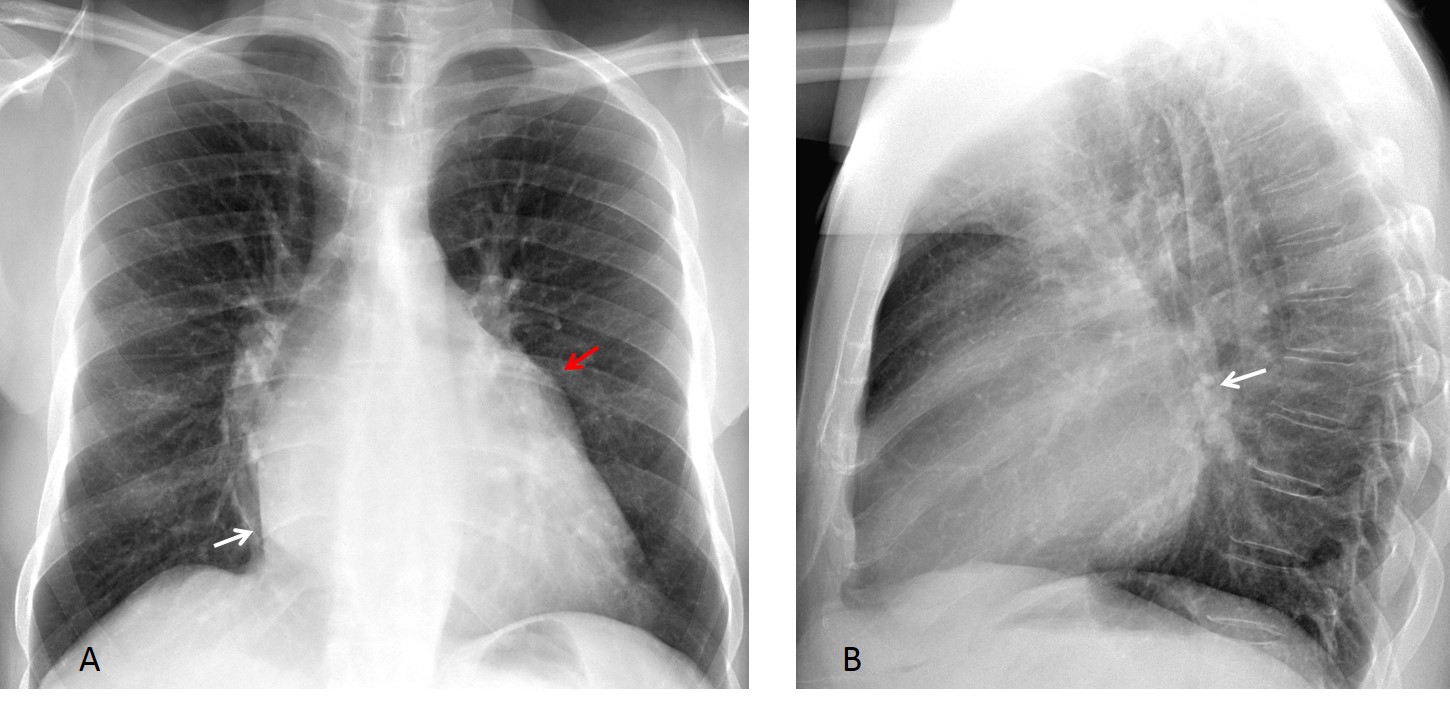
Fig. 5
Fig. 5: 28-year-old immigrant with typical findings of mitral disease. PA view shows redistribution, double contour of left atrium (A, white arrow), and prominent appendage (A, red arrow). There is posterior prominence of left atrium (B, arrow).
Stenotic lesions of the aorta also increase pressure in the left side of the heart, resulting in redistribution. The most common is coarctation, although any aortic obstruction can produce similar findings (Fig. 6).
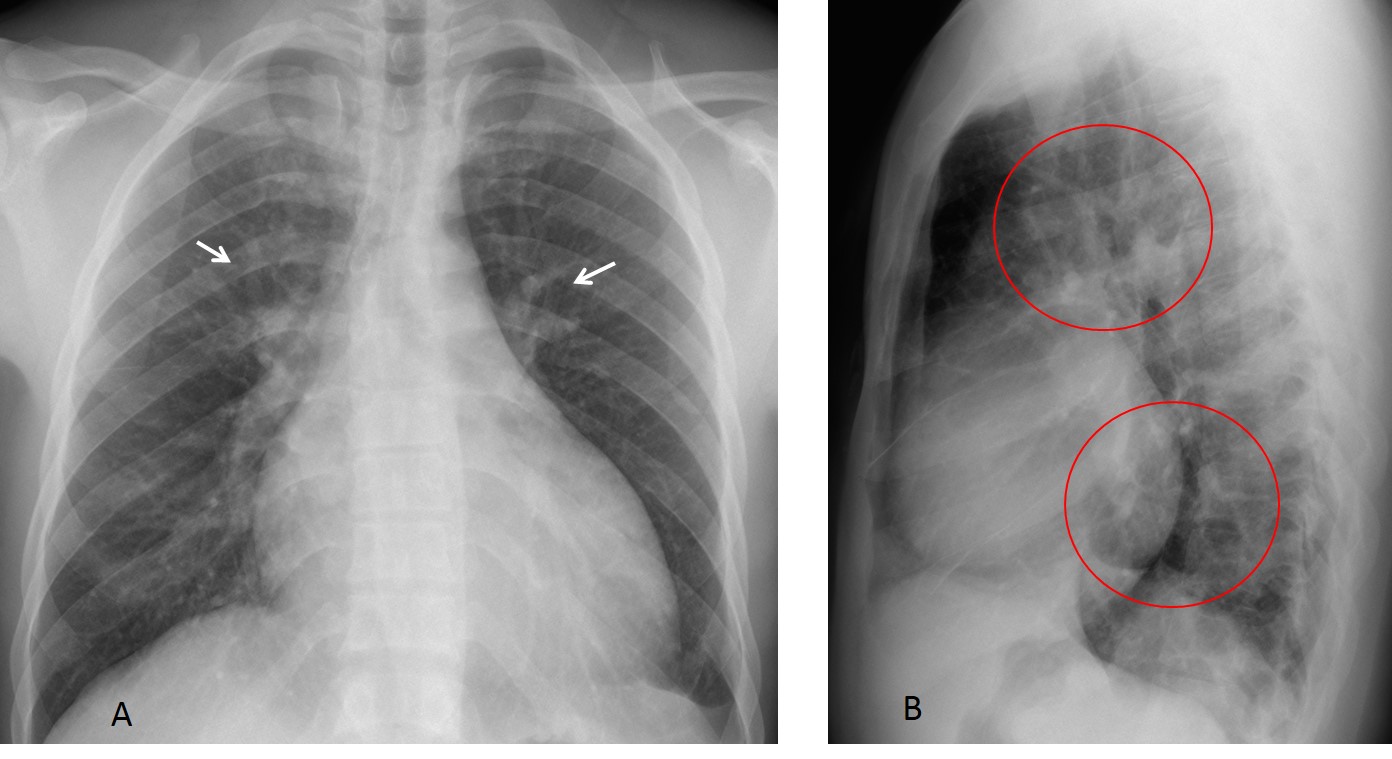
Fig. 6
Fig. 6: 27-year-old man with elevated blood pressure. PA chest film shows cardiomegaly and redistribution (A, arrows). In this particular case, redistribution is also seen in the lateral view (B, circles).
3D reconstruction shows thinning and interruption of the thoracic aorta (C, arrows) with marked collateral circulation. A thoracic-to-abdominal aortic bypass was placed (D, arrow). Post-op radiograph shows decrease in heart size and in redistribution. Note the outline of the graft (E, arrows). Diagnosis: mid-aortic syndrome, secondary to Takayasu disease.
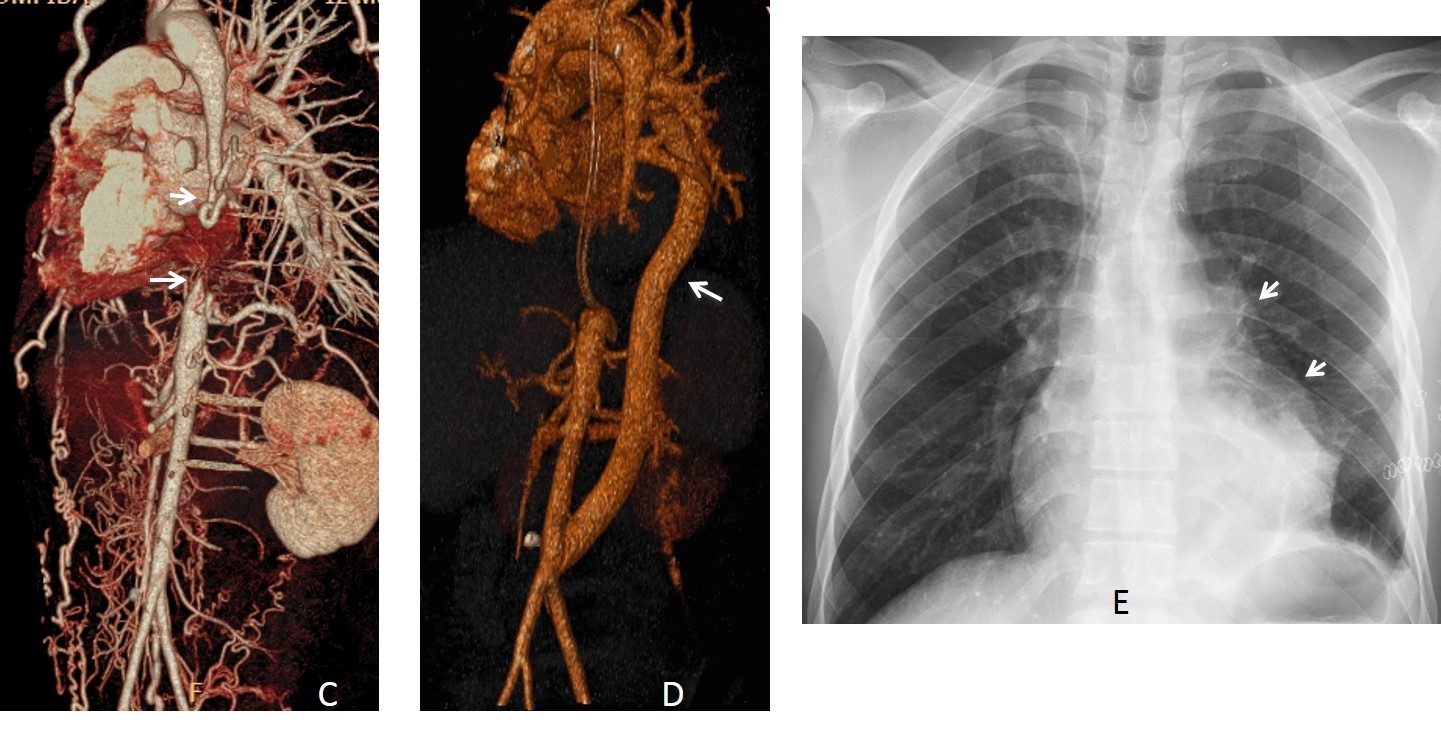
Fig. 6
Obstruction of lower lobe pulmonary arteries is an uncommon cause of redistribution. It can occur in pulmonary embolism (Fig. 7) or in vasculitis (Fig. 8).
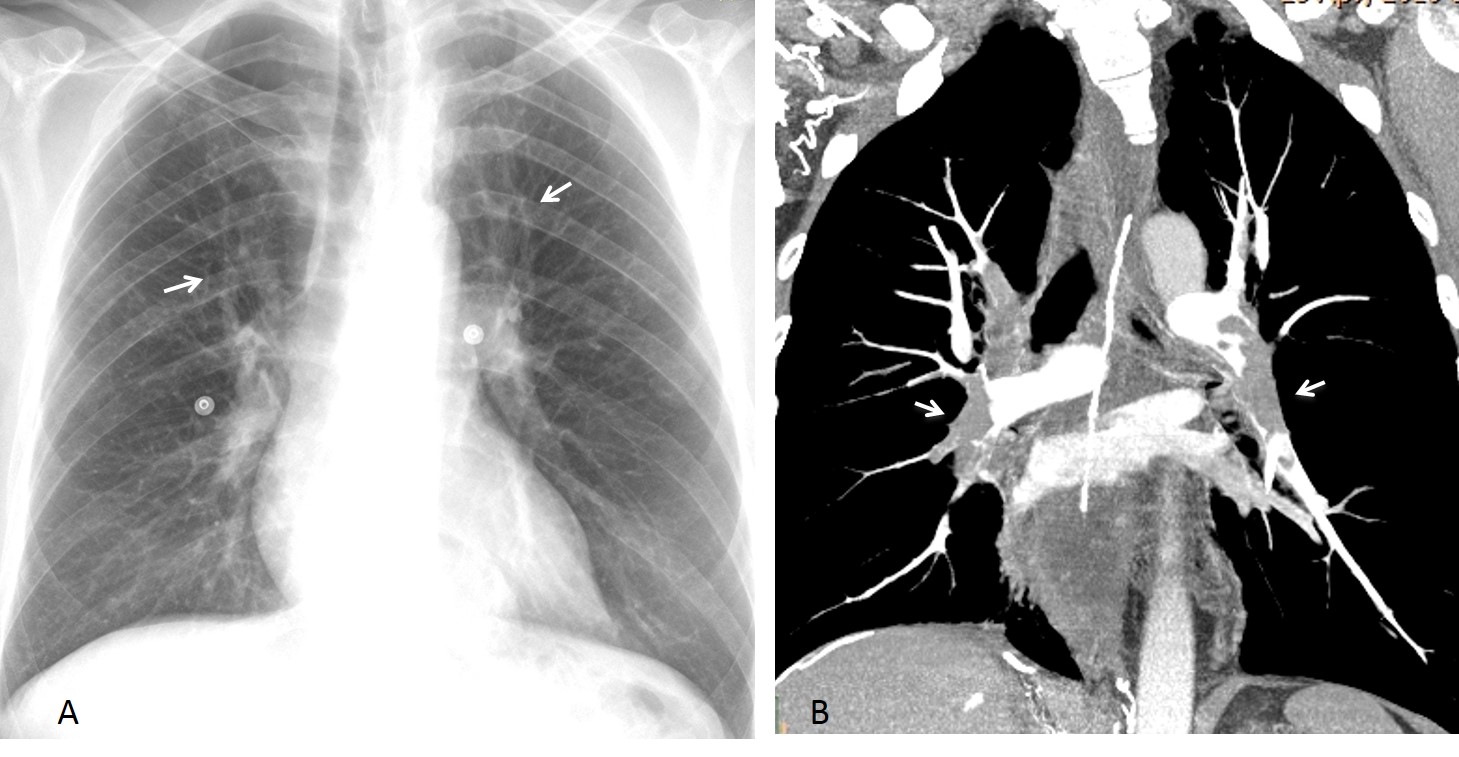
Fig. 7
Fig. 7: 45-year-old man with lower limb phlebitis and severe dyspnea. PA chest film shows redistribution (A, arrows) with a normal-sized heart. CT angiogram confirms the redistribution, secondary to multiple emboli, mainly to lower lobe arteries (B, arrows).
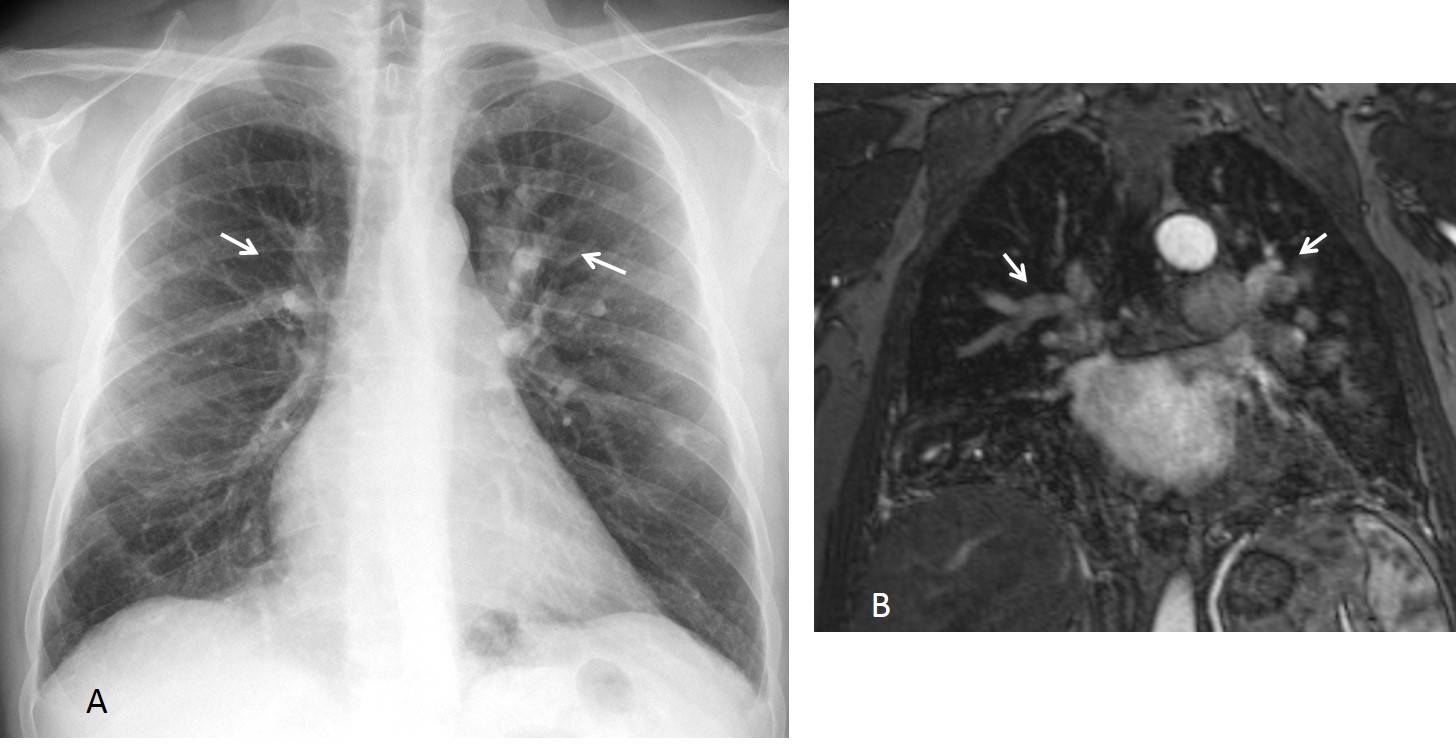
Fig. 8
Fig. 8: 48-year-old man with cognitive problems. PA chest film depicts obvious redistribution (A, arrows). MR angiogram shows that blood flow is decreased in the lower pulmonary arteries and increased in the upper ones (B, arrows). Diagnosis: Takayasu
Emphysema of lower lobes diminishes the blood flow and increases the flow to the upper vessels. In these cases, the etiologic diagnosis is obvious (Fig. 9).
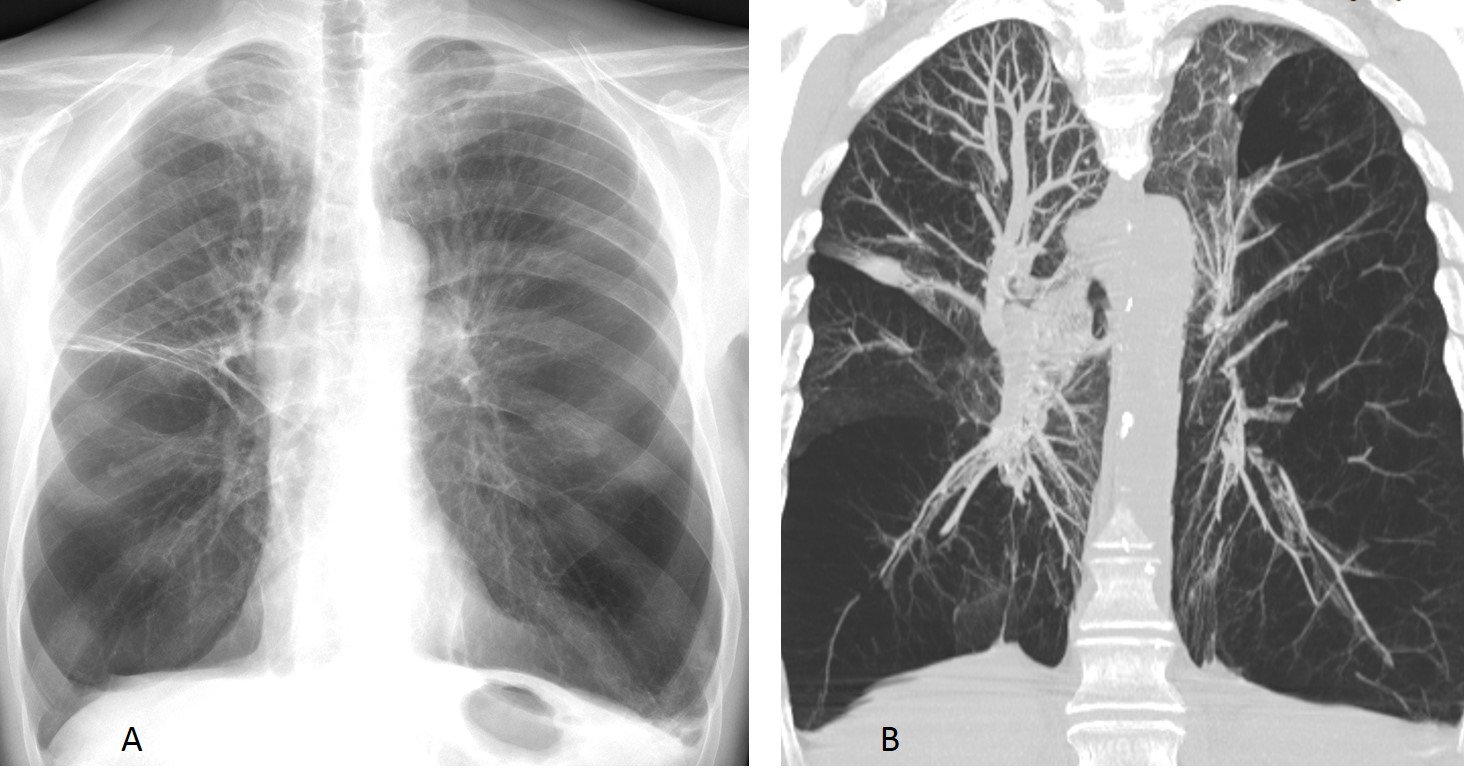
Fig. 9
Fig. 9. 68 y.o. man with alpha 1 antitrypsin emphysema. Marked emphysema of lower lobes causes redistribution (A), confirmed on coronal CT (B).

Follow Dr.Pepe’s Advice:
1. Redistribution may reveal underlying heart problems before clinical symptoms are obvious.
2. Non-obstructive causes of redistribution are left heart failure and atrial fibrillation.
3. Nowadays, the most common obstructive cause of redistribution is aortic valve stenosis.
4. Uncommon causes of redistribution are obstruction of lower lobe arteries and lower lobe emphysema.


Hello,
I think We can see here increased vasculature with moderate hilar vessels dilation but without amputation (characteristic for pulmonary artery hypertension). Vessels seem to be also superiorized.
This would suggest congestive problem ergo mitral stenosis.
On the PA view left atrium might be enlarged- on the lateral view also but would be better visualized with oral barium swallow technique.
Pateient is young so he probably has good compensation mechanism and that is why We don’t see any pleural fluid or apparent edema (interstitial)
…non ci sono i segni della IP…..una forma di pneunopatia di tipo interstiziale e’ un miraggio con l’ rx- tradizionale( HR-tac)….e’ invece compatibile con una cardiopatia mitralica, ancora compensata….lieve congestione ilare vascolare , con iniziale ridistribuzione del flusso in senso caudo-craniale e presenza di ‘ doppio’ contorno sul profilo cardiaco di dx, come da mega orecchietta mitralica…..se poi, ricordandoci che siamo ‘anche’ clinici, sappiamo che ci sono soffi alla auscultazione cardiaca e conosciamo i risultati della eco-cardiaca, la diagnosi si completa….il Bari un disastro in campionato….come il REAL( godono i blu grana?)….
Straightening of left heart border and double density of right heart border imply LA enlargement. Enlarged pulmonary vessels with cephalisation.
Overall features are of pulmonary venous hypertension. Cause is Mitral stenosis or myxoma in Left heart.
Faint round opacity over the left ventricle region seen on both frontal and lateral projection suggests presence of (partially calcified) myxoma.
Diagnosis:
LV myxoma complicated by pulmonary venous HT.
For echocardiogram and MRI cardiac.
Evidence of left paratracheal opacity seen more obvious in lateral film, suggestive of LUL consolidation…supported by mild upward shifting of the left hilum…prominent both hilar shadows with bilateral peribronchial cuffing…thinking of Sacroidosis, yet could not explain the enlarged left atrium causing cardiac double contour…Vote for 4
1. Mitral disease
pul hypertension
double shadow of the lower right heart shadow, superior displecment of the lift main bronchus. calcificasion of the anulus of mitral valve. The findings suggest for mitral gesease
Pulmonary arterial hypertension secondary to mitral stenosis 🙂
Enlarged pulmonary vessels and double contourn of the right hearth border like as LA enlargement, maybe some calcifications on lateral view overlapping hearth shadow..vote for 1.
Mitral valve disease
dilatation of the left atrium in keeping with mitral valve disease (stenosis)
Mitral disease
Mitral stenosis
Double contour of loft atrium
Mitral disease
Mitral stenosis
Congatulations to all of you. Mitral disease is the right diagnosis. This case is presented to discuss vascular redistribution. More information tomorrow.
Diagknowsis: I think the photograph was of painting done in the 18th century. The artist tried to draw the inside of a very tensed dude using charcoal. This dude whose insides were drawn should be suggested to chill out.
Lol