Dr. Pepe’s Diploma Casebook: Case 76 – SOLVED!
Dear Friends,
Only three more cases until summer vacation! Present images belong to a 58-year-old man with fever and malaise. Patient is allergic to contrast media. Have a look at the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Esophageal leiomyoma
2. Duplication cyst
3. Aortic aneurysm
4. Any of the above


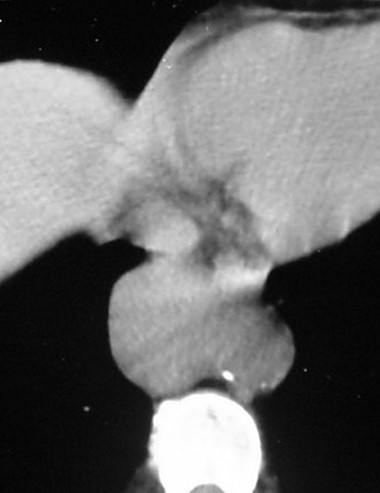
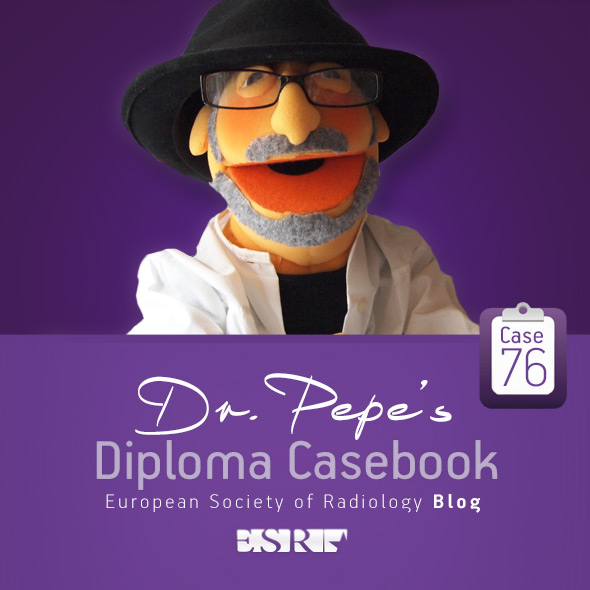
Findings: PA and lateral radiographs show a mass in the lower middle mediastinum (A and B, arrows). Unenhanced CT depicts a rounded soft tissue density mass (C, arrow). Of the three answers offered, all are possible: duplication cyst may show high density, and an aneurysm cannot be ruled out without contrast enhancement. Therefore, the correct answer is no. 4, any of the above.
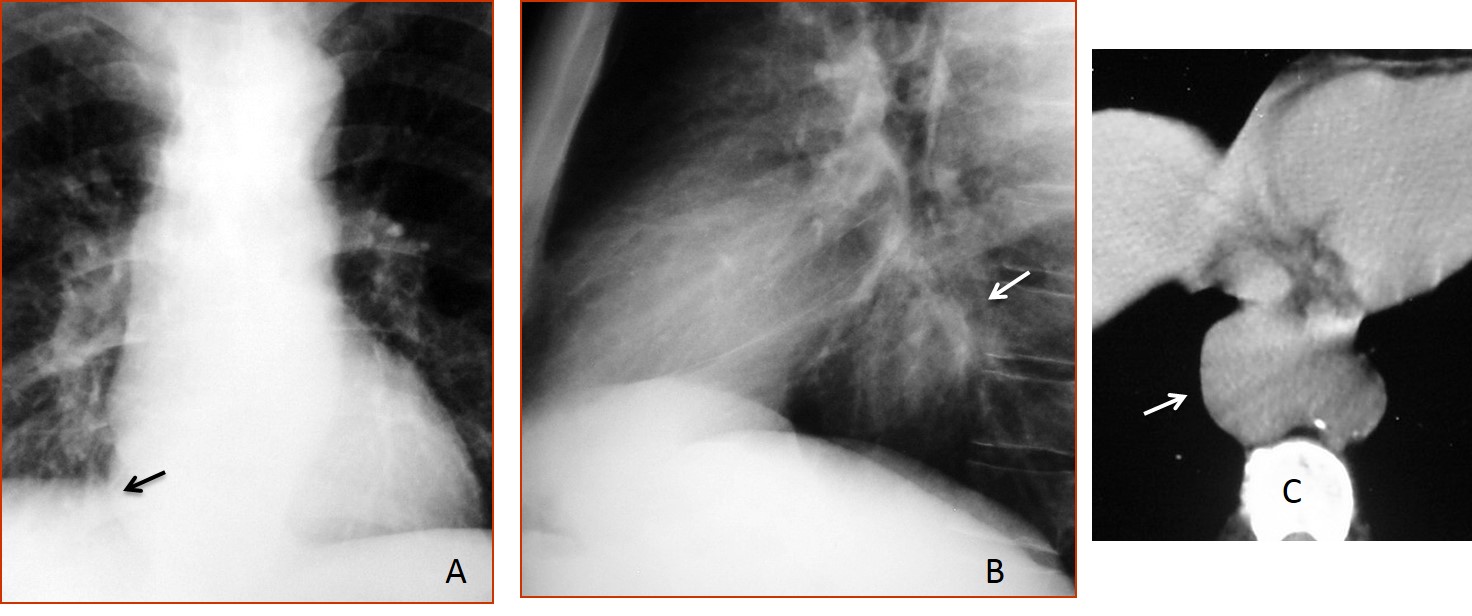
Because of the patient’s allergy to contrast medium, MRI was done. Axial and coronal views show that the mass corresponds to an aneurysm arising from the lateral wall of the aorta (D and E, arrows).
Diagnosis: aneurysm of descending aorta (mycotic).
This case is presented to discuss middle mediastinal masses. Most of these masses correspond to lymphadenopathy, foregut duplication cysts, vascular lesions, or esophageal conditions. Assessment of CT attenuation is helpful in the differential diagnosis. All CT studies should have contrast enhancement to exclude vascular lesions simulating a mediastinal mass, as occurred in the case presented.
As was mentioned in Diploma Casebook case #41, the mediastinum is divided into 4 compartments (anterior, middle, posterior, and thoracic inlet). The middle mediastinum is limited by a line that follows the anterior wall of the trachea and the posterior border of the heart and a second line drawn 1 cm behind the anterior contour of the spine. To facilitate the differential diagnosis, the middle mediastinum is subdivided into three compartments (superior, middle, and inferior) by a horizontal line drawn at the level of the aortic arch and a second line drawn below the hilar region (Fig. 1).
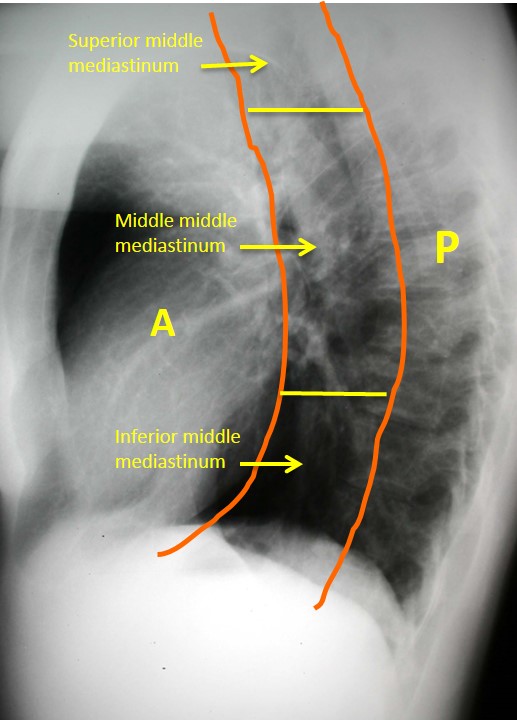
Fig. 1
The most common mass seen in the superior mediastinum is intrathoracic goiter. A small percentage of these lesions extend to the anterior mediastinum. Goiters displace the trachea in the chest radiograph and show high density on unenhanced CT because of their high iodine content (Fig. 2). Focal calcifications are not uncommon.

Fig. 2
Fig. 2: 52-year-old man with moderate dyspnea. Chest radiographs show a large mass in the superior middle mediastinum, displacing the trachea (A and B, arrows).
Coronal CT shows that the density of the mass (C, arrow) is higher than that of the surrounding soft tissues. Sagittal CT depicts scattered calcifications (D, white arrow) and hypodense areas within the mass (D, red arrow). The CT appearance is typical of intrathoracic goiter.

Fig. 2
A characteristic finding in intrathoracic goiters is marked early and prolonged enhancement after contrast injection (Fig. 3).
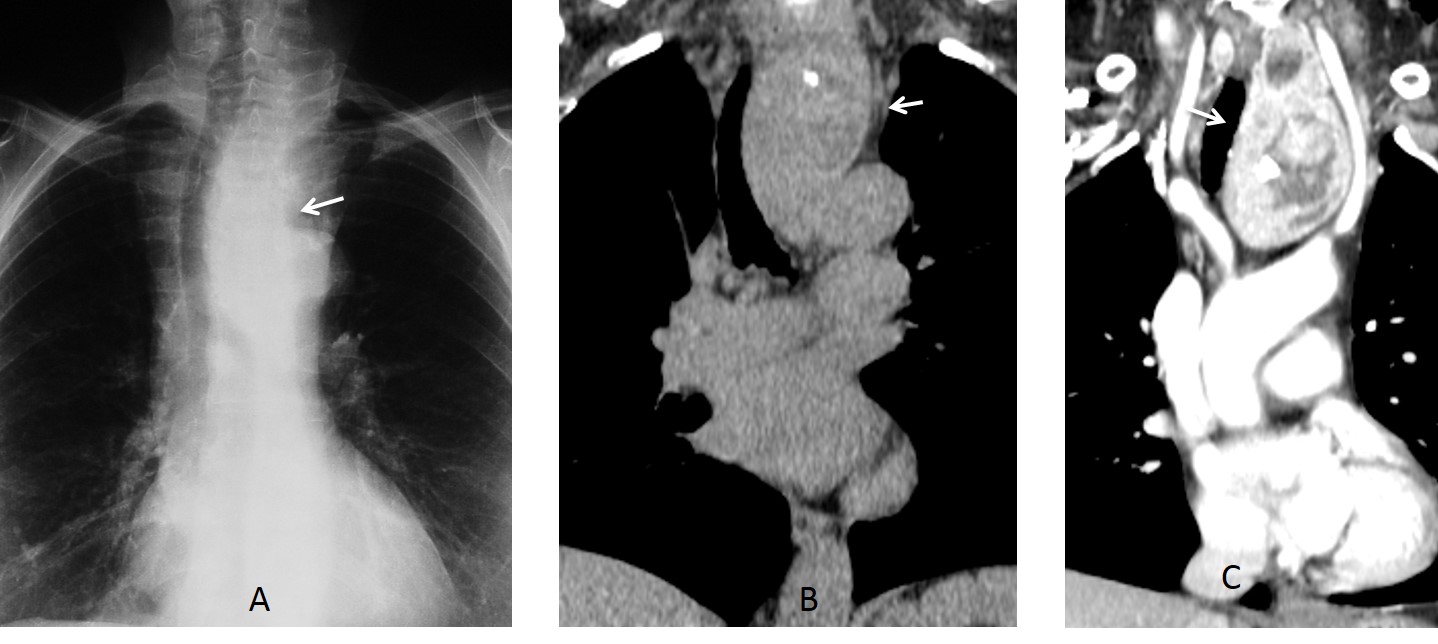
Fig. 3
Fig. 3: 47-year-old man with intrathoracic goiter. PA radiograph shows a mass displacing the trachea (A, arrow). Unenhanced CT confirms the mass (B, arrow). After contrast injection, the mass enhances markedly (C, arrow), confirming the diagnosis of goiter.
Aneurysms of the aortic arch may simulate a mass in the superior middle mediastinum. The trachea may be displaced or not, depending on the location. The diagnosis is easily made with enhanced CT (Fig. 4).
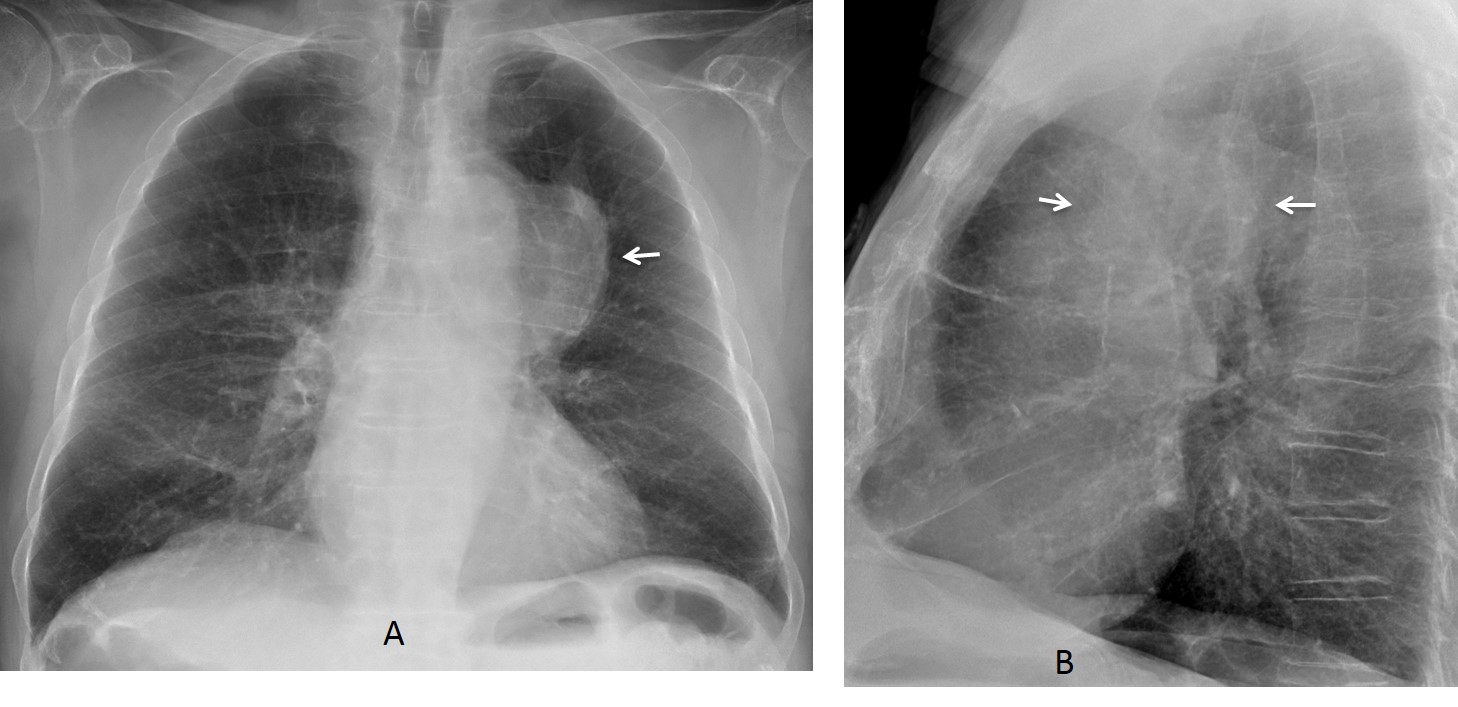
Fig. 4
Fig. 4: 52-year-old man, asymptomatic. Chest radiographs show a mass in the middle mediastinum (A and B, arrows). The trachea is not displaced.
Axial and sagittal enhanced CT show a partially thrombosed aneurysm arising from the aortic arch (C and D, arrows). The location of the aneurysm explains the absence of tracheal displacement.
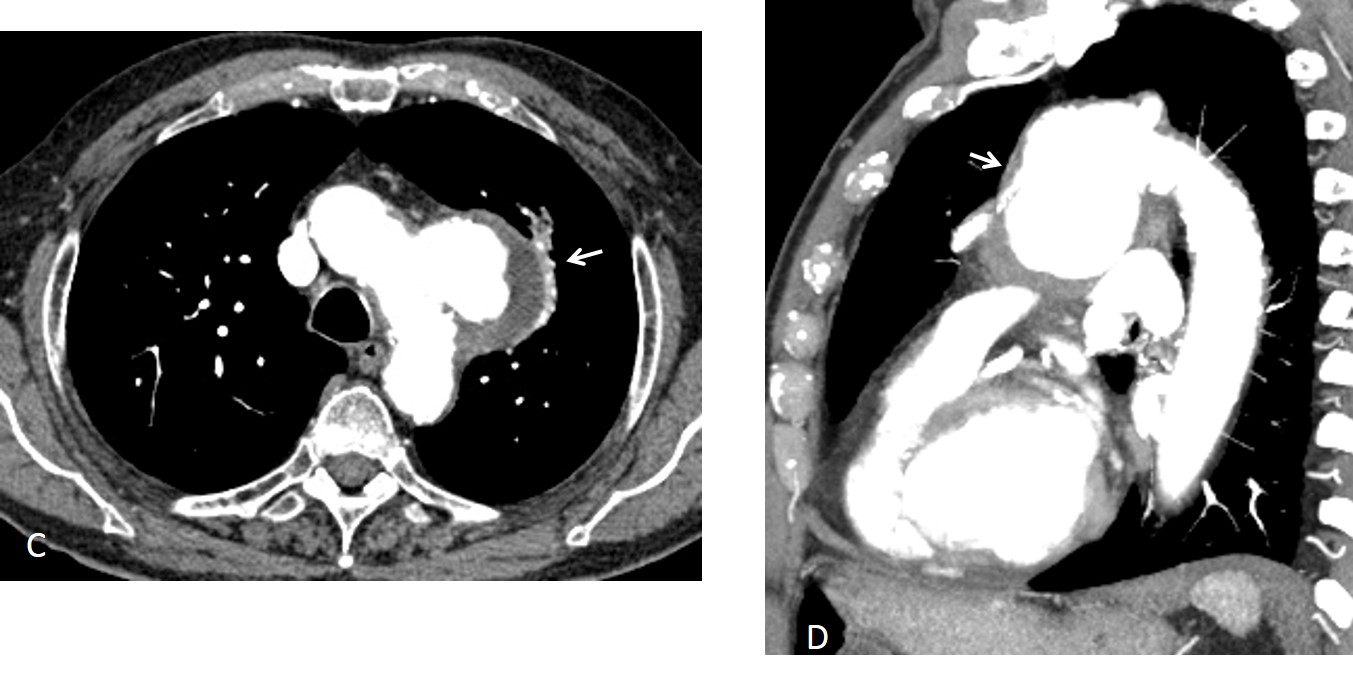
Fig. 4
Mediastinal lymphadenopathy can occur in any location in the middle mediastinum. When the enlarged node is in the upper area, it is usually seen as a right paratracheal mass on the PA chest radiograph (Fig. 5). The etiology of the findings cannot be established on plain film features, but it is easily depicted on CT.
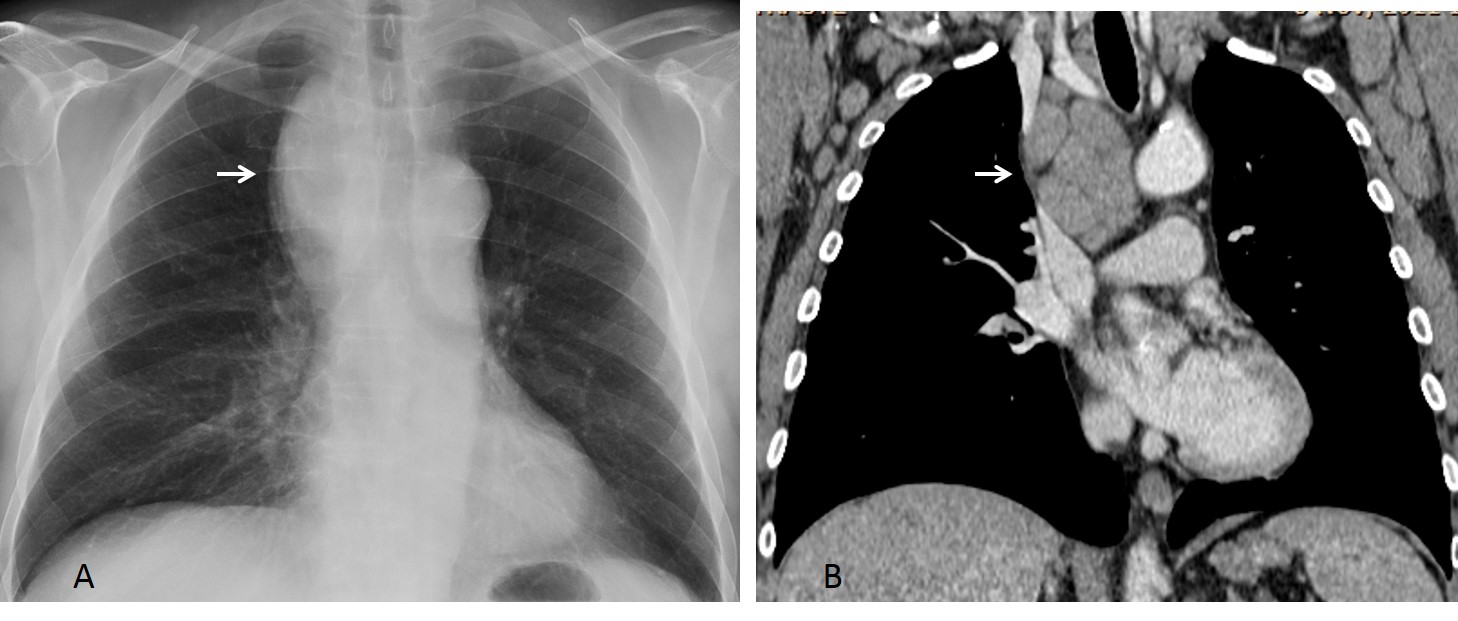
Fig. 5
Fig. 5: 72-year-old man with weight loss and asthenia: PA chest film shows a large paratracheal mass (A, arrow), with minimal tracheal displacement. Coronal CT depicts multiple lymph nodes in the upper mediastinum (B, arrow). Diagnosis: chronic leukemia.
In the middle portion of the mediastinum, the most common conditions are enlarged lymph nodes and duplication cysts. Enlarged lymph nodes usually appear as a subcarinal mass, better seen on the lateral view. They may be secondary to lymphoproliferative disease, metastasis, or granulomatous disease. Calcified lymph nodes suggest an old granulomatous condition. Low-attenuation nodes are suggestive of TB (Fig. 6).
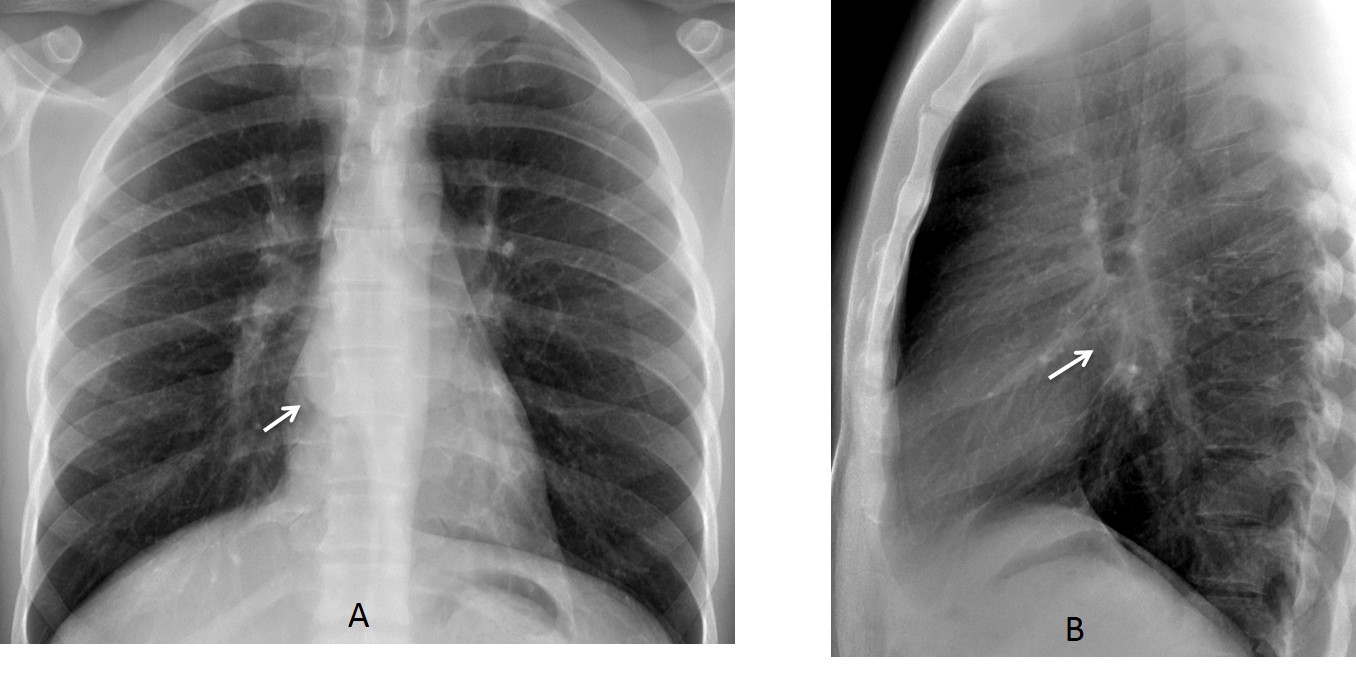
Fig. 6
Fig. 6: 25-year-old man, a native of Pakistan, with dysphagia. PA and lateral radiographs show a subcarinal mass (A and B, arrows).
Enhanced axial and coronal CT depicts a mass of matted lymph nodes with numerous low-density areas (C and D, arrows). Diagnosis: TB.
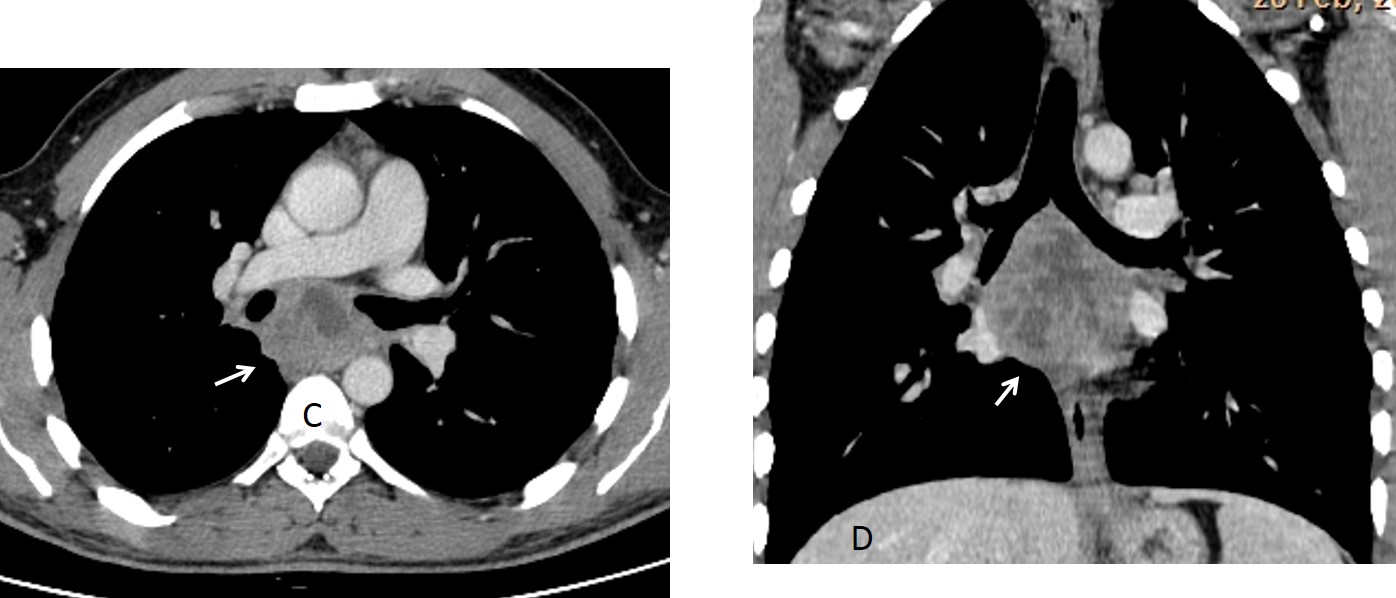
Fig. 6
Congenital foregut cysts account for about 20% of mediastinal masses. Most of them arise around the carinal area. They may be hidden in the PA view, and are discovered in the lateral projection (Fig. 7). On CT they appear as a round mass of water attenuation which does not change after contrast enhancement.
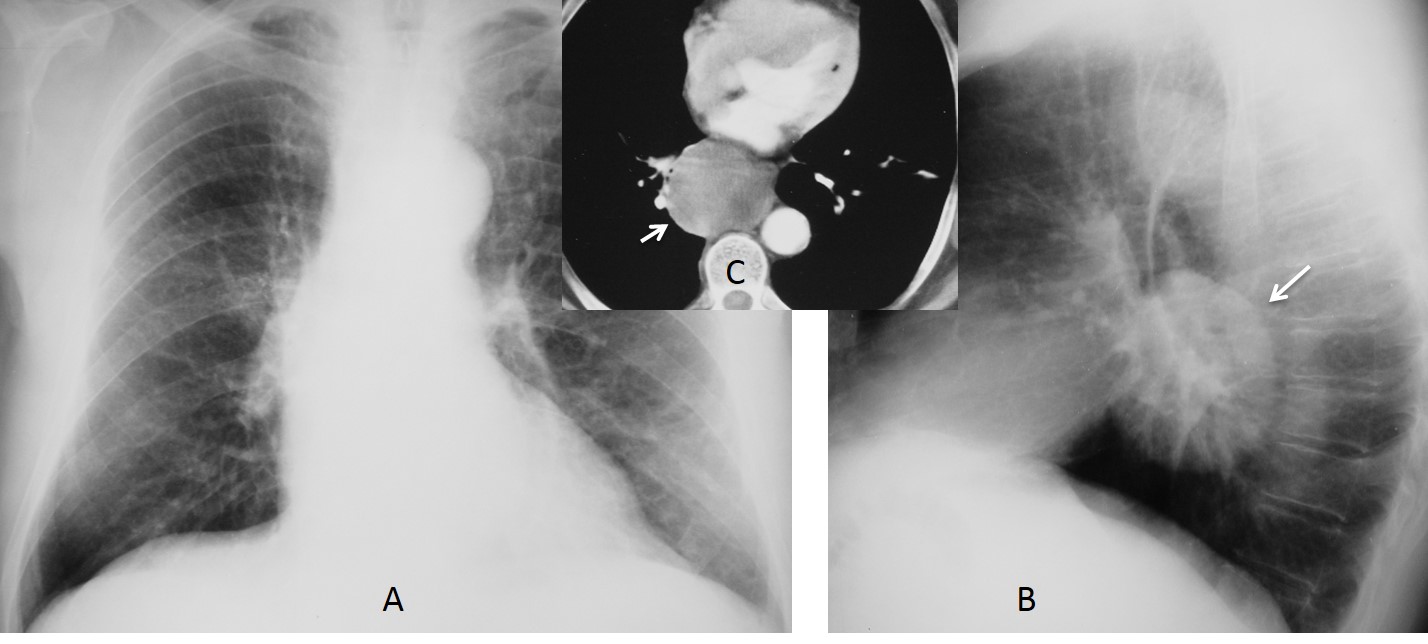
Fig. 7
Fig. 7: 35-year-old man, asymptomatic. The PA chest film (A) is unremarkable. The lateral view shows a large rounded lesion in the subcarinal region (B, arrow). Axial enhanced CT confirms a nonenhancing mass in the middle mediastinum (C, arrow). Diagnosis: congenital foregut cyst.
Due to previous infection or hemorrhage, duplication cysts may show high attenuation on CT, mimicking a solid mass. In such cases, MRI confirms the fluid content (Fig. 8).
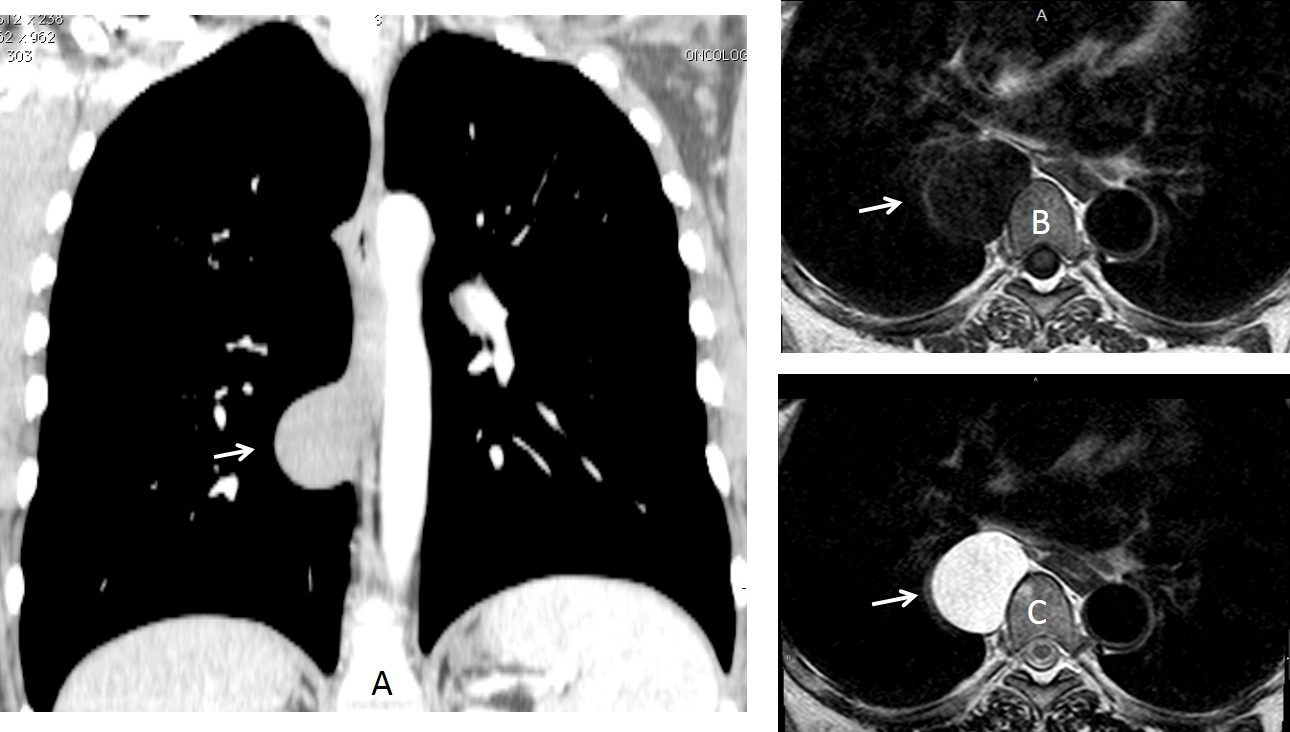
Fig. 8
Fig. 8: congenital duplication cyst mimicking a solid lesion on coronal enhanced CT (A, arrow). MR shows the typical appearance of a cyst in T1W and T2W images (B and C, arrows).
In rare cases, congenital cysts show a fluid-calcium level from milk of calcium. The diagnosis is easily made by placing the patient in prone position, which mobilizes the calcium sediment to the opposite wall, confirming the cystic nature of the mass (Fig. 9).
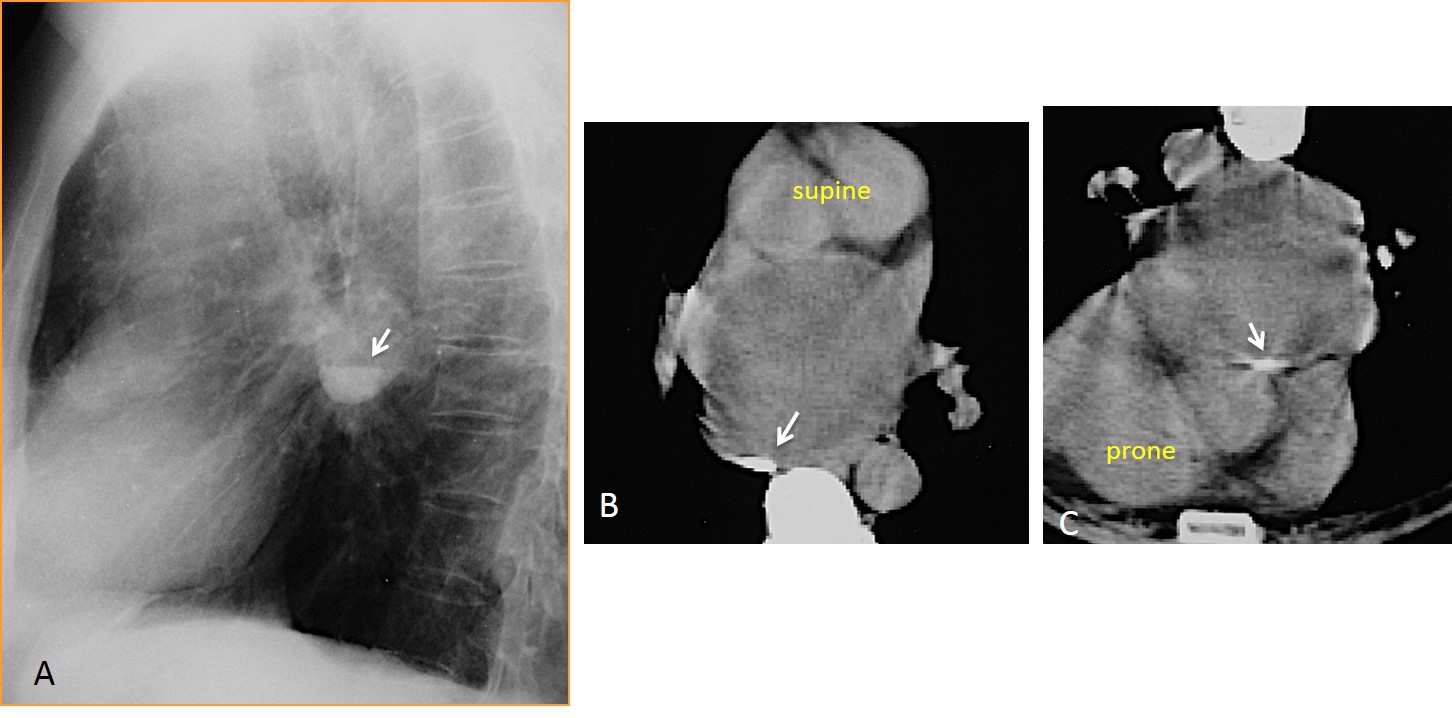
Fig. 9
Fig. 9: fluid-calcium level in a congenital cyst (A, arrow). In another patient, the milk of calcium flows from the back of the cyst in the supine position (B, arrow) to the front in the prone position (C, arrow).
By far, the most common condition occurring in the lower mediastinum is hiatal hernia, which affects about 10% of adults; the incidence increases with age. Hiatal hernia is easily recognized by visualization of the gastric air. A small percentage do not have visible air on chest radiography, and mimic a mass (Fig. 10). In rare cases, abdominal fat herniates through the hiatus; CT examination in then needed to confirm the diagnosis (Fig. 11).
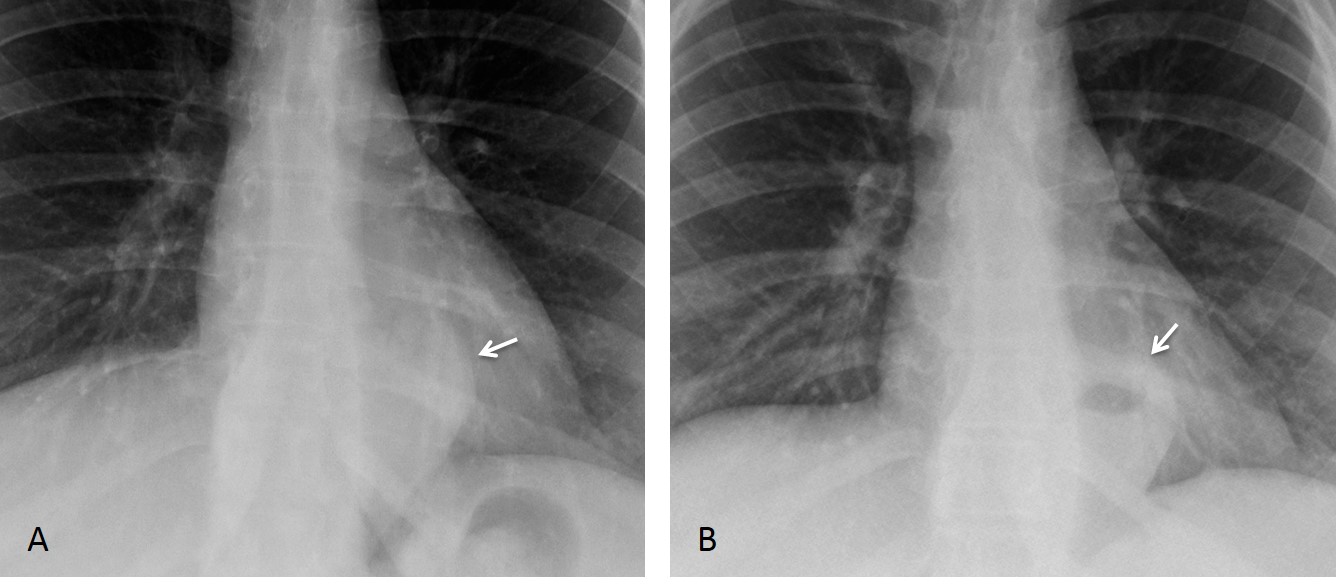
Fig. 10
Fig. 10: 50-year-old man with an airless hiatal hernia simulating a mass (A, arrow). A previous film shows an air-fluid level within the hernia (B, arrow), confirming the diagnosis.
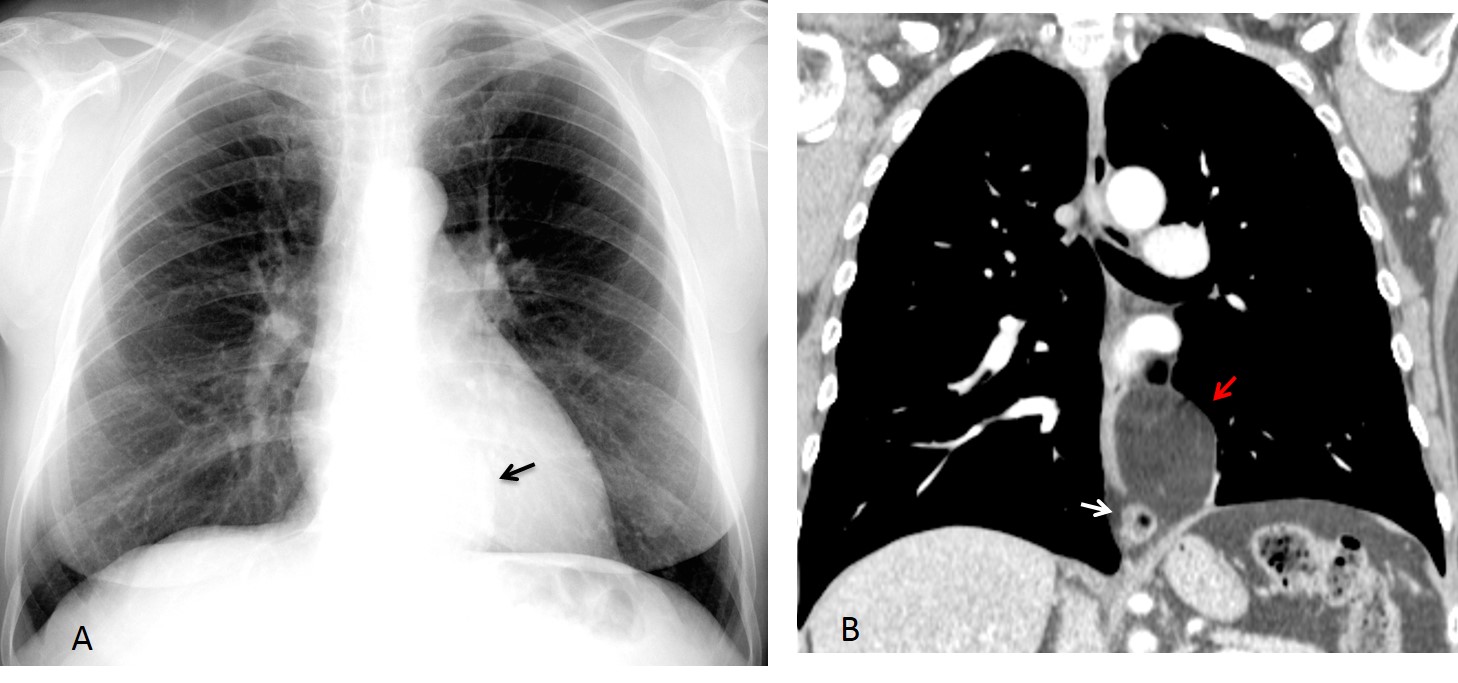
Fig. 11
Fig. 11: 54-year-old obese woman with a lower middle mediastinal mass (A, arrow). Coronal CT shows a small hiatal hernia (B, white arrow) and considerable herniation of abdominal fat (B, red arrow).
Occasionally, mediastinal varices in cirrhotic patients may appear as a lower middle mediastinal mass and simulate an airless hiatal hernia. The diagnosis is easily made with enhanced CT (Fig. 12).
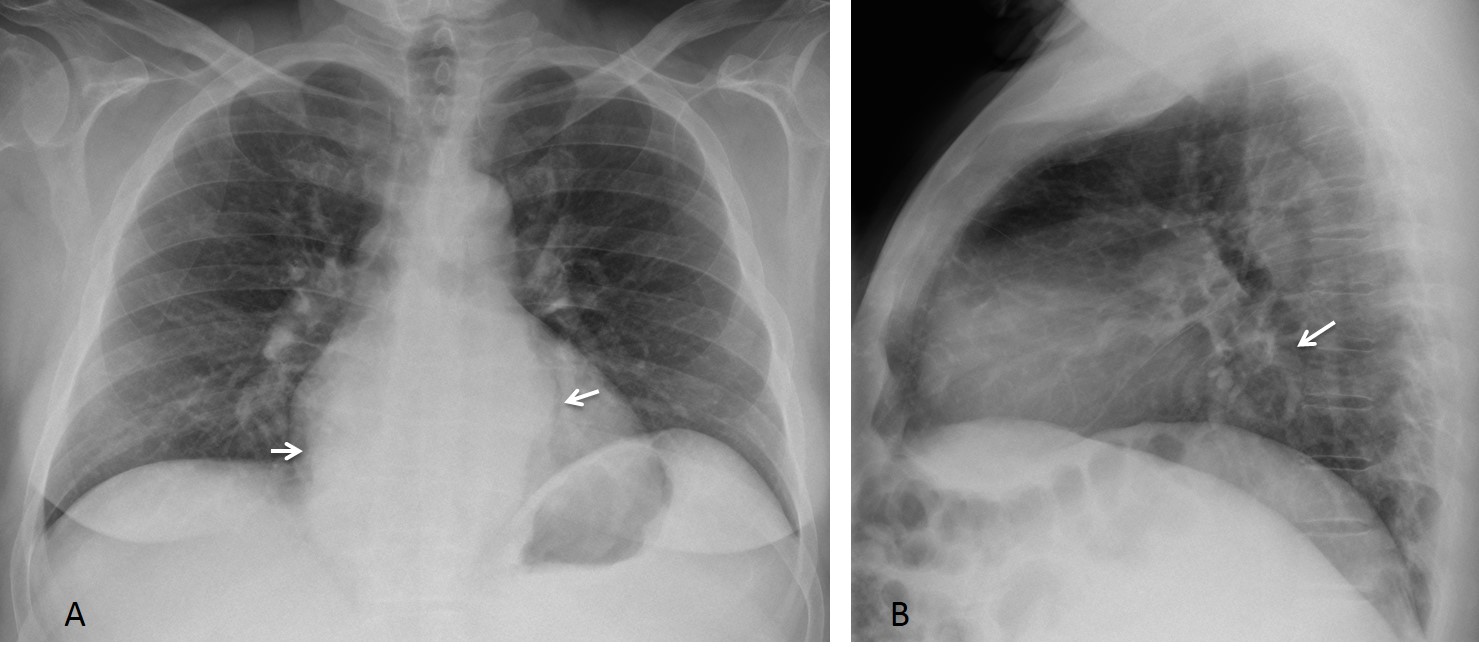
Fig. 12
Fig. 12: 58-year-old man with cirrhosis with a lower middle mediastinal mass simulating hiatal hernia (A and B, arrows).
Axial enhanced CT confirms large mediastinal varices (C and D, arrows). There is also splenomegaly and marked irregularity of the liver contour.
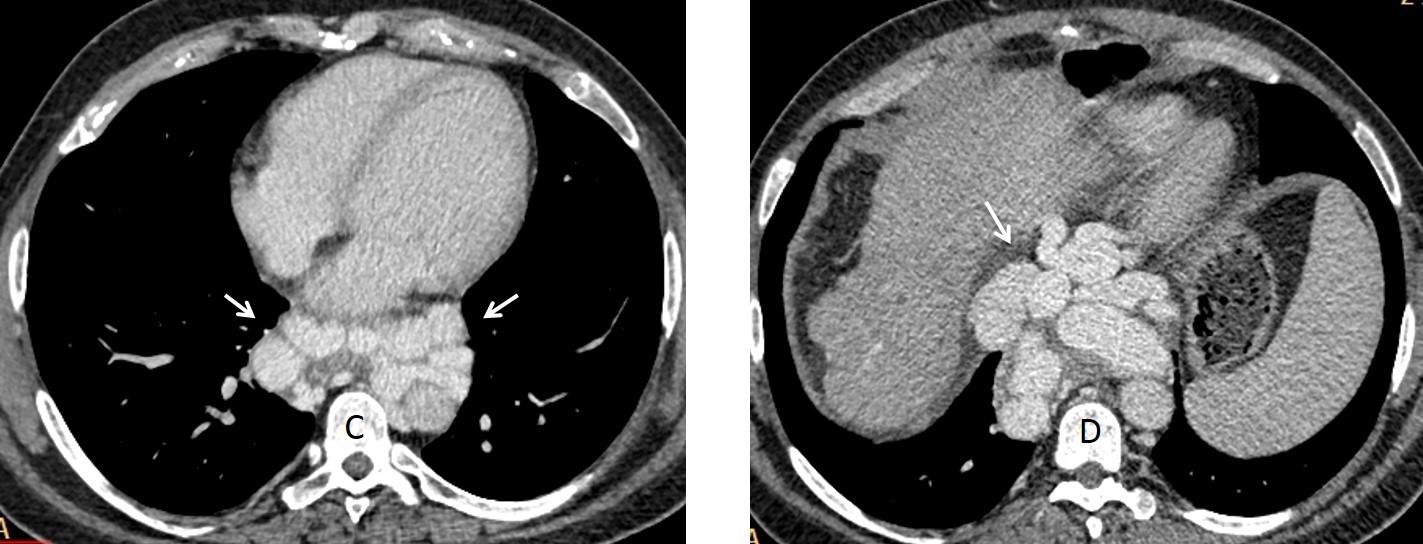
Fig. 12
It is important to remember that the esophagus lies in the center of the middle mediastinum, and that this structure may mimic a mass in any of the 3 subdivisions. A barium swallow clarifies the diagnosis (Fig. 13).
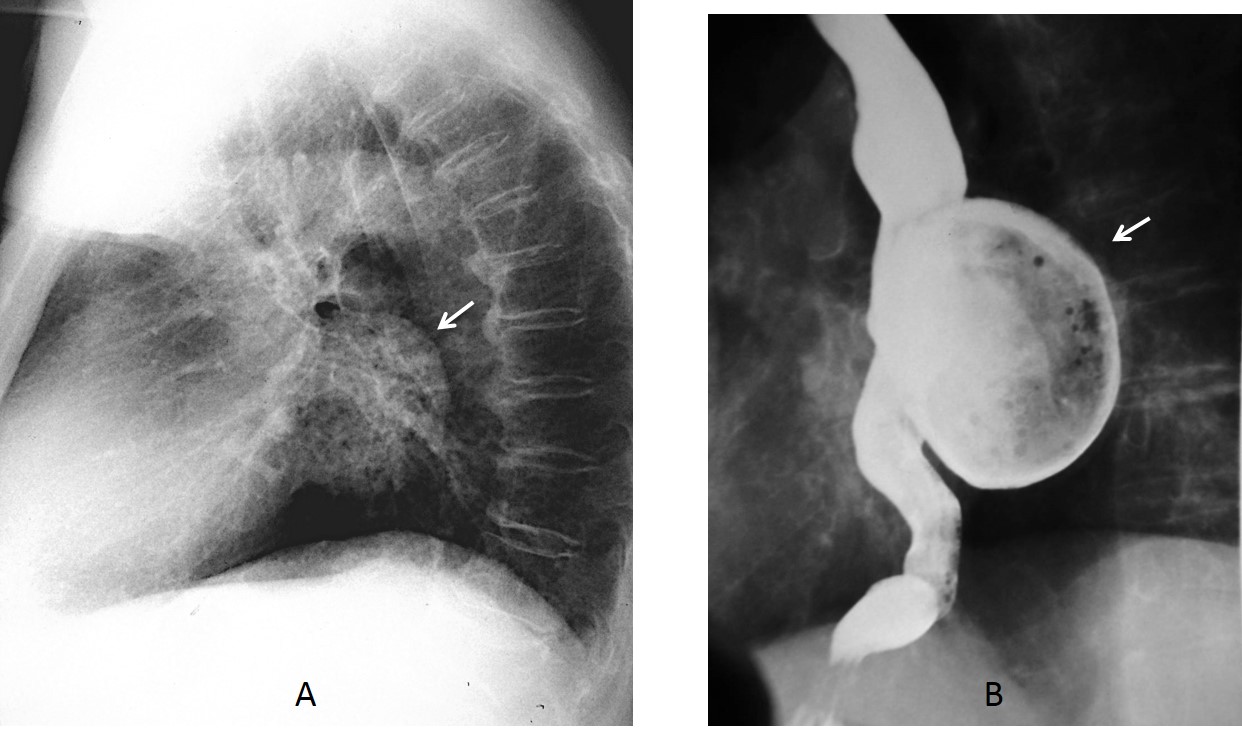
Fig. 13
Fig. 13: 75-year-old man with dysphagia and fetid breath. The lateral radiograph demonstrates a rounded mass in the middle mediastinum (A, arrow). Barium swallow confirms that the suspected mass is actually an esophageal diverticulum (B, arrow).
Follow Dr.Pepe’s Advice:
1. Most middle mediastinal masses represent enlarged lymph nodes or duplication cysts. Vascular structures and lesions arising in the esophagus should always be excluded.
2. The most common mass in the superior middle mediastinum is intrathoracic goiter.
3. Duplication cysts are usually located around the carinal area.
4. Lymph nodes usually affect the upper and middle compartments.
5. Hiatal hernia is the most common condition occurring in the lower middle mediastinum.


I say any of the above.
I think is difficult with out contrast to see the difference.
Especially if we cant see the rest of the CT slides.
Actually it’s a secret option 5. Vagus nerve schwannoma
Wow! Why I did’t think that?
Sarcastic response… Am I soo wrong or maybe soo close?
It was an honest response. I had not thought of this possibility.
Ok, honestly I’m a little relieved…
In my opinion the correct answer is esophageal leiomyoma.
May be mycotic aneurysm.
…la sede….le caratteristiche UH….la vicinanza senza piano di clivaggio, con la vicina aorta,,,,propendono x un aneurisma dell’aorta discendente
If the patient is allergeic to contrast, we can do MRI thorax instead.
4. Any of the above
You are correct. MRI was done.
Para nosotros , no es un aneurisma aortico porque en la TAC se puede ver el calcio intimal que no demuestra que este dilatada.
En cuando a un leiomioma esofágico, llama la atención que no presente síntomas de disfagia.
Por lo que la imagen retrocardíaca en el perfil de tórax y para aortico en la TAC podría corresponder a un quiste de duplicación esofágico.
Y la fiebre puede ser por una complicación del mismo.
Una discusión razonada. Respuesta el viernes.
…quella è la sede anatomica della v. azygos, che potrebbe essere dilatata, per disturbi di canalizzazione della VCI…
esophageal leiomyoma
The most probable – duplication cyst ( smooth shaped ,below carina, more often on the right side, in CT it shouldn’t be always fluid density, it can be soft tissue density ). Clinical symptoms due to bronchi compression, or infection itself. Differential diagnosis
in MRI.
Any of the above
thank you for case
Before posting the answer I want to thank you all for participating. The correct answer is saccular aneurysm. I honestly believe that the diagnosis cannot be made without contrast enhancement. Therefore, the best answer is 4. Any of the above.
Congratulations to Gus who was the first one.
….la probabile diagnosi puo’ pero’ essere avanzata sulla base delle caratteristiche TD, di base( UH identica a quella del lume aortico) e “mancanza” del piano di clivaggio con l’aorta….pertanto l’ipotesi diagnostica esatta è la 3….la 4 , per definizione , ha escluso l’ipotesi di un aneurisma che è invece indicata dal dott. Pepe….La Iuve sarà dura per il Barca, come io in questo caso….Saluti da Bari….
Dear friend, a native Englishman pointed to me that “Any of the above” included any of the possibilities offered. Therefore, aortic aneurysm is not excluded in the option nº 4.
Hope we see a good match on Saturday and Barça wins!
….carissimo e mitico professore….la palla è rotonda ed anche senza m.d.c si puo’ vincere la partita….saluti anche a lorenzo Bonomo altro mio caro maestro ed amico…
Post mediastinum soft tissue density lesion In right side of mediastinum with indistinct phase with aorta. Further evaluation with endoscopic USG.
any of above