Dr. Pepe’s Diploma Casebook: Case 84 – SOLVED!
Dear Friends,
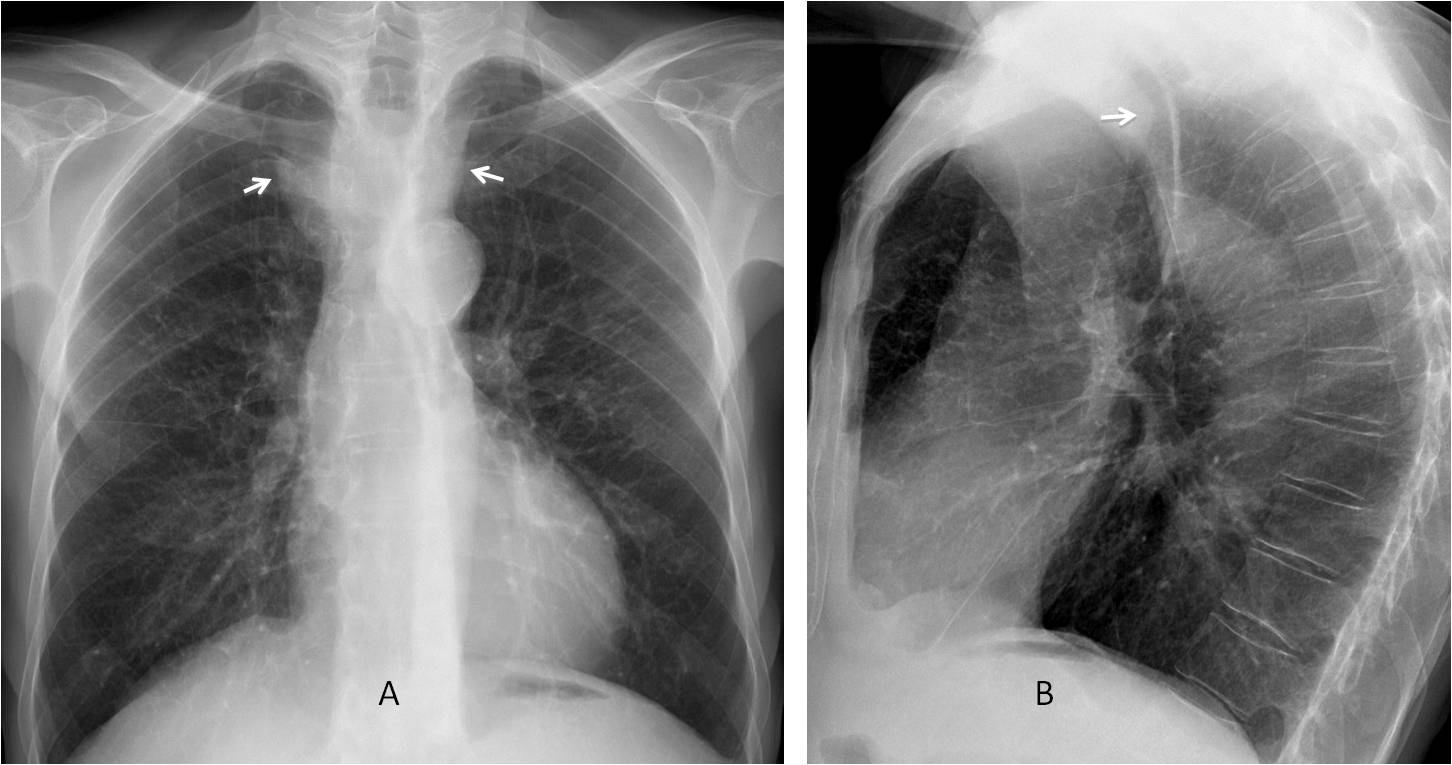
Today’s images belong to a 63-year-old man with moderate dyspnea.
What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.


Findings: PA radiograph shows widening of the upper mediastinum (A, arrows), which suggests tortuosity of the supra-aortic vessels. The lateral view shows marked narrowing of the trachea (B, arrow), apparently due to an anterior mediastinal mass.
Coronal and sagittal enhanced CT images show an aneurysm of the innominate artery (C and D, white arrows) compressing and narrowing the trachea (D, red arrow).

Final diagnosis: innominate artery aneurysm impinging on the trachea.
The trachea is a mid-line structure located in the upper middle mediastinum. Its air content makes it visible over the grey background of the mediastinal structures. In the conventional chest radiograph, tracheal displacement is a reliable basis to suspect a mediastinal abnormality.
The purpose of this presentation is to identify tracheal displacement in the PA and lateral radiographs and review the most common causes.
For diagnostic purposes, the trachea can be divided into two segments in the PA radiograph, cervical and intrathoracic, separated by an imaginary line drawn at the level of the clavicles.
In the PA radiograph, the trachea has a straight course. Deviation of the cervical trachea secondary to malposition of the head should not be confused with pathology (Fig. 1A). The intrathoracic trachea has an indentation in the lower left side caused by the normal left aortic arch. This indentation is more evident in aged patients (Fig. 1B).
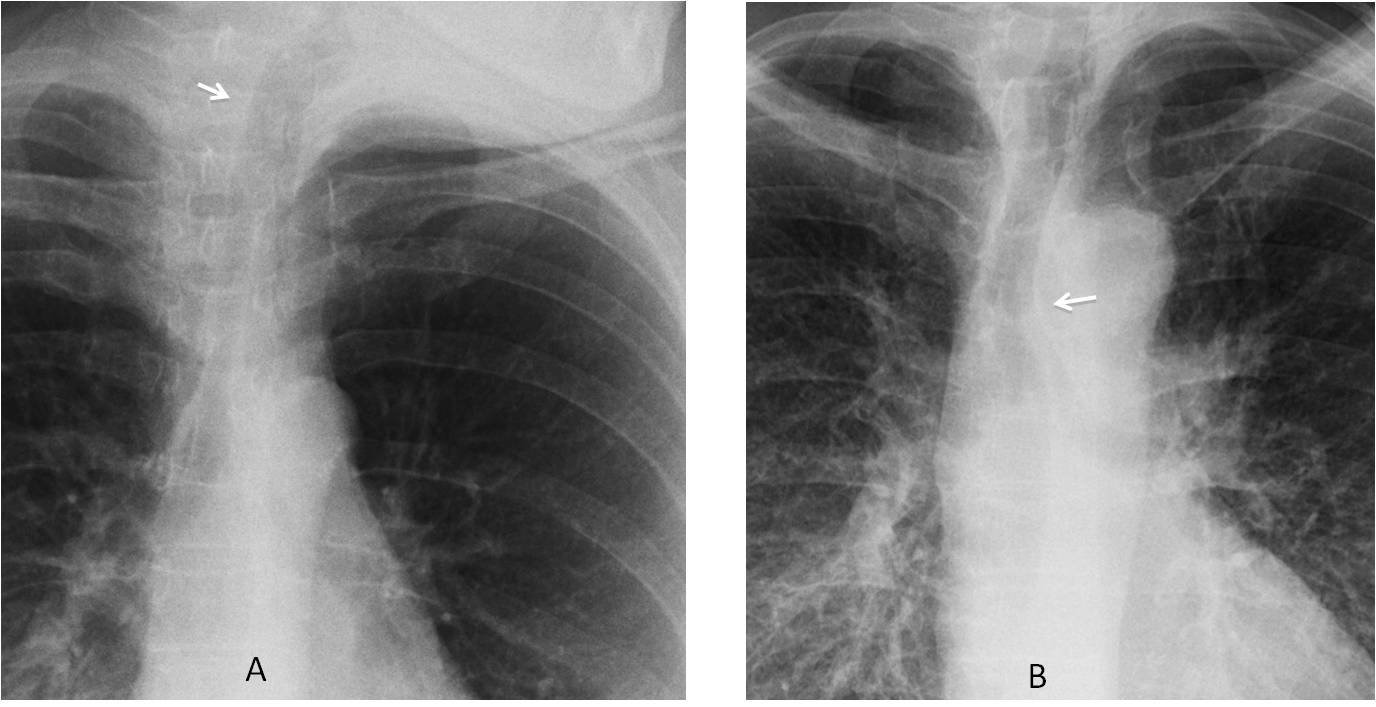
Fig. 1
Fig. 1: Displacement of the cervical trachea (A, arrow) due to malposition of the head. Note the mandible rotated to the left. B. Normal indentation of the lower trachea secondary to pressure from the aortic arch (B, arrow).
Considering that the thyroid gland surrounds the upper trachea, the most common cause of deviation of the cervical trachea is thyroid enlargement or a thyroid mass of any etiology (Fig. 2).
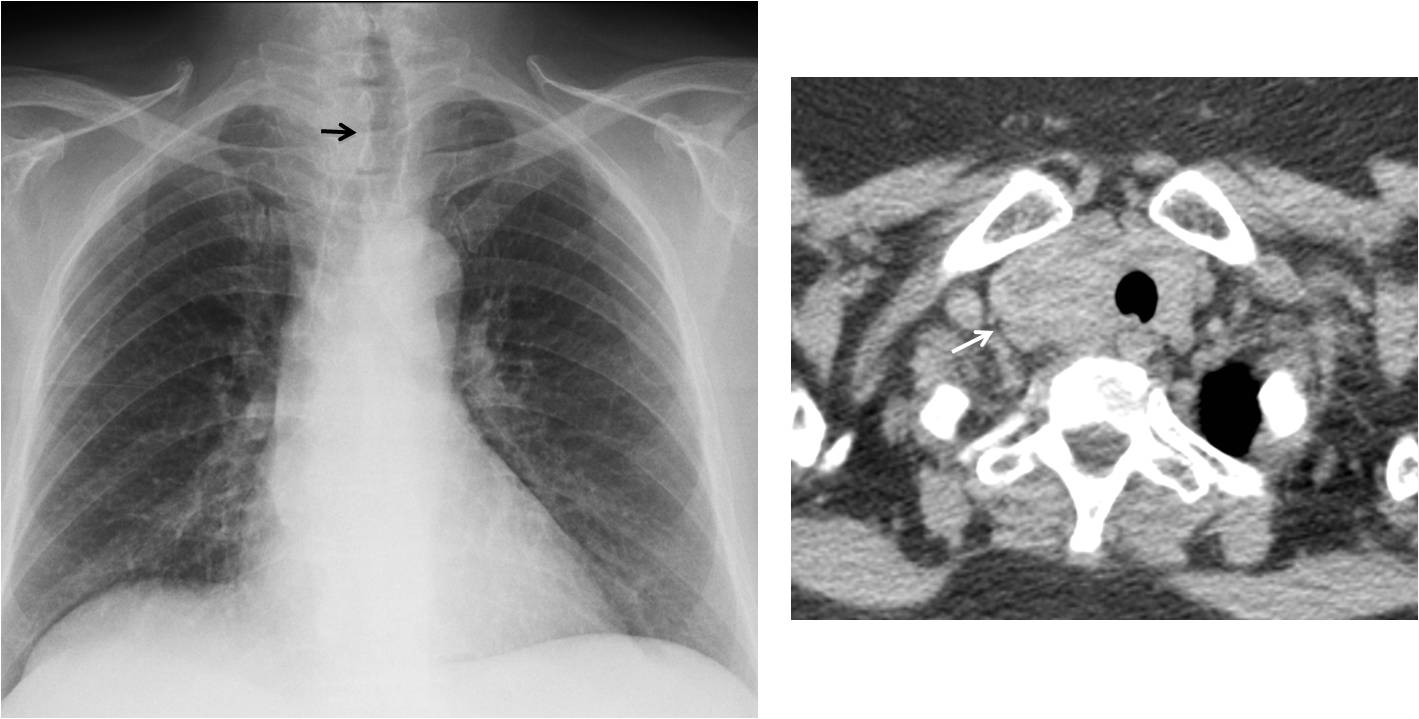
Fig. 2
Fig. 2: Displacement of the cervical trachea (A, arrow) in a patient with Grave’s disease. Axial CT shows enlargement of the right lobe of the thyroid (B, arrow).
Enlarged cervical lymph nodes are a less common cause of cervical trachea deviation, and a distant second to thyroid diseases (Fig. 3).
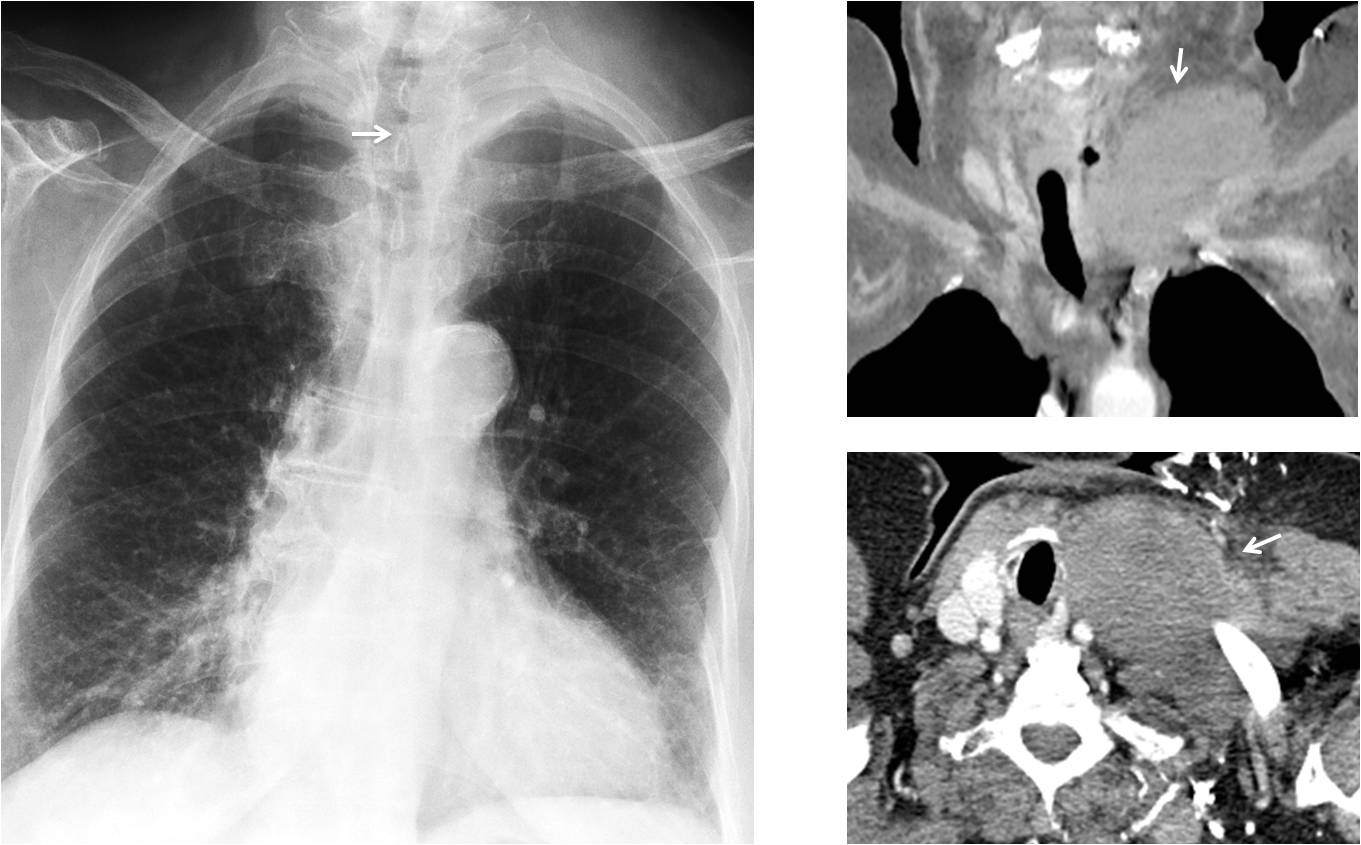
Fig. 3
Fig. 3: Slight displacement of the cervical trachea (A, arrow) in a patient with enlarged lymph nodes in the left supraclavicular fossa (compare with the right side). Enhanced coronal and axial CT show the matted lymph nodes (B and C, arrows). Diagnosis: lymphoma.
The most common causes of displacement of the intrathoracic trachea are aortic arch anomalies and mediastinal masses.
Type B right aortic arch with an aberrant left subclavian artery is the most common related vascular anomaly, occurring in 0.1 % of the population. It is easily suspected in the PA radiograph because the distal trachea is pushed to the left instead of the right, and the aortic knob is not in its normal location (Fig. 4). Double aortic arch has a more confusing appearance in the PA chest film and should be confirmed with enhanced CT (Fig. 5).
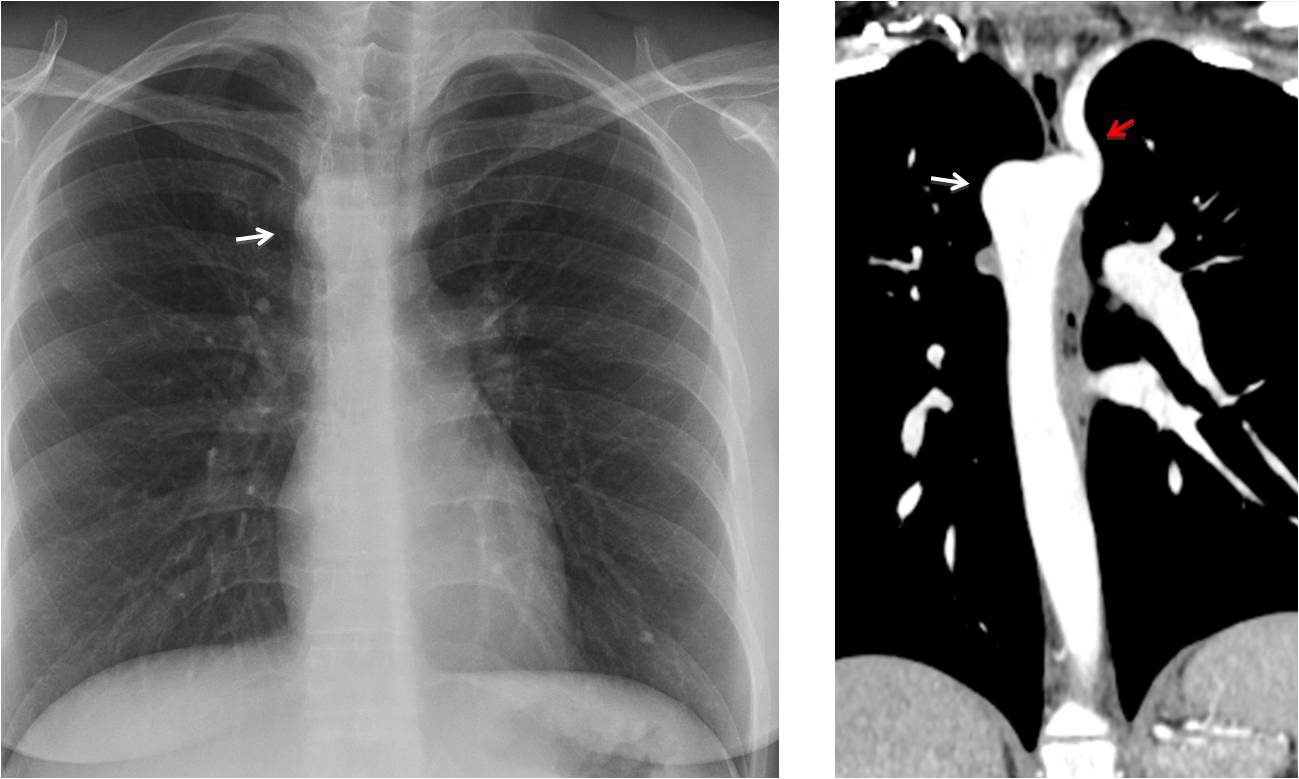
Fig. 4
Fig. 4: Type B right aortic arch with aberrant left subclavian artery. PA radiograph shows the aortic knob on the right side (A, arrow), pushing the trachea towards the left. No left aortic knob is seen. Enhanced coronal CT confirms the right aortic arch (B, white arrow) with the left subclavian artery arising as the last vessel (B, red arrow).
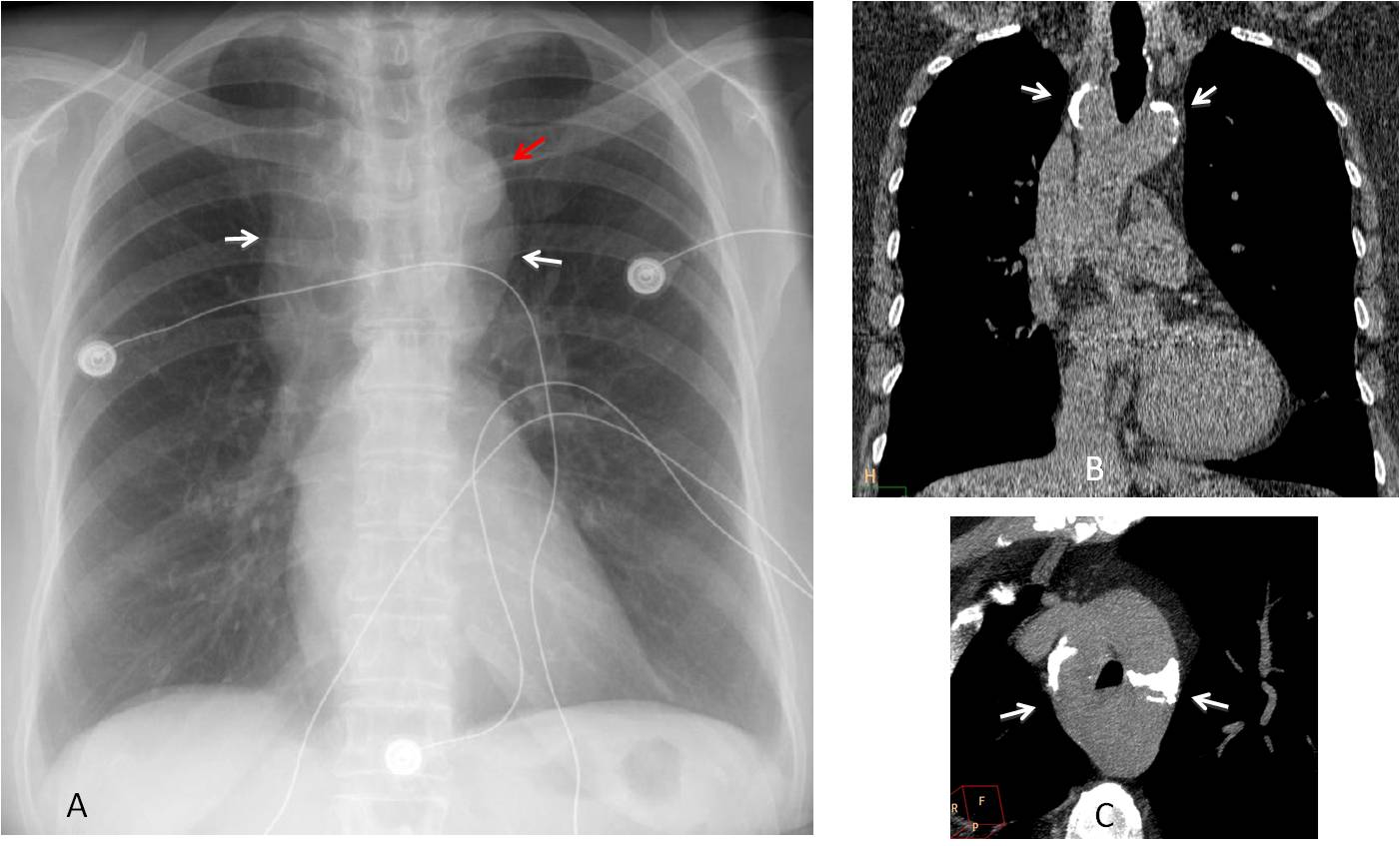
Fig. 5
Fig. 5: Preoperative film in a 57-year-old woman. PA radiograph shows a left aortic arch (A, red arrow), apparently surrounded by a mediastinal mass (A, white arrows). The trachea is in the midline. Unenhanced coronal and axial CT images show a calcified double aortic arch (B and C, arrows) surrounding the trachea.
Aneurysms of the aortic arch may displace the trachea and simulate a mediastinal mass. Enhanced CT should be done to clarify the diagnosis (Fig. 6).
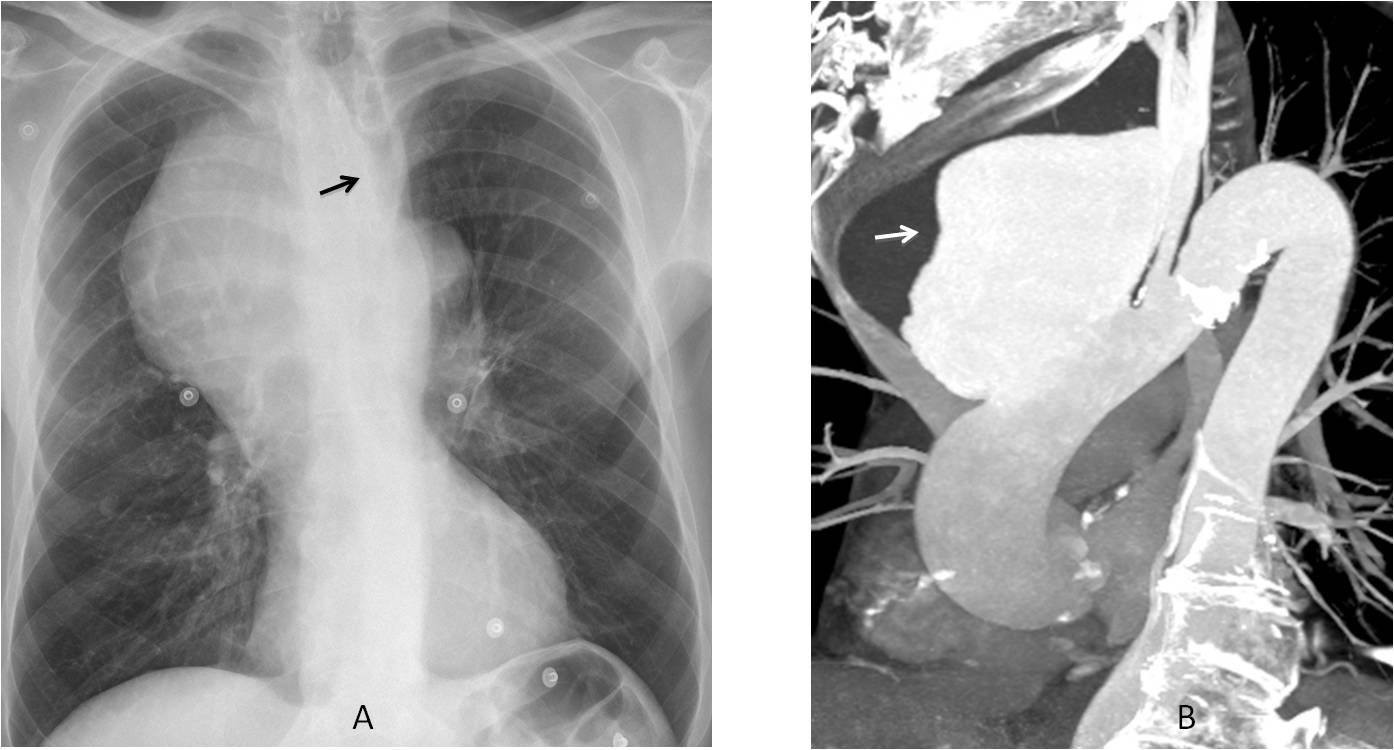
Fig. 6
Fig. 6: 54-year-old man with a large right mediastinal mass displacing the trachea towards the left (A, arrow). Enhanced oblique CT shows a large aneurysm arising from the anterior aortic wall (B, arrow).
Upper middle mediastinal masses may displace the thoracic trachea. Intrathoracic goiter is the most common of these, followed by enlarged lymph nodes. The diagnosis of goiter is easily confirmed by CT, which shows a high-density mass with marked early and prolonged enhancement after contrast injection (Fig. 7).
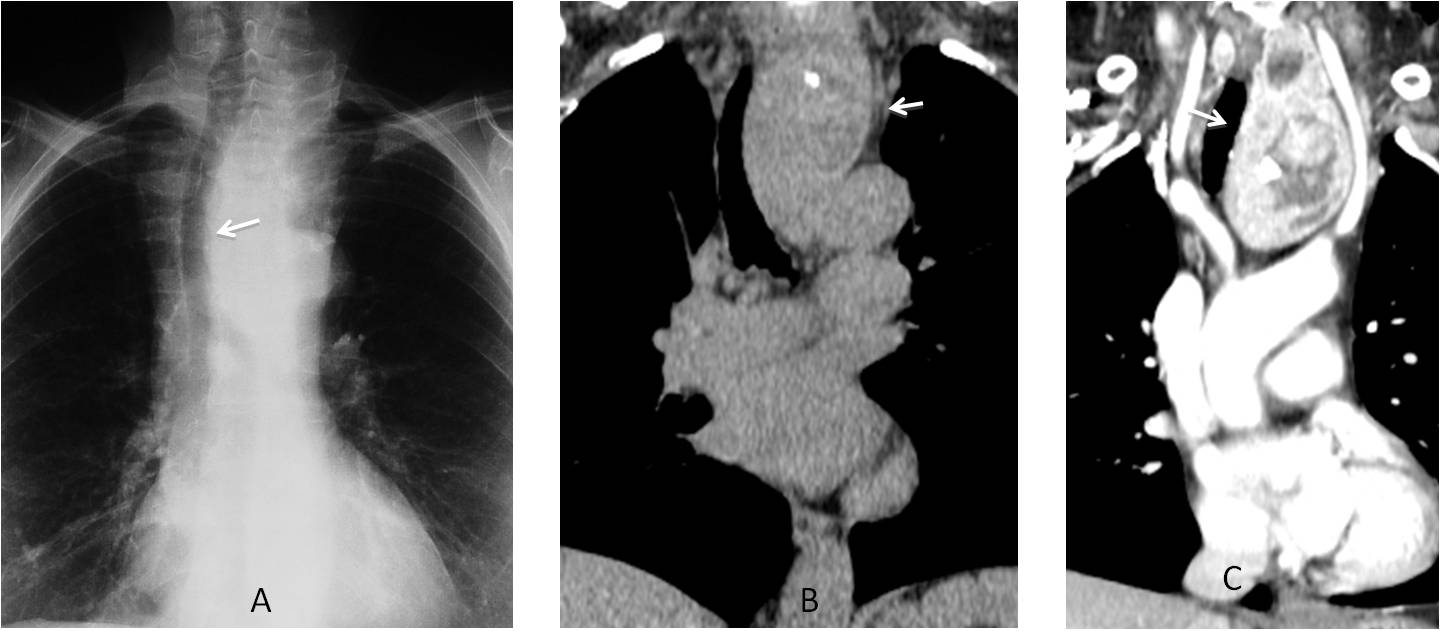
Fig. 7
Fig. 7: 47-year-old man with intrathoracic goiter. PA radiograph shows a mass displacing the trachea (A, arrow). Unenhanced CT confirms the mass (B, arrow). After contrast injection, the mass enhances markedly (C, arrow), confirming the diagnosis of goiter.
For practical purposes, only the intrathoracic trachea is visible in the lateral view. It is located approximately at the midline and has a straight or slightly oblique course depending on the body habitus.
Displacement of the trachea in the lateral view is important, especially when the PA view is unremarkable, as was seen in the first case of this presentation. Forward displacement is the most common and it occurs mainly in aortic arch anomalies and conditions affecting the oesophagus.
Most vascular conditions are related to a right or double aortic arch running behind the trachea and oesophagus. The imprint on the trachea may be subtle or obvious (Fig. 8). The vascular anomaly is usually seen in the PA view, although it may be overlooked (Fig. 9).
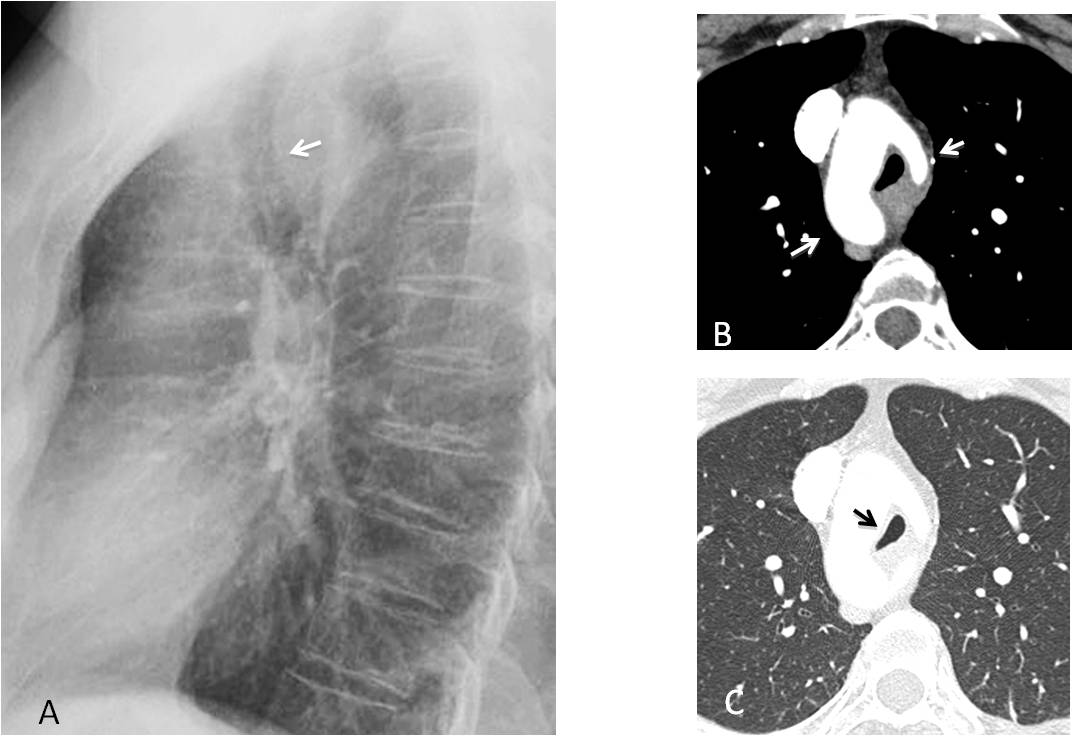
Fig. 8
Fig. 8: 45-year-old asymptomatic man with a posterior mass displacing the trachea forward (A, arrow). Enhanced axial CT shows an incomplete double aortic arch (B, arrows), narrowing the trachea (C, arrow).
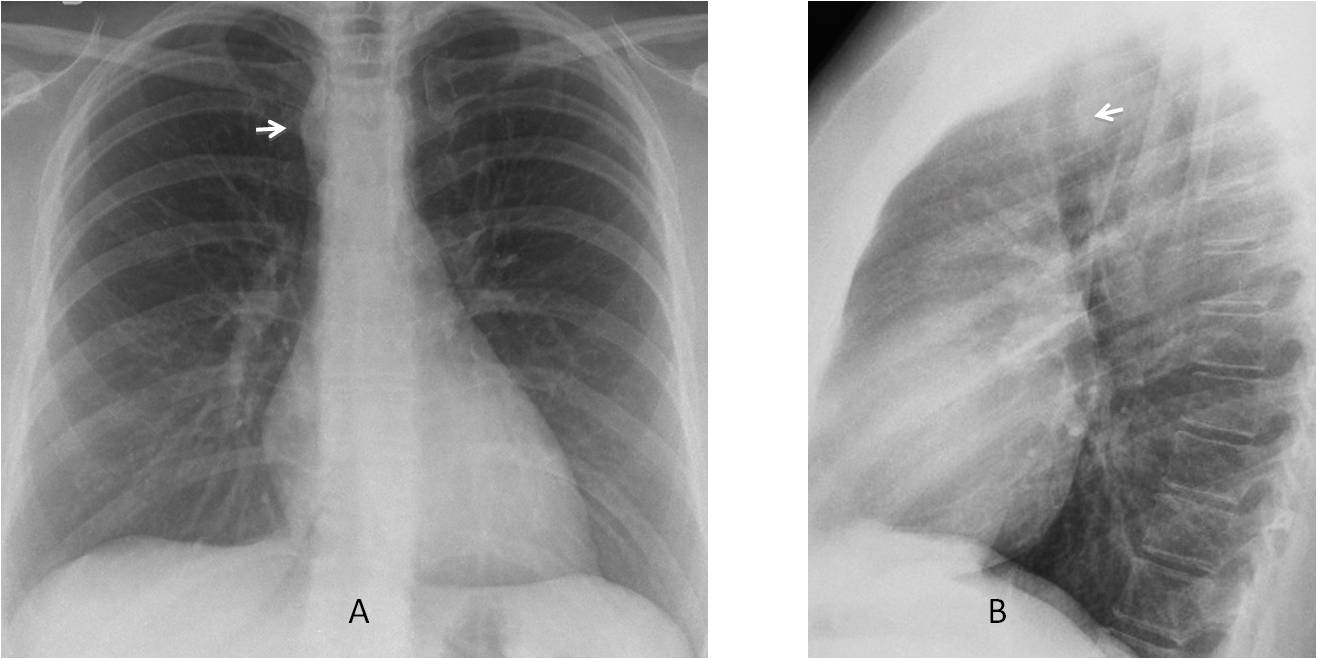
Fig. 9
Fig. 9: 27-year-old asymptomatic woman. There is a mild convexity at the right mediastinum (A, arrow), raising suspicion of a right aortic arch. Note that there is no visible left aortic knob. Lateral view shows a slight indentation in the posterior trachea (B, arrow).
Axial and coronal enhanced CT images confirm the right aortic arch (C and D, white arrows). The left subclavian artery (D, red arrow) arises from a large Kommerell diverticulum (C and D, asterisk).
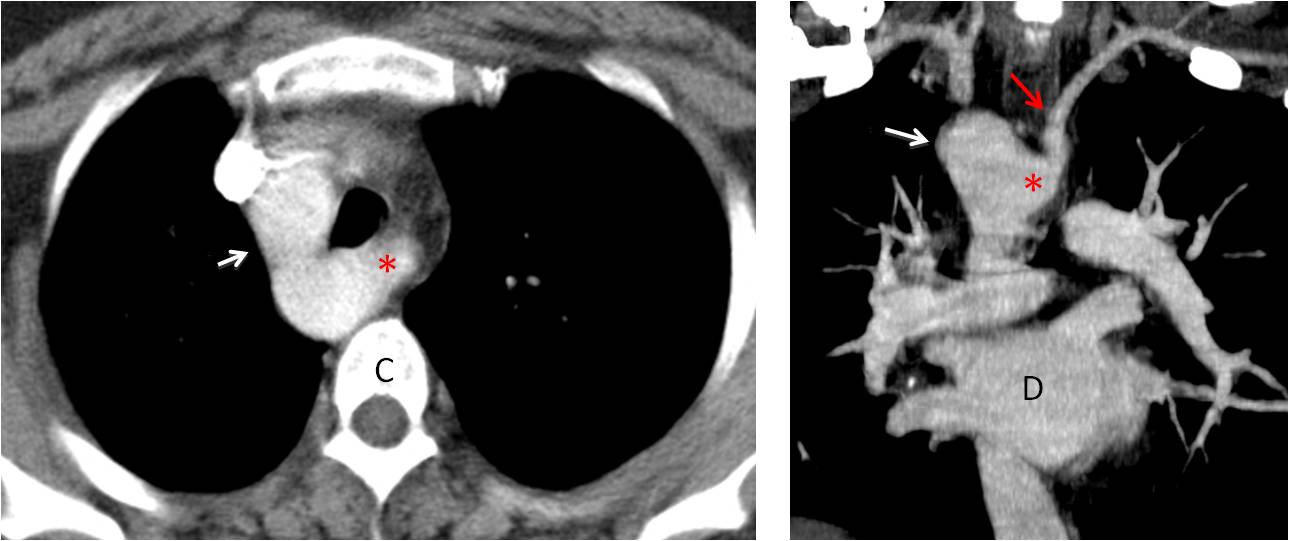
Fig. 9
Upper oesophageal conditions involve the retrotracheal space, pushing the trachea forward in the lateral view. The changes may be hidden by the mediastinum in the PA view (see Caceres’ Corner case #124). The most common offender is carcinoma (Fig. 10), although other pathologies may also be the cause (Fig. 11).
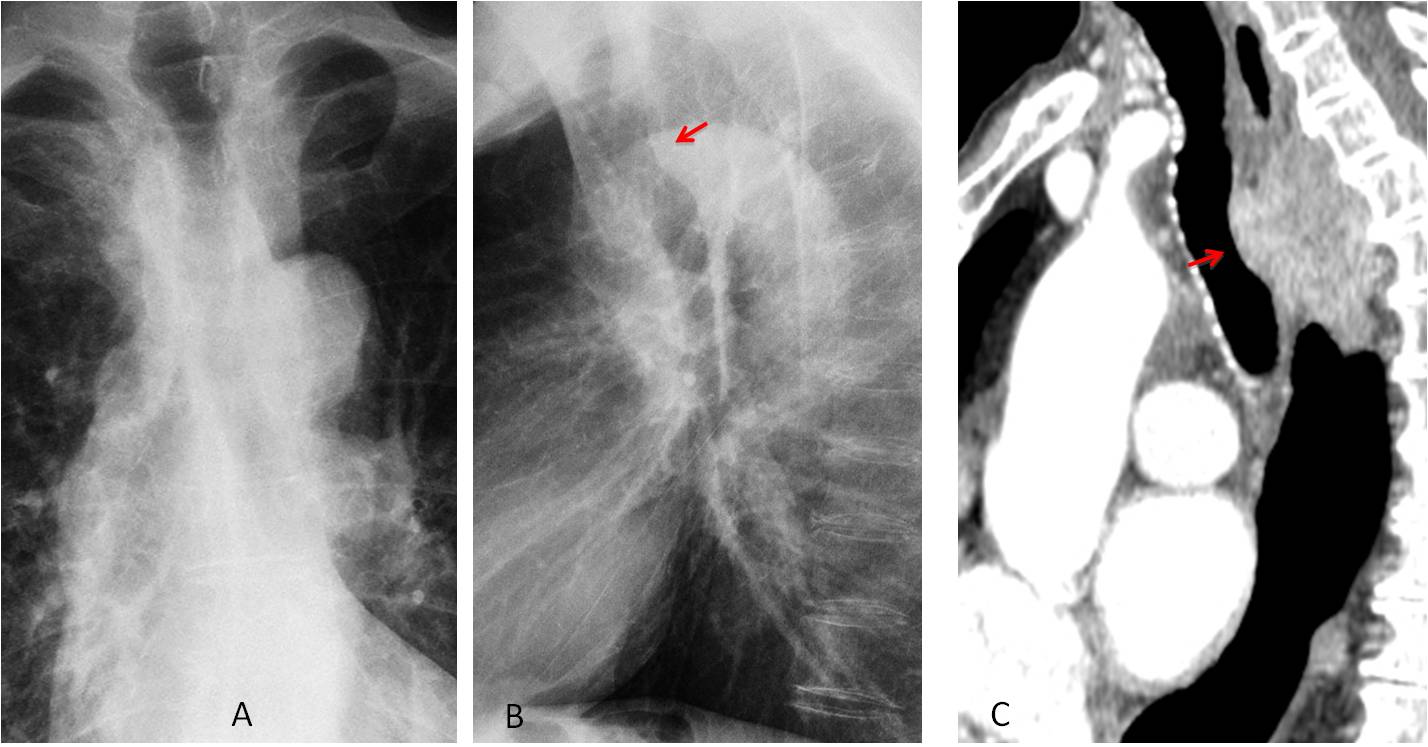
Fig. 10
Fig. 10: 65-year-old man with dysphagia. PA chest film (A) is unremarkable except for saber-sheath trachea. The lateral film shows compression of the posterior tracheal wall (B, red arrow). Sagittal CT shows a large mass behind the trachea (C, arrow). Carcinoma of oesophagus.
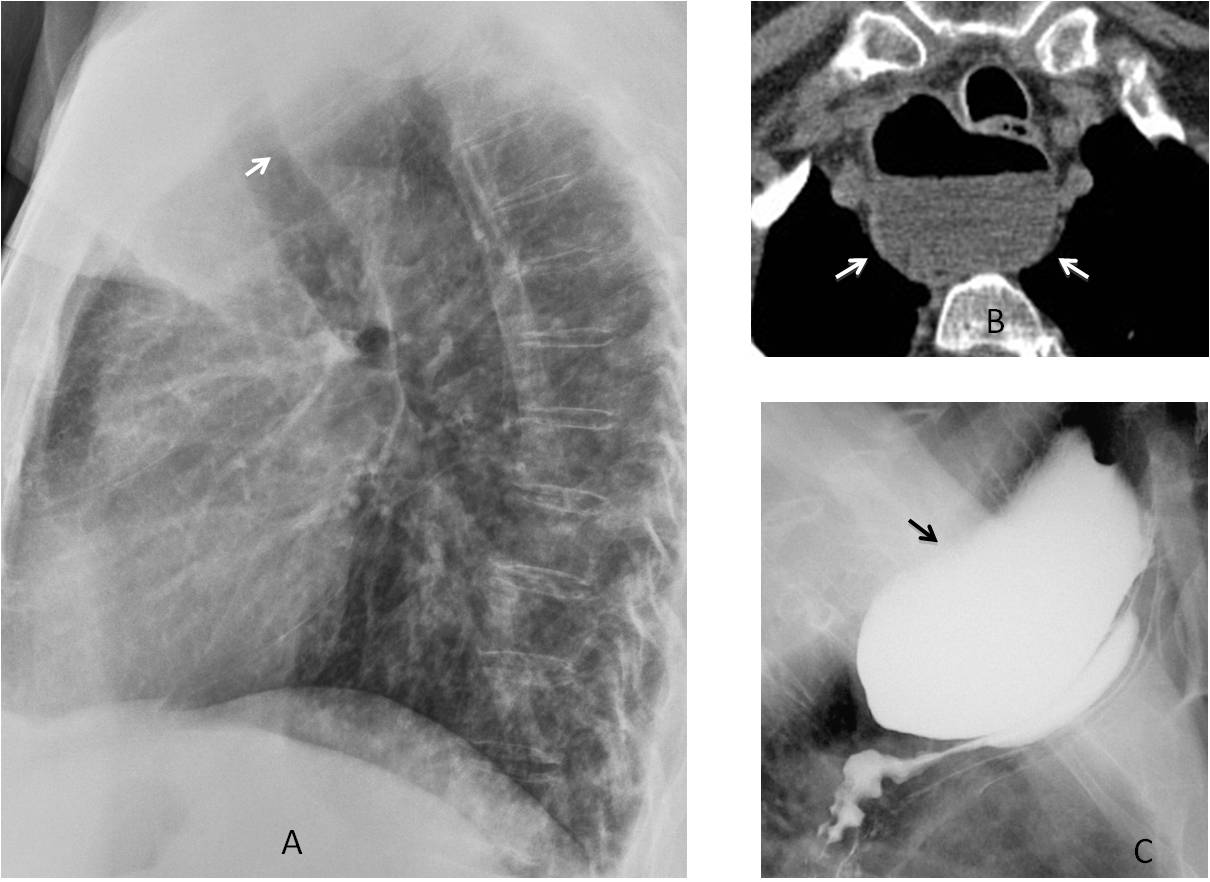
Fig. 11
Fig. 11: 58-year-old woman with recurrent pulmonary infections. Lateral view shows a retrotracheal opacity impinging on the trachea (A, arrow). Axial CT demonstrates a retroesophageal air-fluid level (B, arrows), confirmed to be a Zenker’s diverticulum after barium swallow (C, arrow). There is barium aspiration into the trachea.
It is not unusual for endothoracic goiters to be seen behind the trachea as a retrotracheal mass. It is interesting to note that the trachea may not be pushed forward, as the goiter is located lateral to the trachea. The diagnosis is mainly based on the PA view, which usually shows an obvious mediastinal mass pushing the trachea (Fig. 12).
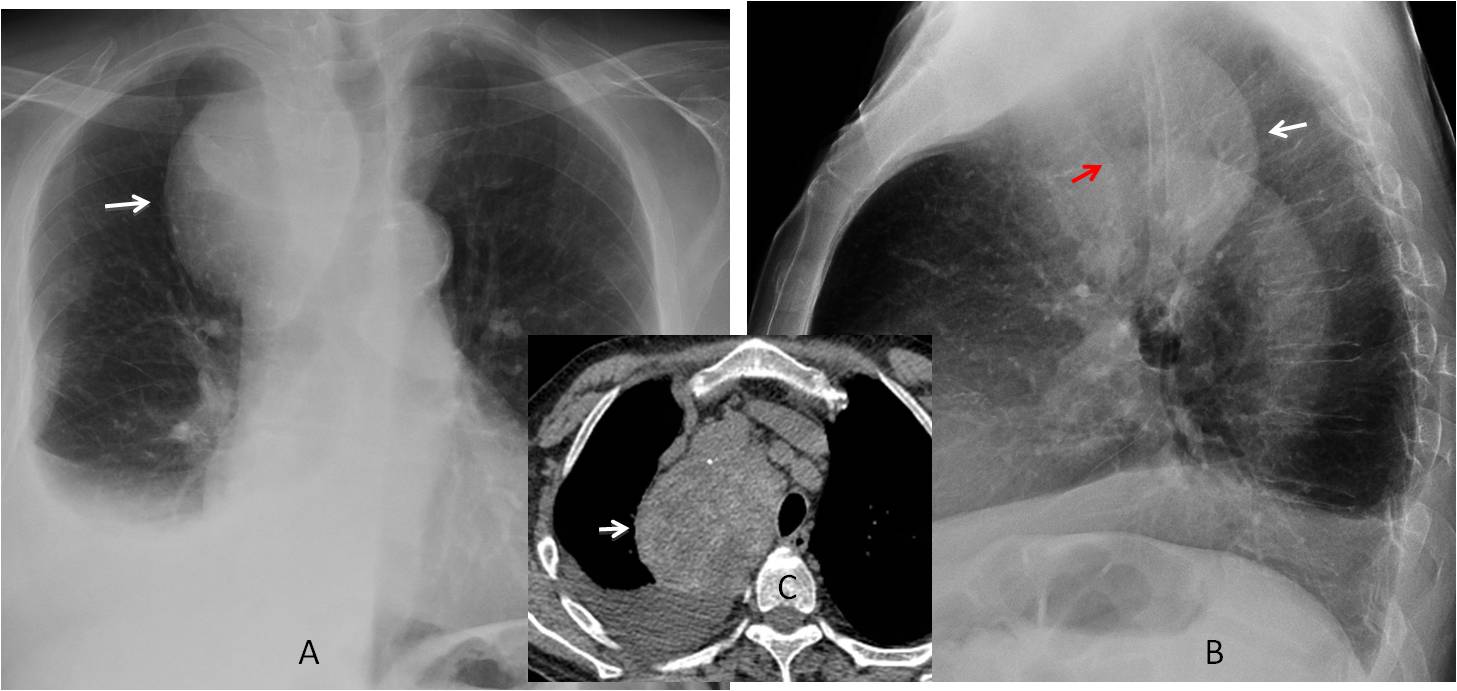
Fig. 12
Fig. 12: 56-year-old woman with an endothoracic goiter. The PA view shows an obvious upper mediastinal mass (A, arrow). Note that it appears as a retrotracheal mass in the lateral view (B, white arrow), although the trachea is not displaced forward (B, red arrow). Unenhanced sagittal CT confirms the diagnosis of a large goiter lateral to the trachea (C, arrow).
Follow Dr.Pepe’s Advice:
1. Always look at the trachea in PA and lateral views.
2. The most common cause of displacement of the cervical trachea is a thyroid mass.
3. Aortic arch anomalies or endothoracic goiter are the most common causes of displacement of the thoracic trachea in the PA view.
4. Anterior displacement of trachea in the lateral view is usually due to aortic arch anomalies or oesophageal conditions.


emphysema; a small aneurysm of ascending aorta
bronchiectasis + possible right inferior lobe mass
Expanding the superior mediastinum bilateral mostly right. On the lateral view the trachea is displaced anterior – may be – goitre.
Sorry – the trachea is displaced posterior.
Rt paratracheal round opacity – ?dilated azygos
Ascending aortic aneurysm
…vi è una patologia espansiva nel mediastino superiore che in AP deborda dal profilo mediastinico superiore dx “oscurando” l immagine tracheale…..quest’ultima in LL è improntata anteriormente ,e sospinta in dietro…..non è un gozzo intratoracico….la TC chiarirà la patologia….
Anterior-superior mediastinal mass, could be tymoma, lymphoma, substernal goiter….there is visible trahea compression
Golden S signe-right uporem Łobez colaps due to tu probably
Right upper lobe i ment
…penso che “anche” questo caso sia stato già pubbilicato! Aneurisma aorta ascendente ….
Congratulations to all of who made the right observation (posterior displacement of th trchea in the lateral view)
aortic aneurysm.