Dr. Pepe’s Diploma Casebook: Case 88
Dear Friends,
This week’s case follows the pattern of a “Meet the Examiner” presentation, with questions and answers similar to a real examination. Take your time before scrolling down for the answer. And no peeking!
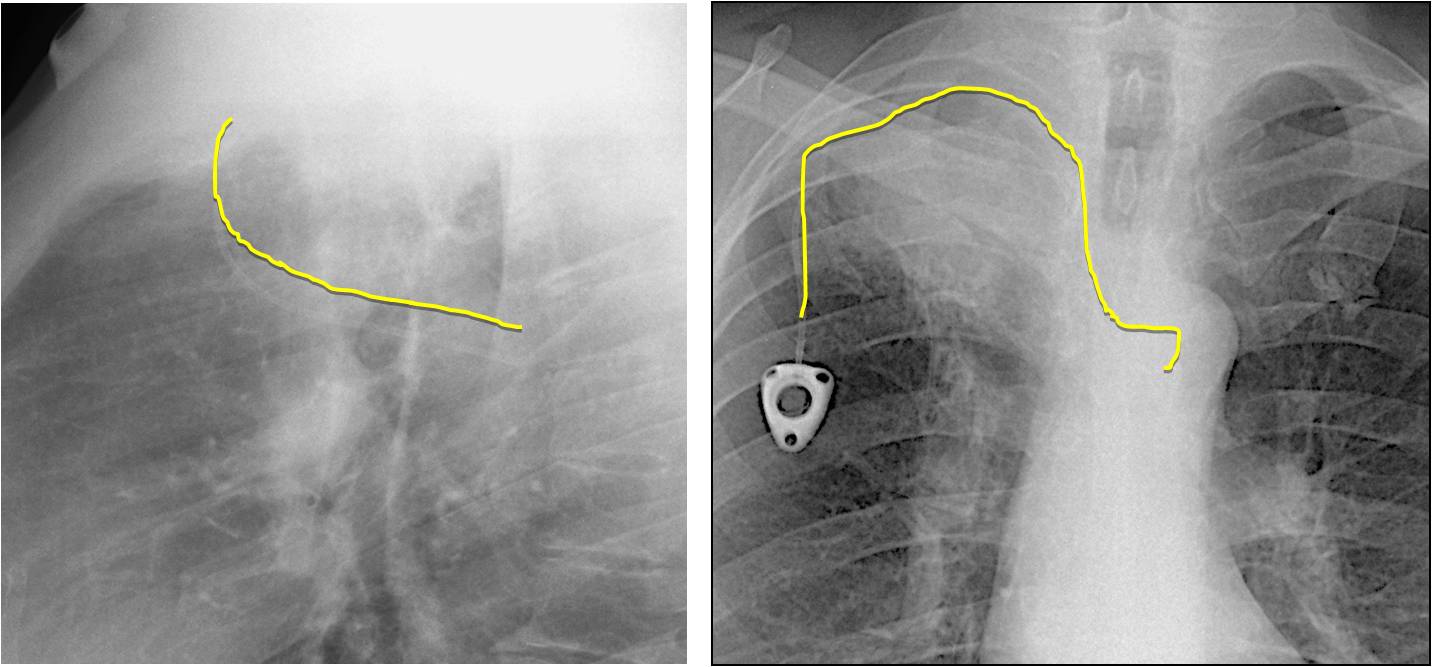
The chest radiographs belong to a 54-year-old man in treatment for RUL carcinoma.
What do you see?
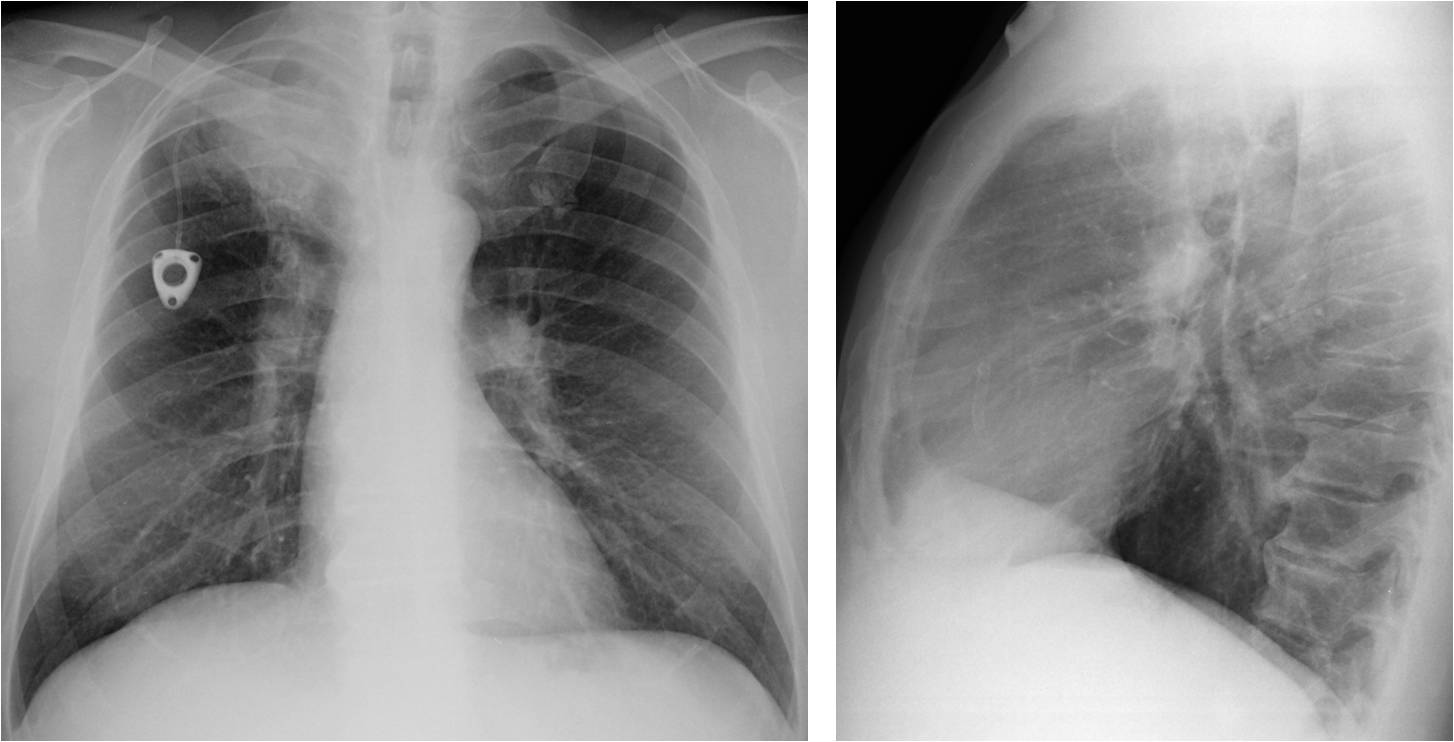
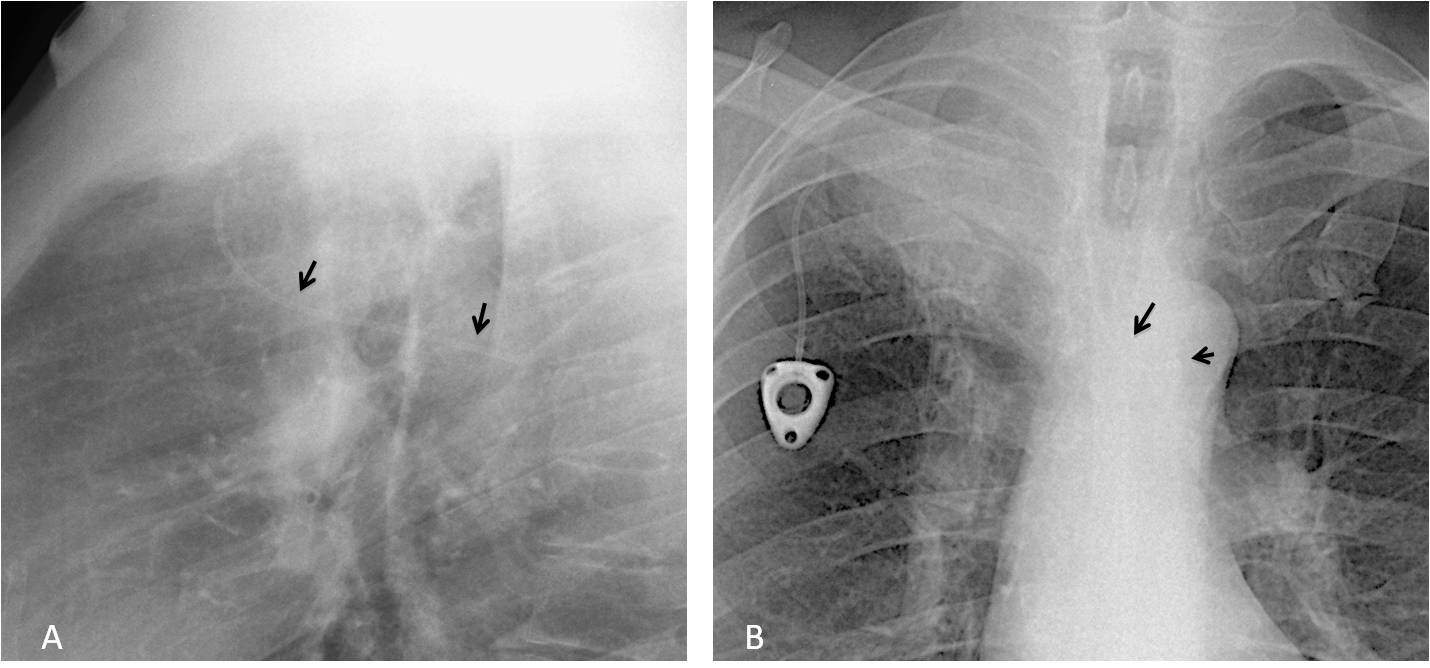
Aside from the obvious RUL carcinoma, the most relevant finding is an abnormal path of the port-a-cath, clearly seen in the lateral view (A, arrows). In the PA view the catheter is barely visible crossing the midline and turning sharply downwards (B, arrows). Where do you think the catheter is?
1. Azygos vein
2. Left superior vena cava
3. Internal mammary vein
4. None of the above
The horizontal trajectory in the lateral view excludes the left superior vena cava and mammary vein, which are anterior vertical structures. The crossing of the midline goes against placement in the azygos vein, which is a right-sided structure.
The correct answer is: 4. None of the above.
Coronal, axial and sagittal CT images show that the catheter has been placed inadvertently in the right subclavian artery (A-C, red arrows). It then traverses the aortic arch and ends in the proximal descending aorta (A-C, yellow arrows). Note the opacified subclavian vein (A and B, white arrows).
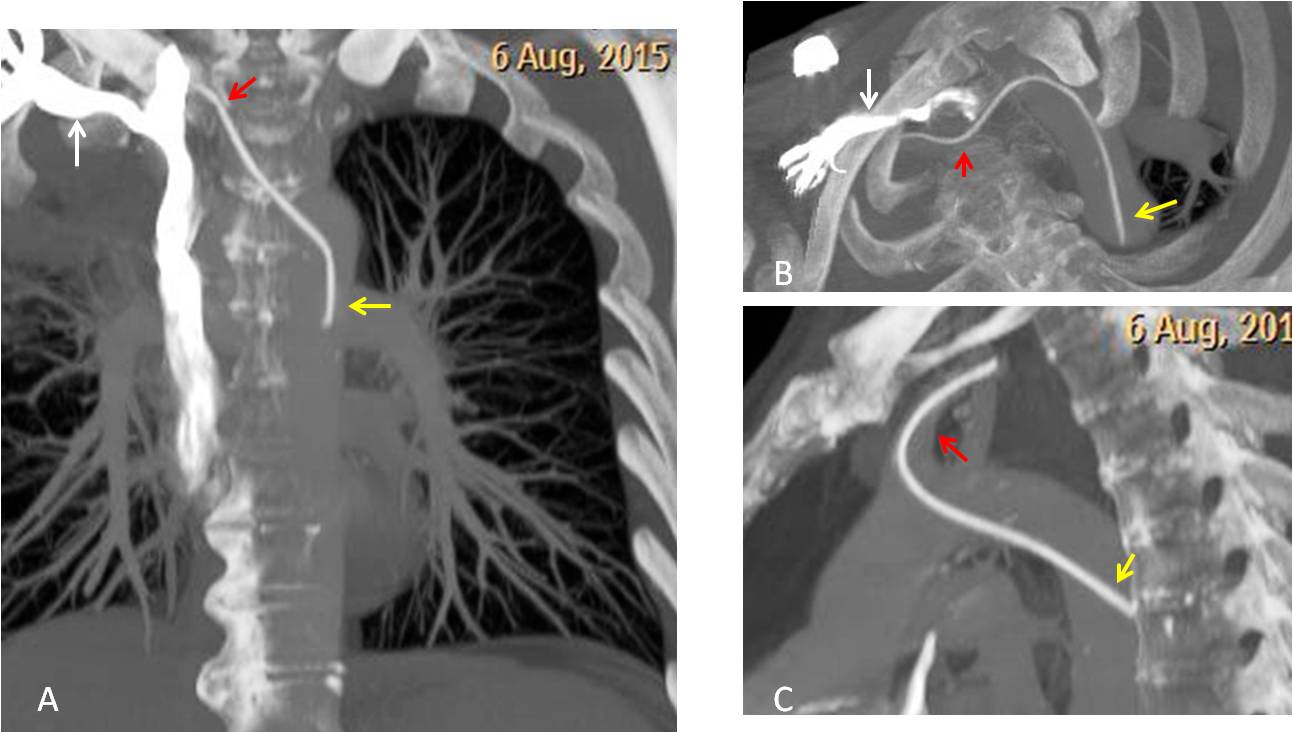
Final diagnosis: Inadvertent placement of the port-a-cath into the arterial system.
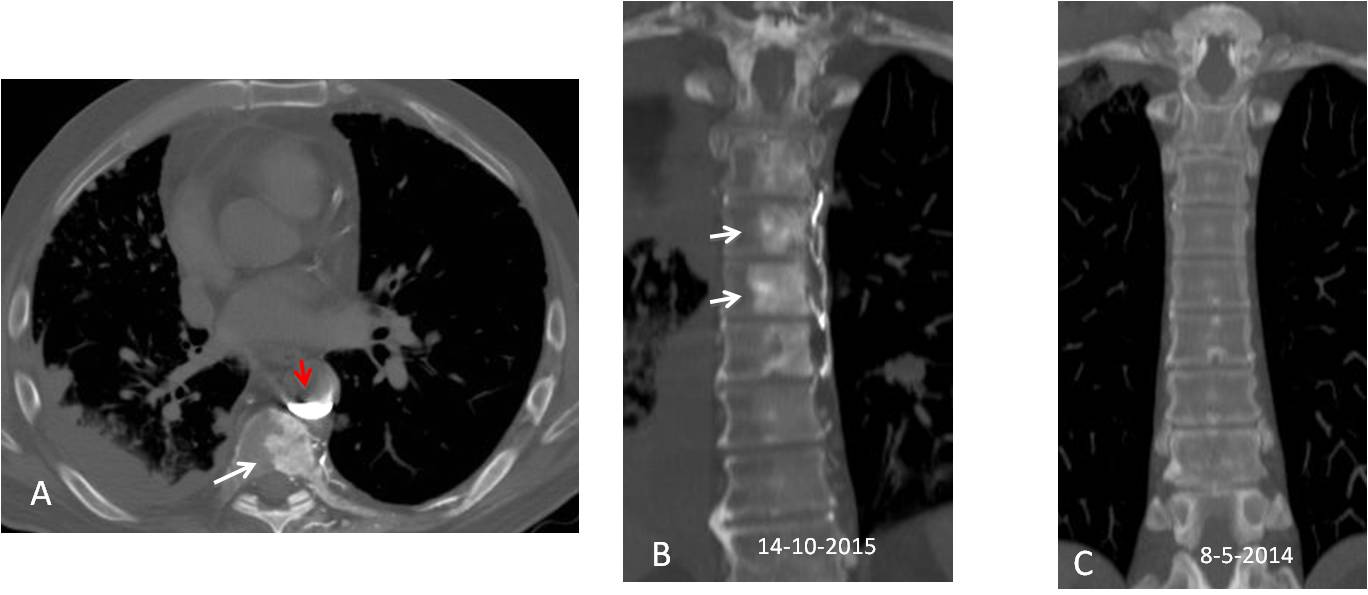
Injection through the catheter confirms that contrast material pools in the descending aorta (A, red arrow). An unexpected finding is an osteoblastic area in the adjacent vertebra (A, white arrow). Coronal reconstruction shows sclerotic changes in several vertebrae (B, arrows), which were not present 17 months before (C).
Would you say that the patient has osteoblastic metastases?
This patient has what is known as vanishing bone metastases(*). These are areas of increased vertebral density secondary to enhancement of the vertebral venous plexus, mainly reported in patients with SVC obstruction. In our patient, the enhancement was secondary to direct contrast injection into the arterial system.
It is important to be aware of this pitfall to avoid making a false diagnosis of osteoblastic metastases.
(*) Vanishing bone metastases : a pitfall in the interpretation of contrast enhanced CT in patients with superior vena cava obstruction. N Thomas et al
The British Journal of Radiology, 84 (2011), e176–e178

Follow Dr.Pepe’s Advice:
1. Add the arteries to the list of places where IV catheters may go.
2. Contrast enhancement may give a false impression of osteoblastic vertebral metastases, mainly in patients with SVC obstruction.

