Dr. Pepe’s Diploma Casebook: Case 92 – SOLVED!
Dear Friends,
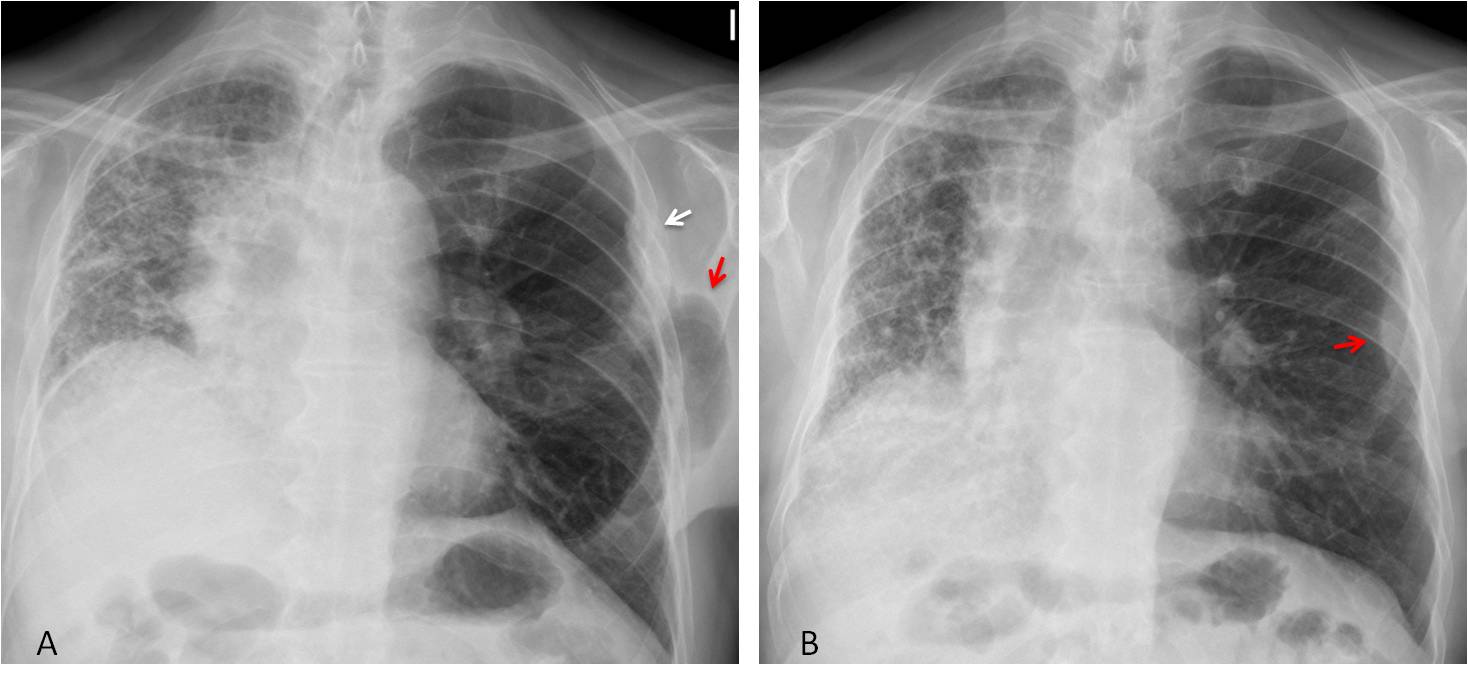
Today I am showing radiographs of a 62-year-old man with moderate dyspnoea. No acute symptoms. What do you see?
Check the images below, leave me your thoughts in the comments section, and come back on Friday for the answer.


Findings: There is a marked disparity in size of the lungs, secondary to a left lung transplant. Note the surgical fracture of the left 4th rib (A, arrow). A rounded collection of air overlaps the left rib cage (A, red arrow). PA radiograph in full inspiration shows that the pocket of air has disappeared and in its place there is protrusion of extrapleural fat (B, red arrow). The appearance is similar to Caceres’ Corner case 89.
Unenhanced axial CT shows postsurgical thinning and widening of the intercostal space (C, arrow). Coronal CT confirms herniated lung into the same space (D, arrow).
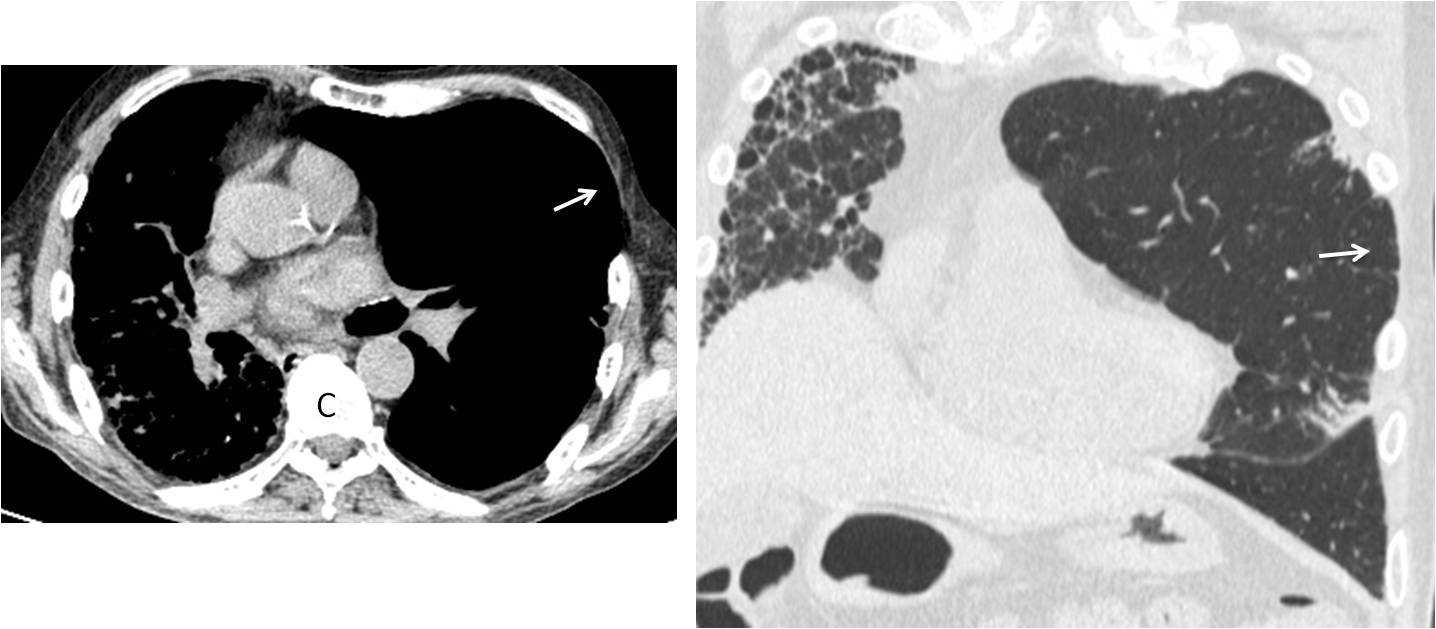
Final diagnosis: left lung transplant and associated pulmonary hernia.
I am presenting this case to discuss air in the chest wall. Its most common form of presentation is subcutaneous emphysema. The radiographic appearance is typical, appearing as streaks of air between the fascia planes and muscle bundles. The amount of air can vary from scarce to massive (Fig. 1).
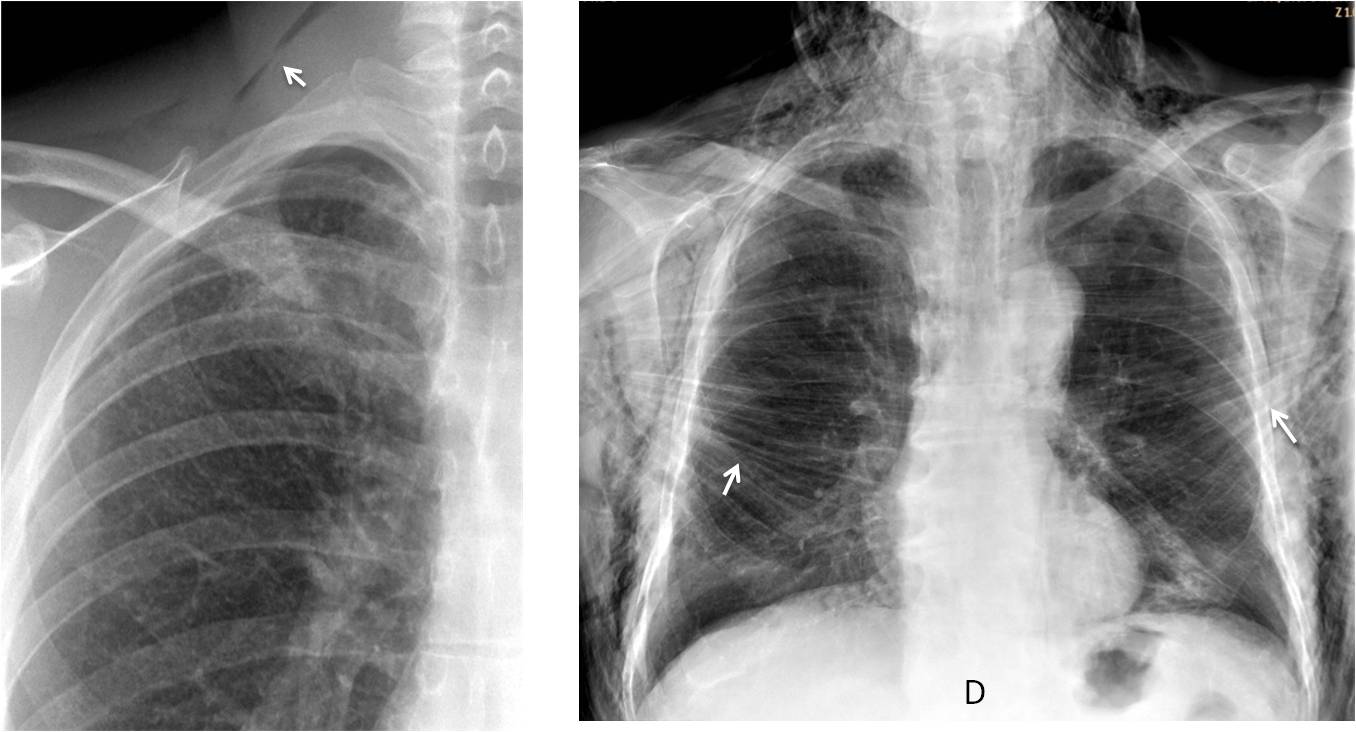
Fig. 1
Fig. 1: Radiographs of two patients after percutaneous lung biopsy. The first has a sliver of air in the neck (A, arrow), whereas the second has developed widespread subcutaneous emphysema. Note the air within the pectoral muscles (B, arrows).
Subcutaneous emphysema per se is innocuous most of the time and the air usually disappears spontaneously in a short time. When indicated, treatment is directed at the underlying causes, which may be classified as: iatrogenic, traumatic, spontaneous or infectious.
Iatrogenic subcutaneous emphysema sometimes occurs after surgery or after external interventional procedures. In my experience, lung transplantation is the procedure that causes the largest air collections (Fig. 2).
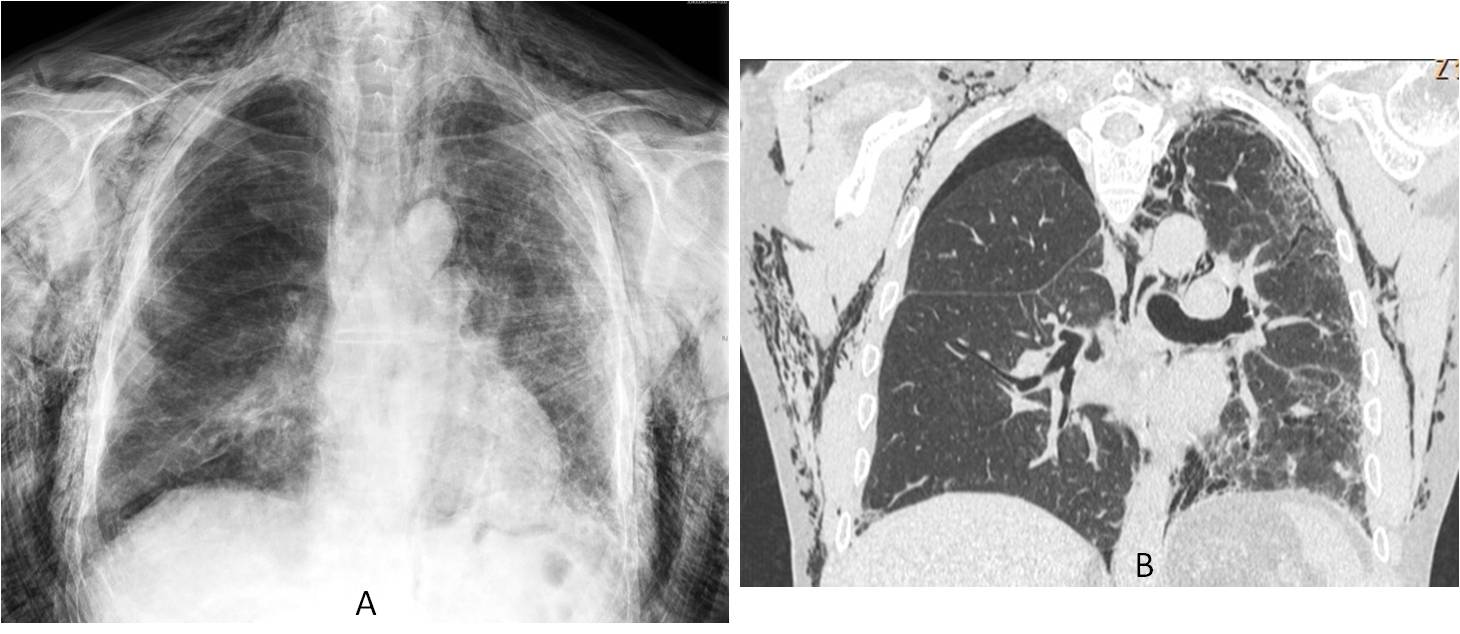
Fig. 2
Fig. 2: Severe subcutaneous emphysema after lung transplantation (A and B).
Percutaneous procedures such as lung biopsy or chest tube placement (Fig. 3) communicate the chest wall with the lung, giving rise to subcutaneous air.
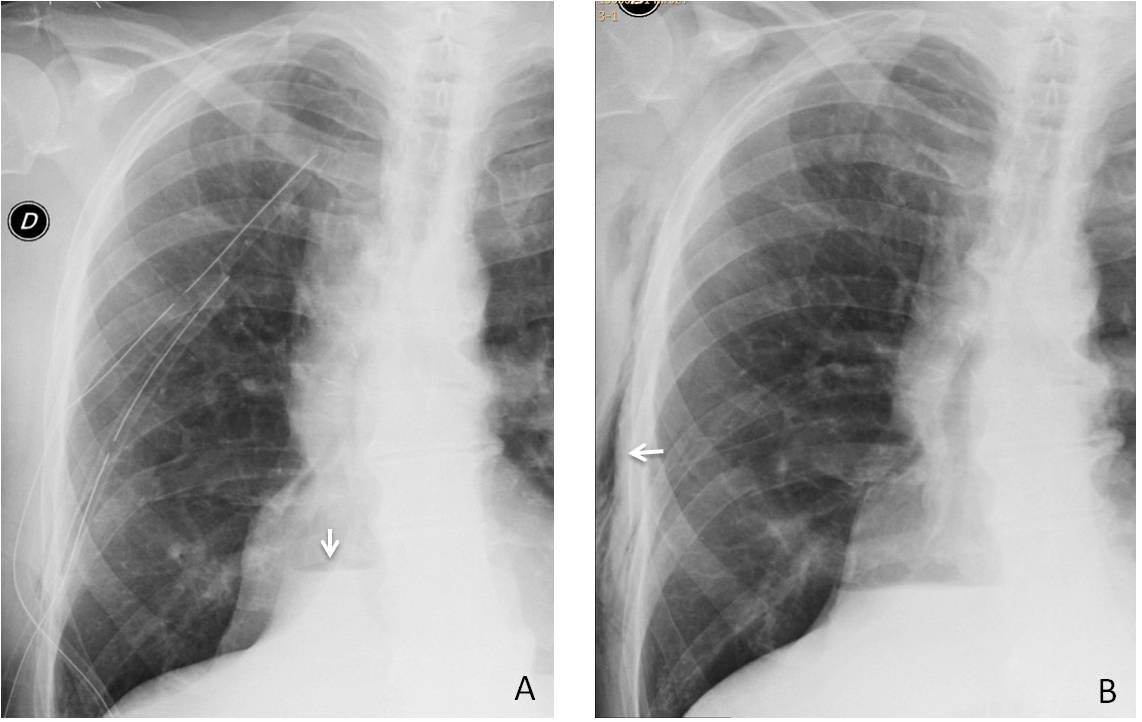
Fig. 3
Fig. 3: 62-year-old man with empyema. Initial radiograph shows draining chest tubes and an air-fluid level in the pleura (A, arrow). After removal of the tubes, subcutaneous emphysema has developed (B, arrow).
Trauma is a common cause of subcutaneous emphysema. Open wounds create a path between the room air and the chest wall, originating localized emphysema in the injured area (Fig. 4). This can also happen when an air-containing viscus is punctured (Fig. 5).
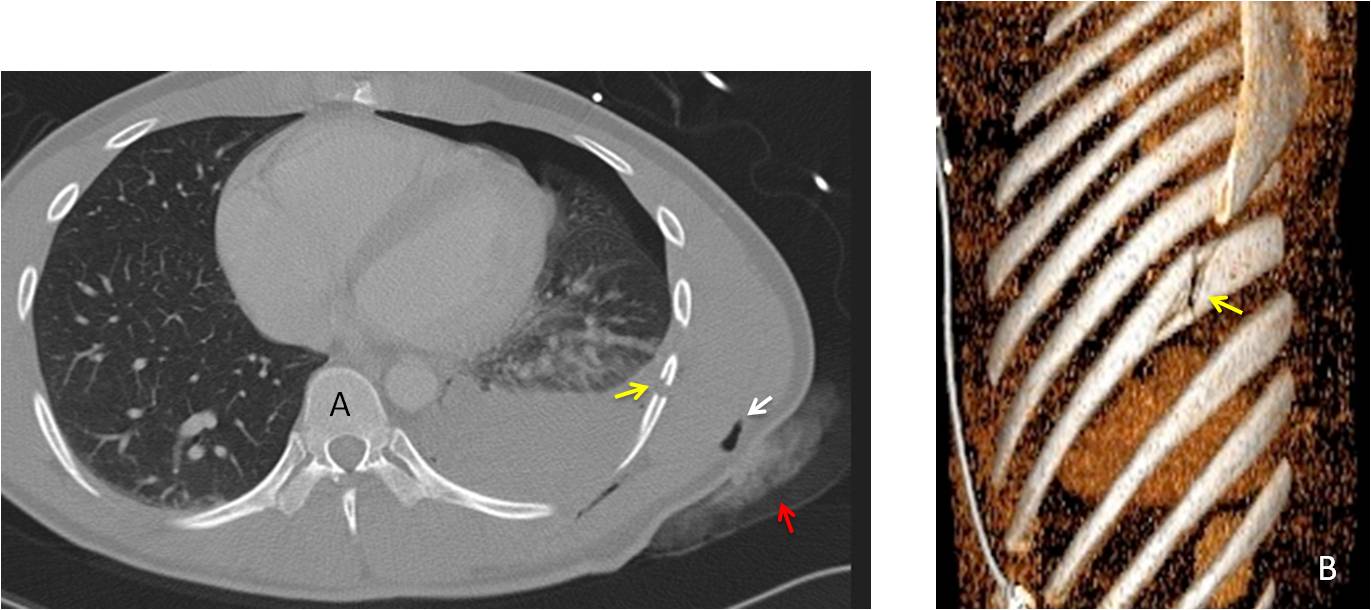
Fig. 4
Fig. 4: 24-year-old man with a stab wound in the chest. Axial CT shows hemo and pneumothorax. There is air in the area of the wound (A, white arrow), as well as bleeding of the chest wall (A, red arrow). The knife has transected one of the lower ribs (A and B, yellow arrows).
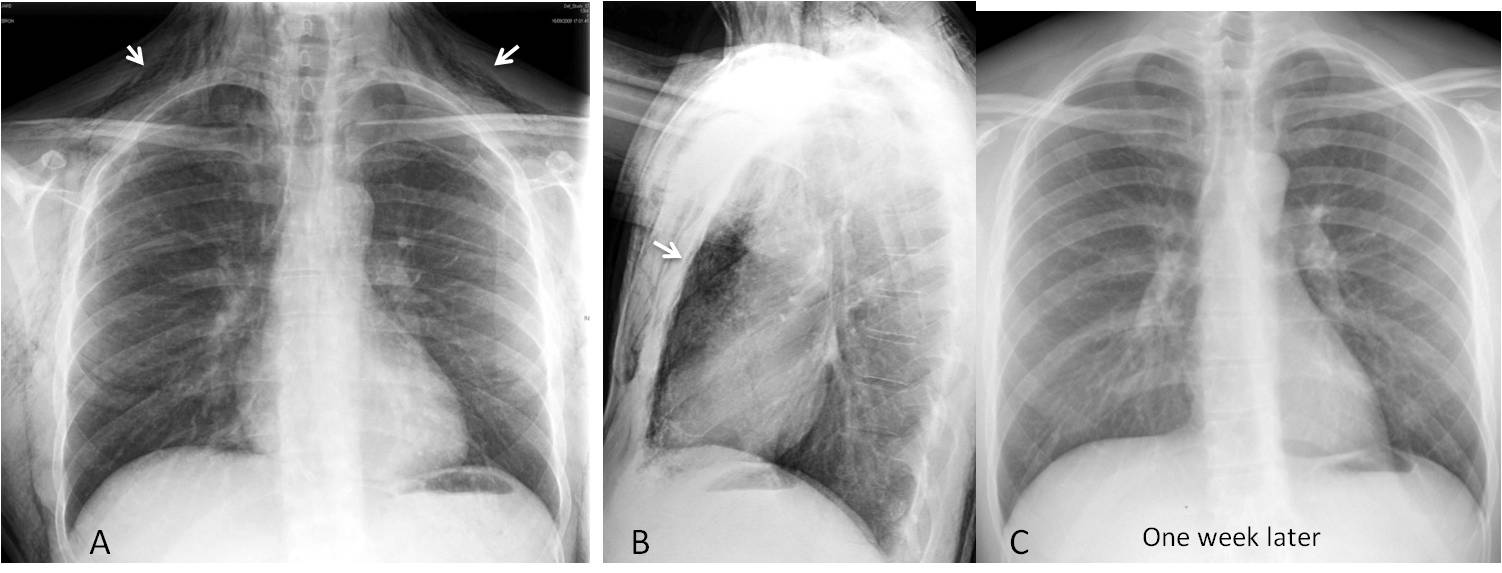
Fig. 5
Fig. 5: 27-year-old man stabbed in the neck, injuring the upper trachea. Extravasated air has collected mainly in the soft tissues of the neck (A, arrows), and some has travelled downward into the mediastinum (B, arrow). Chest radiograph one week later (C) shows that the air has reabsorbed.
Blunt chest trauma can also generate subcutaneous emphysema, usually secondary to lung puncture by fractured ribs (Fig. 6). Less common causes are ruptures of air-containing viscera, such as the trachea, bronchi, or esophagus (Fig. 7). In blunt or open trauma, subcutaneous air may underlie a serious process (eg, fractured bronchus) and should be properly investigated.
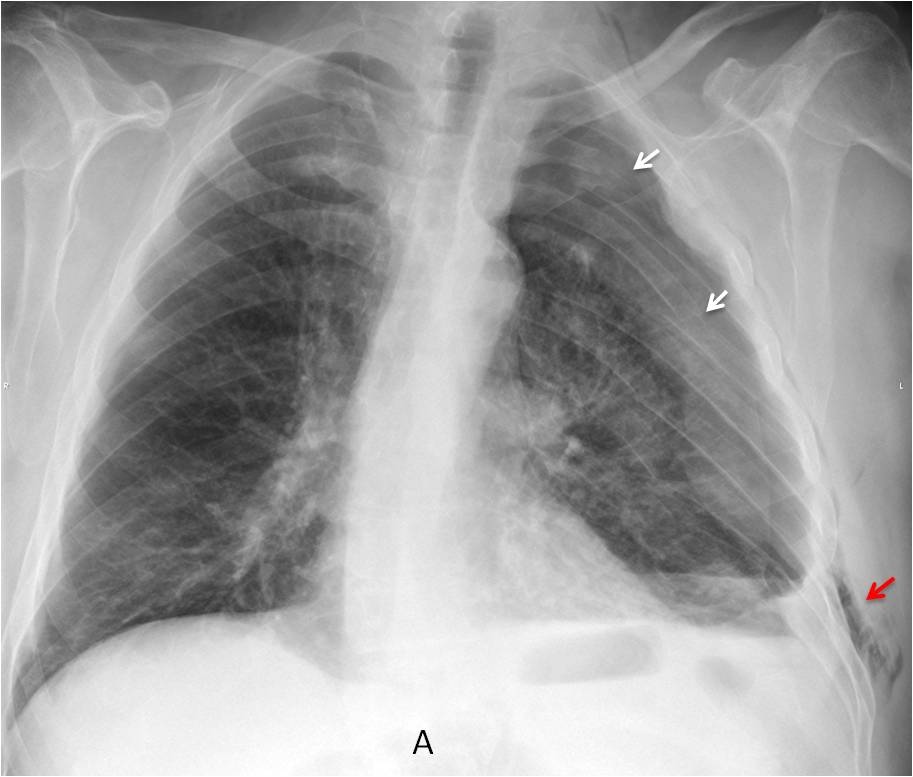
Fig. 6
Fig. 6: 38-year-old man after a motorcycle accident. There are multiple fractures on the left (A, white arrows) accompanied by subcutaneous emphysema (A, red arrow).
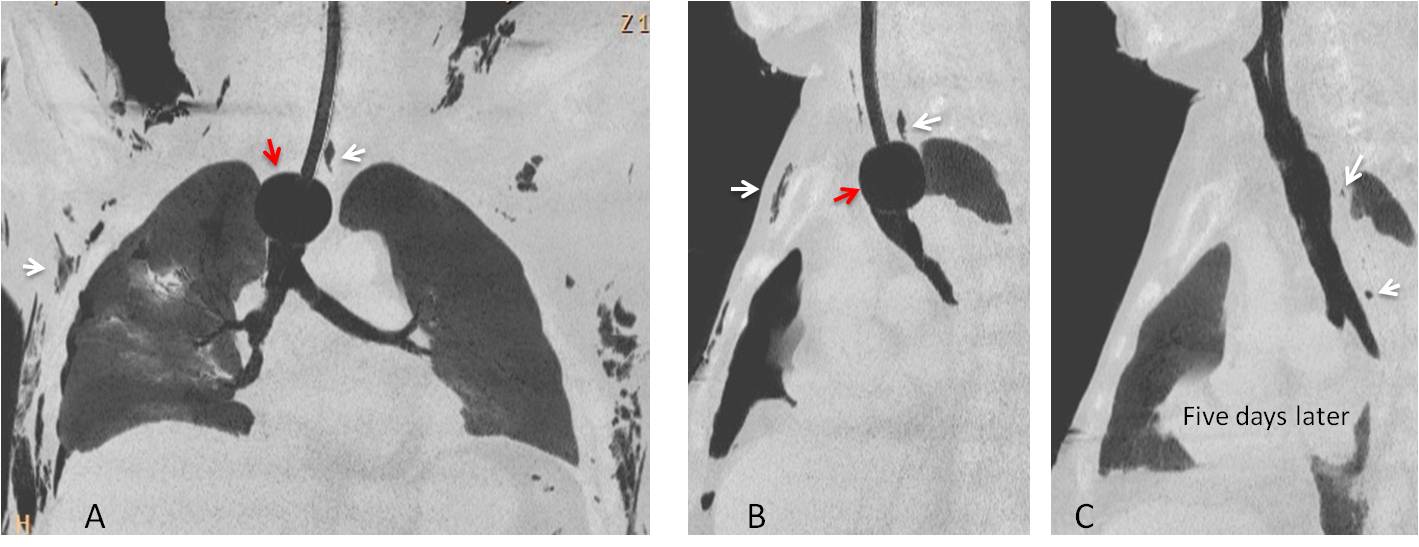
Fig. 7
Fig. 7: Pneumomediastinum and subcutaneous emphysema caused by a tracheal tear after overinflation (A and B, red arrows). Initial films show linear air in the mediastinum and subcutaneous emphysema (A and B, white arrows). Five days after removal of the balloon, the air has practically disappeared (C, arrows).
Spontaneous subcutaneous emphysema is associated with spontaneous pneumomediastinum, when alveolar rupture occurs due to increased intrathoracic pressure (cough, vomiting, mechanical ventilation). The extravasated air migrates across the interstitial space towards the mediastinum and to the soft tissues of the chest wall. The most common etiology is asthma (Fig. 8), although modern life has generated other causes as well (Fig. 9).
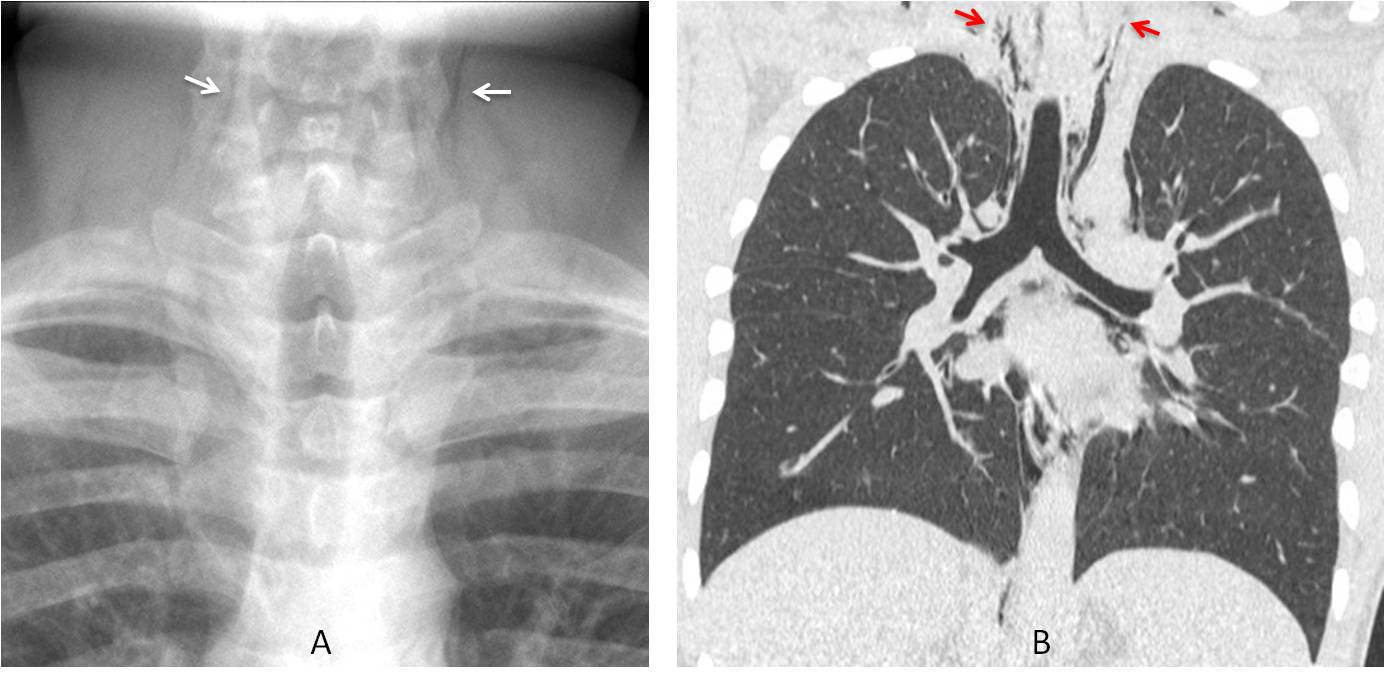
Fig. 8
Fig. 8: 18-year-old male adolescent with an acute asthma attack. Cone down view of the neck shows streaks of air in the soft tissues (A, arrows). Coronal CT confirms the air in the neck (B, arrows) and the associated pneumomediastinum.
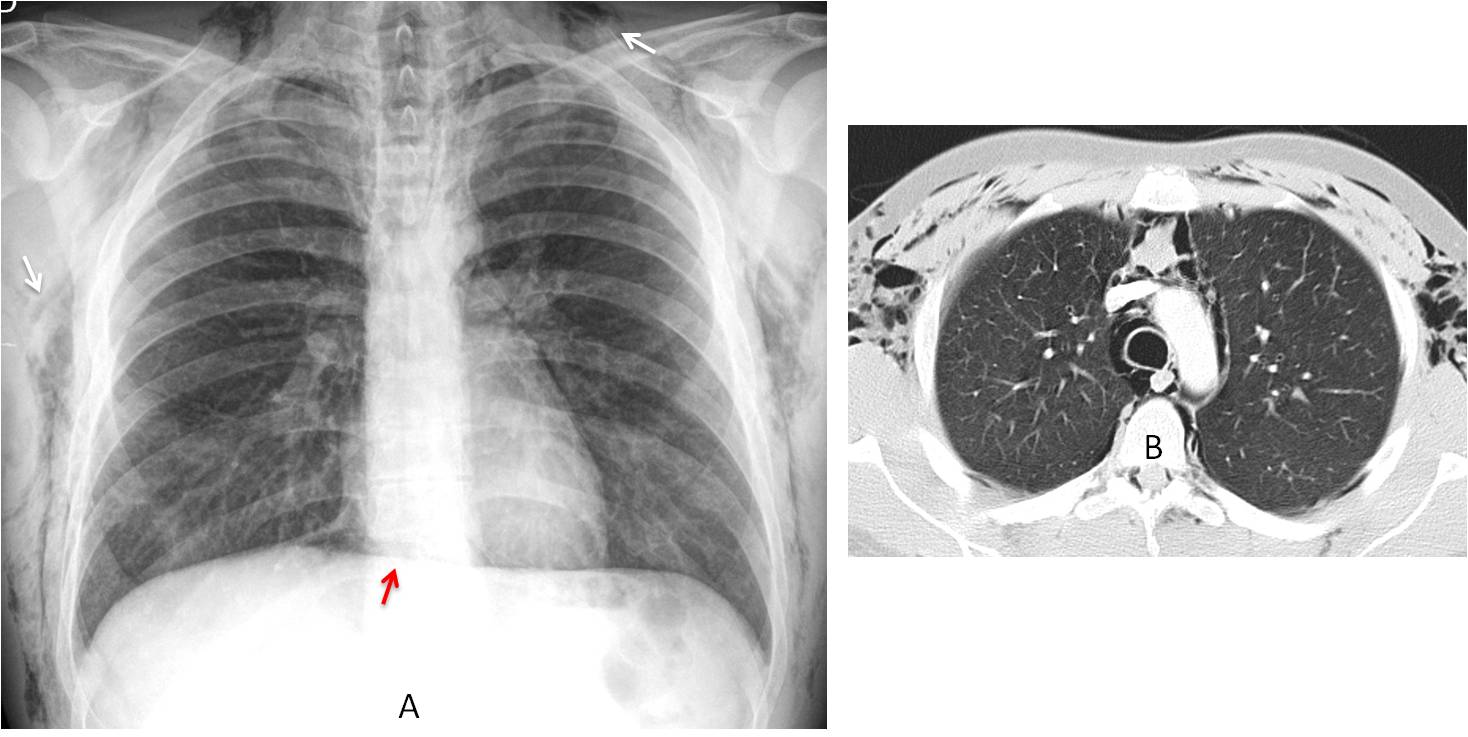
Fig 9
Fig. 9: 40-year-old male cocaine addict with chest pain. Cocaine snorting is a well recognized cause of pneumomediastinum. PA chest film shows air in the mediastinum and soft tissues of the chest (A, white arrows). Note the continuous diaphragm sign (A, red arrow). Axial CT depicts the extravasated air in the mediastinum and chest wall (B).
Case courtesy of Dr. Eva Castañer
Infection is a rare cause of subcutaneous emphysema, which may be related to air-producing organisms or underlying diabetes (Fig. 10).
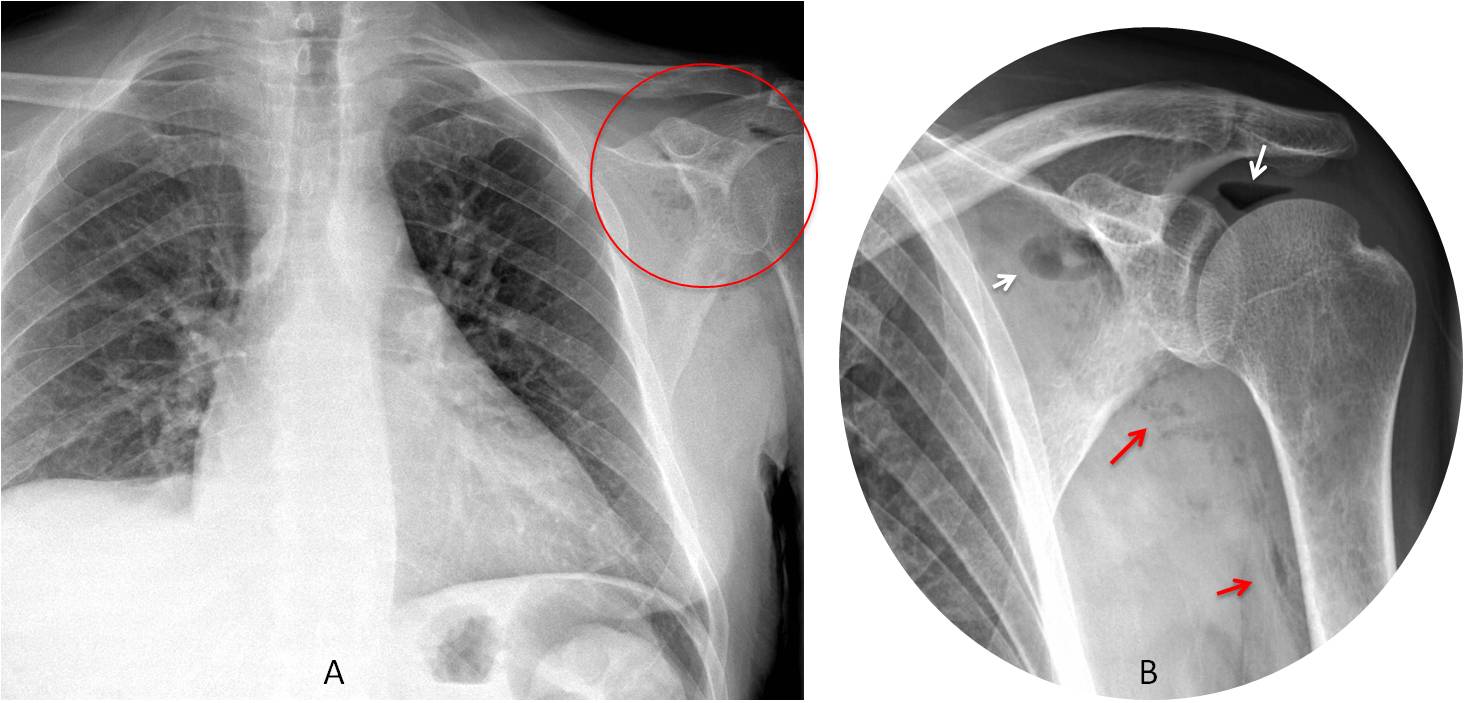
Fig. 10
Fig. 10: 58-year-old man with fever and shoulder pain. There are pockets of gas in the left shoulder (A, circle). Cone down view shows air within the shoulder joint (B, white arrows) and soft tissues of the arm (B, red arrows). Diagnosis: septic arthritis of the left shoulder joint.
Subcutaneous emphysema may also originate outside the chest when air migrates from neighboring areas, such as the soft tissues of the neck or abdomen (Fig. 11).
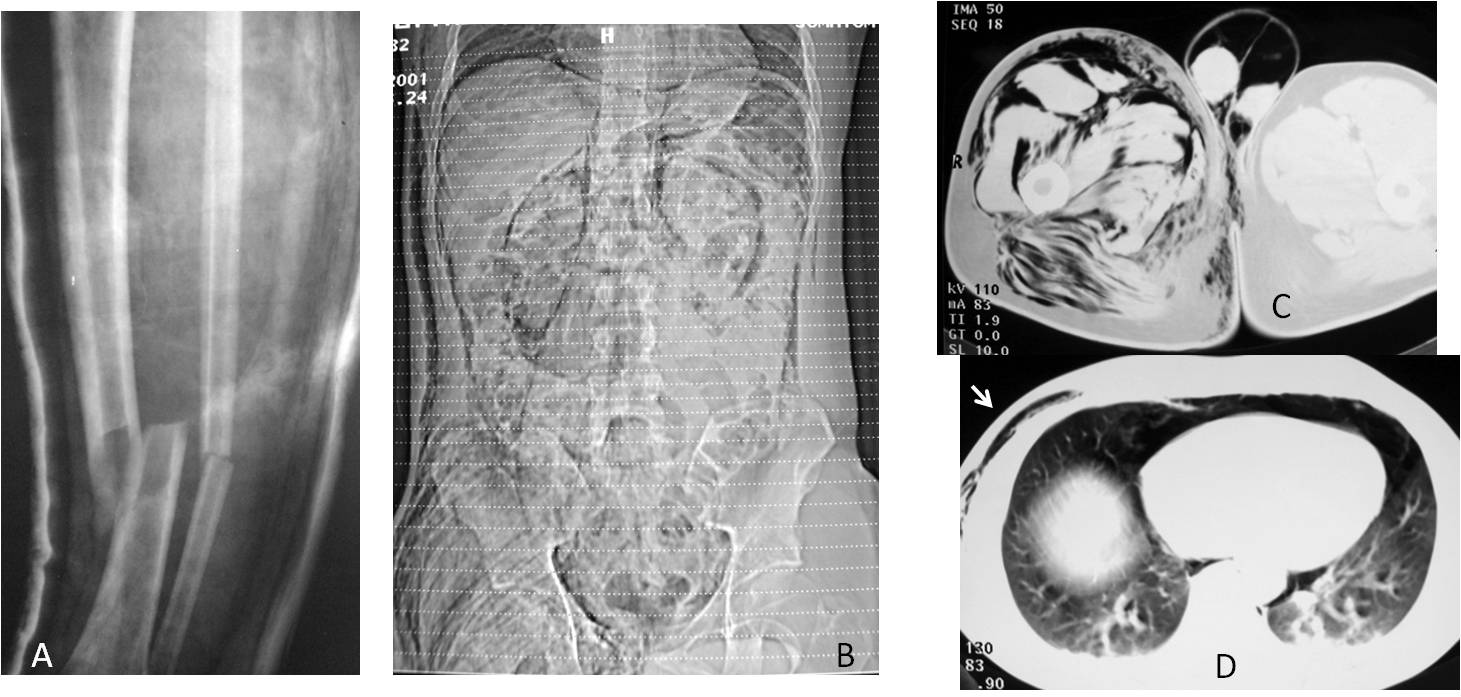
Fig. 11
Fig. 11: 42-year-old man who sustained a blow to the right leg with an air pump. The accident broke his tibia and fibula (A) and injected air under pressure into the soft tissues of the leg and right abdomen (B and C) that reached the chest wall (D, arrow).
Case courtesy of Dr. Delia Sureda
Lung hernia, an uncommon condition, is seen as a rounded pocket of air overlapping the chest wall (Fig. 12). It may not be visible in inspiratory films, but can manifest in expiratory views. Lung hernia is secondary to weakening of the chest wall and is usually related to previous surgery, although it can be spontaneous (Fig. 13).
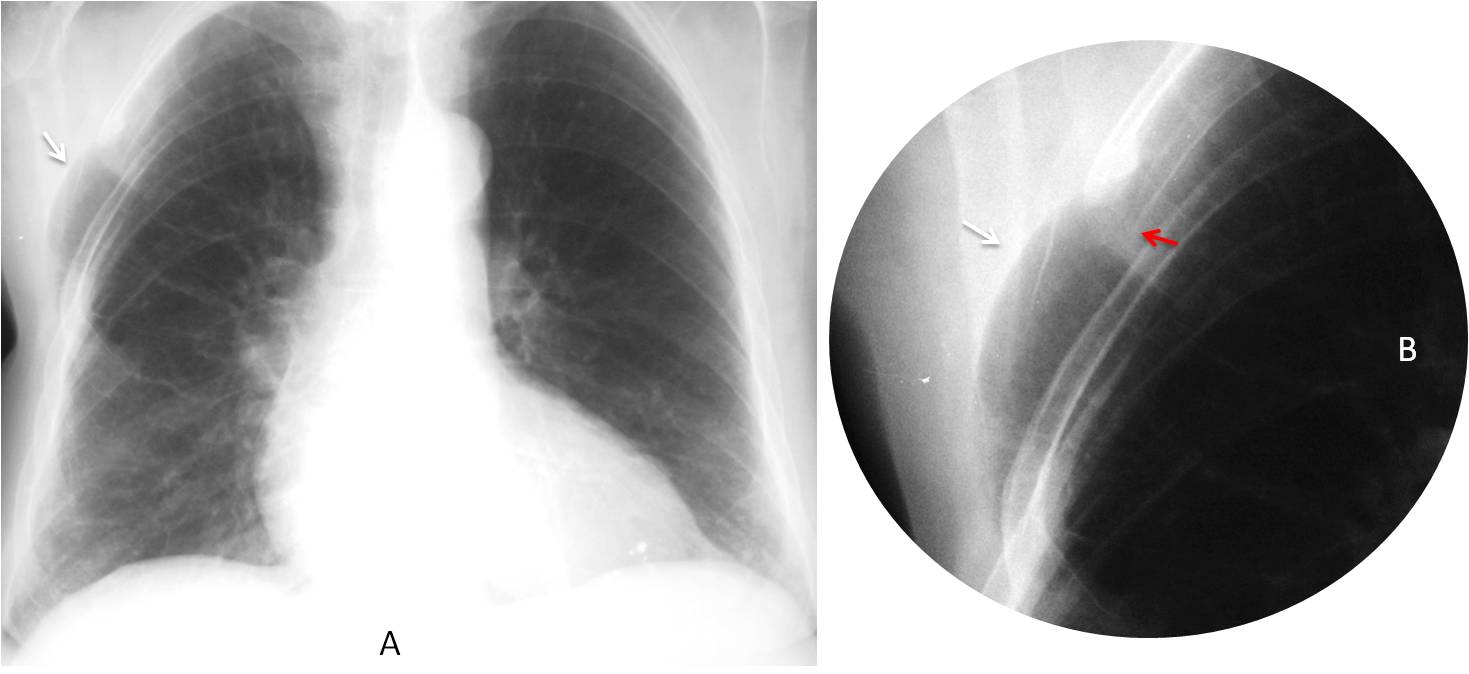
Fig. 12
Fig. 12: Hernia of the right lung after surgery. Note the rounded herniated lung (A and B, white arrow) in the area where the rib was resected (B, red arrow).
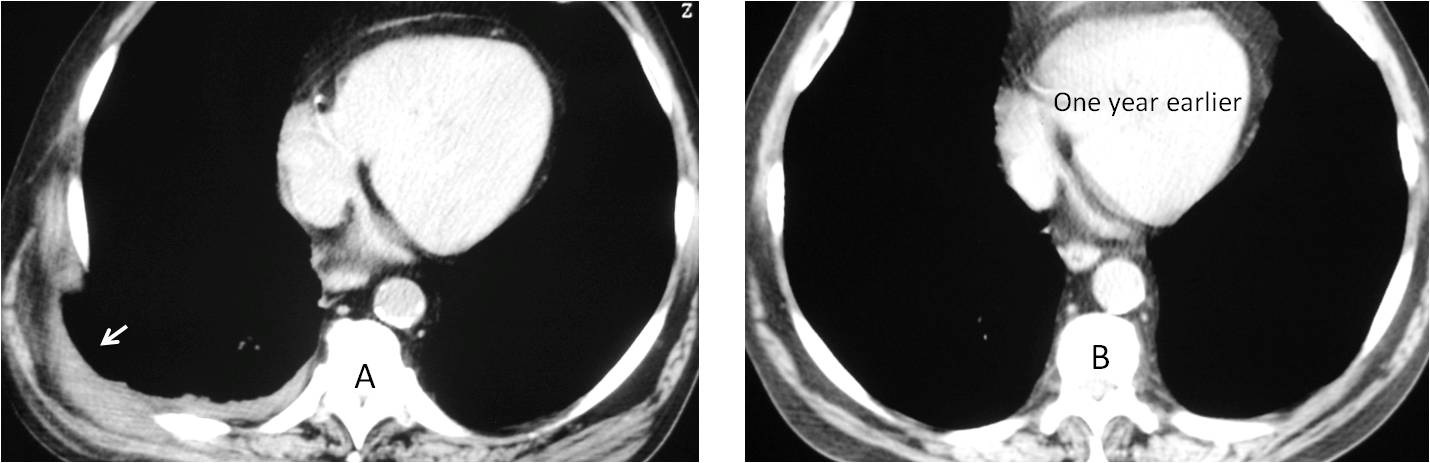
Fig. 12
Fig. 13: 56-year-old man with pain in the right chest after forceful coughing. Axial CT shows a tear at the intercostal space and secondary hernia (A, arrow). Compare with a CT image taken one year previously (B).
Coronal CT shows the herniated lung more clearly (C, red arrow). 3-D reconstruction (D) depicts the widened space.
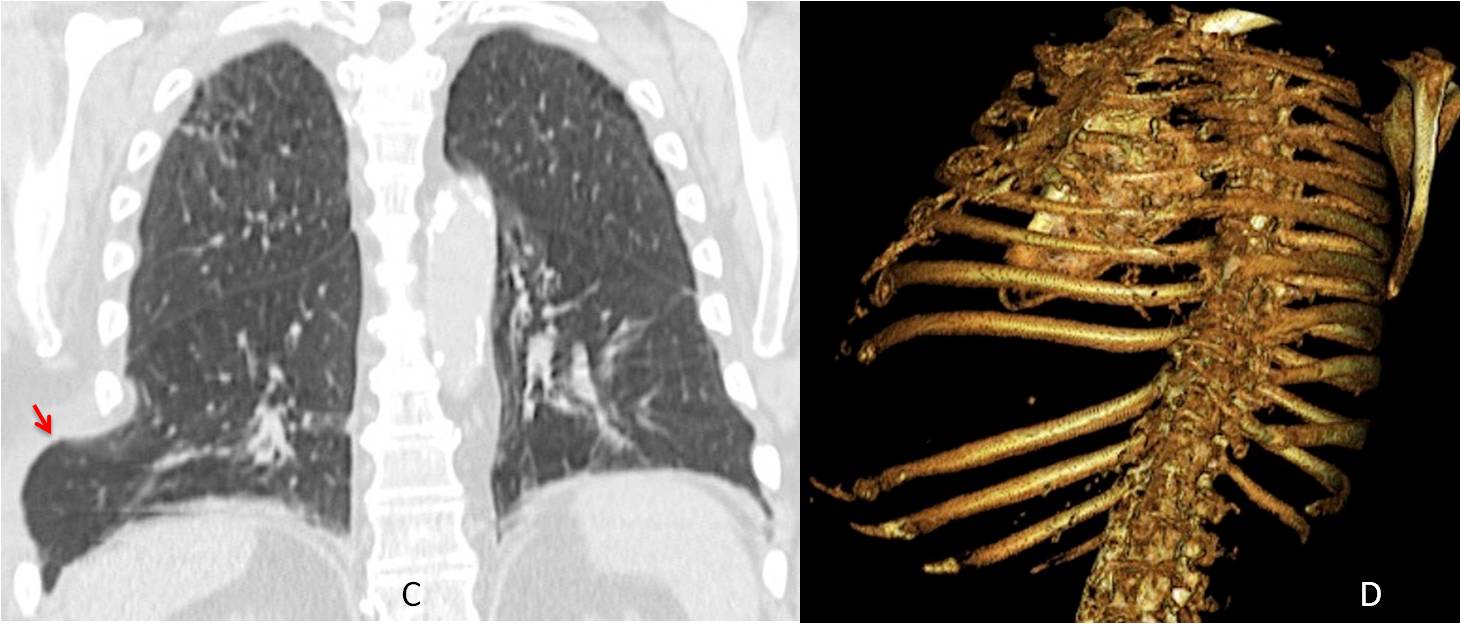
Fig. 13

Follow Dr.Pepe’s Advice:
1. In most cases, subcutaneous emphysema is innocuous and disappears spontaneously.
2. The four causes are: traumatic, spontaneous, iatrogenic, and infection.
3. Lung hernia is uncommon and usually related to previous surgery.


Right lung volume loss, probably secondary to a neoplasm involving the right main bronchus. Fracture of the 4th left rib, laterally, with lung herniation as a sequela.
Good approach. But: how many times have you seen herniation of the lung after fracture of one rib?
Right lung volume loss and diffuse interstitial reticular opacities. Asymmetric fibrotic lung disease?
The left hilum looks distorted but this could be due to the mediastinum shift.
I agree with Mauro about left rib old fracture and lung herniation.
Hello,
there is significant volume loss of right lung with mediastinale shift to left and diaphragm elevation.
Massive fibrosis – maybe after radiation terapy? some history needed.
I agree with Mauro about lung herniation with rib fracture.
Tumor right hilum wth necrosis after radiotherapy with volume loss of right lung with reticulonodules pattern,elevation of right diaphragm ,Shift of mediastinum to the right
pmf
Reticulonodular opacites on right side. Right hilum tumor susp. Mediastinum shift on right side. Right diaphragm lift up. Fracture of the 4th left rib-meta susp. Aortic arch dilatation.
with herniation on left side probably true.
Significant volume loss of right lung with mediastinale shift to right and diaphragm elevation.
Cause probably fibrosing mediastinitis, Idiopathic
I agree with Mauro about left rib old fracture. Osteoporosis
Necessary CT
Reticulonodules opacieties on right side, status post radiotherapy. Right hilum Tu-suspect. Shift mediastinum on right side.Aortic arch dilated. Fracture of the 4th left rib-meta suspect with herniation.
Unilateral left lung transplantation for fibrotic lung disease with lung herniation?
Congratulations! Well done!
Actually, all the information is in the radiographs. It is a matter of interpreting it correctly:
a) most common cause of herniation: surgery
b) disparity between both lungs: transplant
See Caceres’ corner case 56
….pregiatissimo Professore….iperchiarezza del polmone sx, bolla di enfisema sottocutaneo….a dx, perdita di volume del polmone, risalita della cupola diaframmatica, con shift cardiomediastino, da probabile cr ilare…
….frattura costale sx, recente….
Raised right hemidiaphragm. Also decreased right lung volume, ipsilateral mediastinal shift
In addition there is increased interstitial thickening in the right lung.
Fracture at the left sided 4th rib, focal pleural thickening and also a pocket of air lying outside the left lateral chest wall in the axillary region suggests lung herniation.
Most likely the findings are due to trauma
Emphysema can also be hereditary. Emphysema Natural Treatment improve health naturally, viably and securely. The reality of the situation is that the Herbal Supplements properties of herbs have been ” proven ” when you widen the criteria of what is acknowledged as the standard of proof.