here is a new case from Hospital Dr Peset archive.
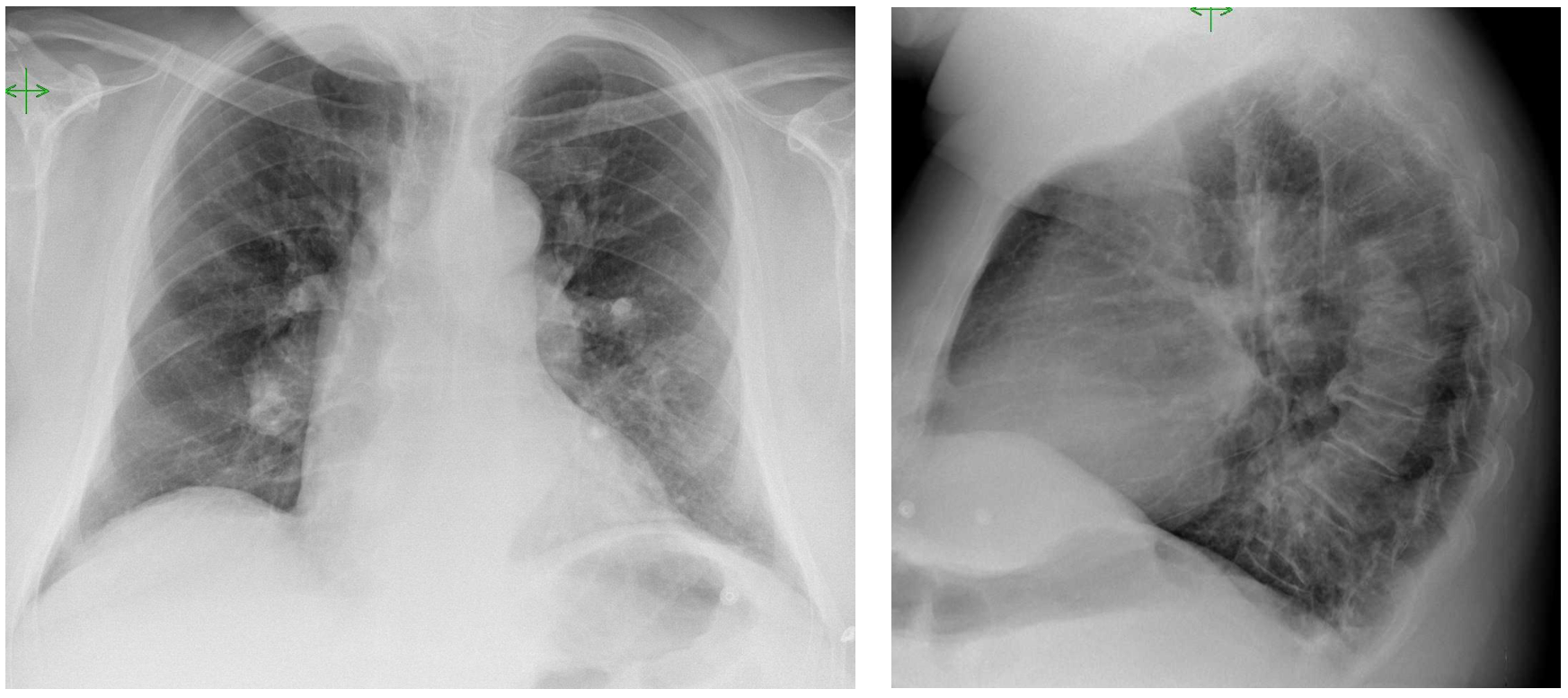
This is a 67 year old man with COPD. He was presented with worsening of his dyspnea, he now needs two pillows to sleep.
Solution:
In this patient the prominent finding is an enlarged right parahilar area (Arrows). The enlargement has a “tubular” shape. A tube pointing towards the hilum should be either a bronchus or a vessel.
Some of you mentioned pulmonary arterial hypertension and these could be true but in this case there is a specific sign that should orient you.
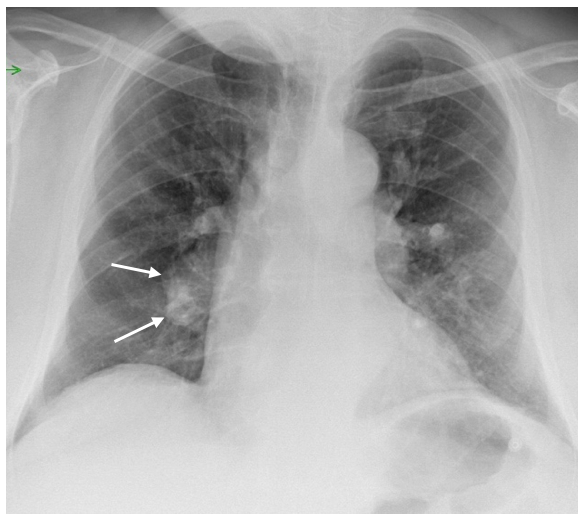
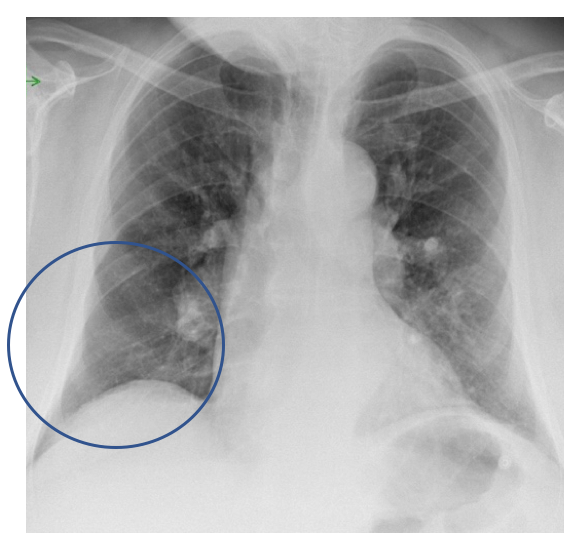
Indeed here we see a signs of acute pulmonary embolism: the Palla sign.
Dr Palla, an Italian radiologist and his colleagues from Pisa described in 1983 a sign of pulmonary embolism: the enlargement of the right descending pulmonary artery in PA chest radiographs. They found a correlation of this enlargement in several patients as compared to normal and to the same patients after treatment. Unfortunately this sign has not proven to be very common, although probably with the advent of CT angiography we don´t look for it very often.

The combination of the clinical scenario and the Palla sign raises the possibility of a pulmonary embolism, and a CTA was performed.
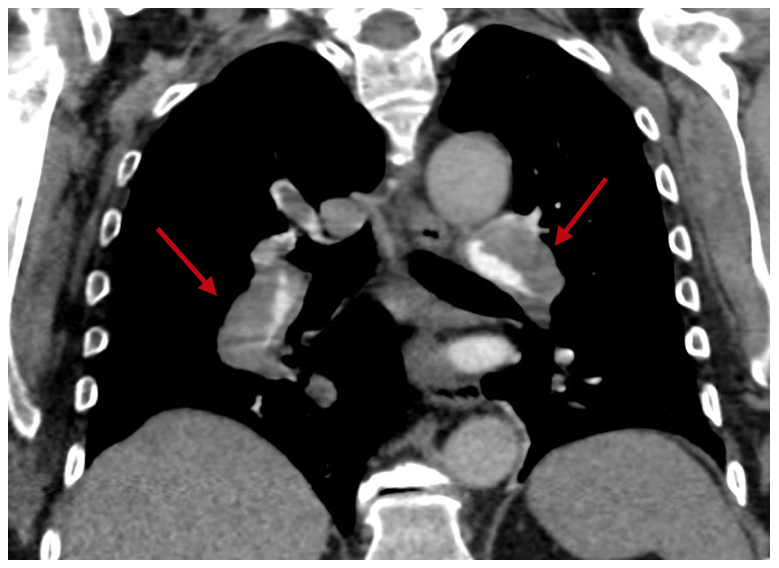
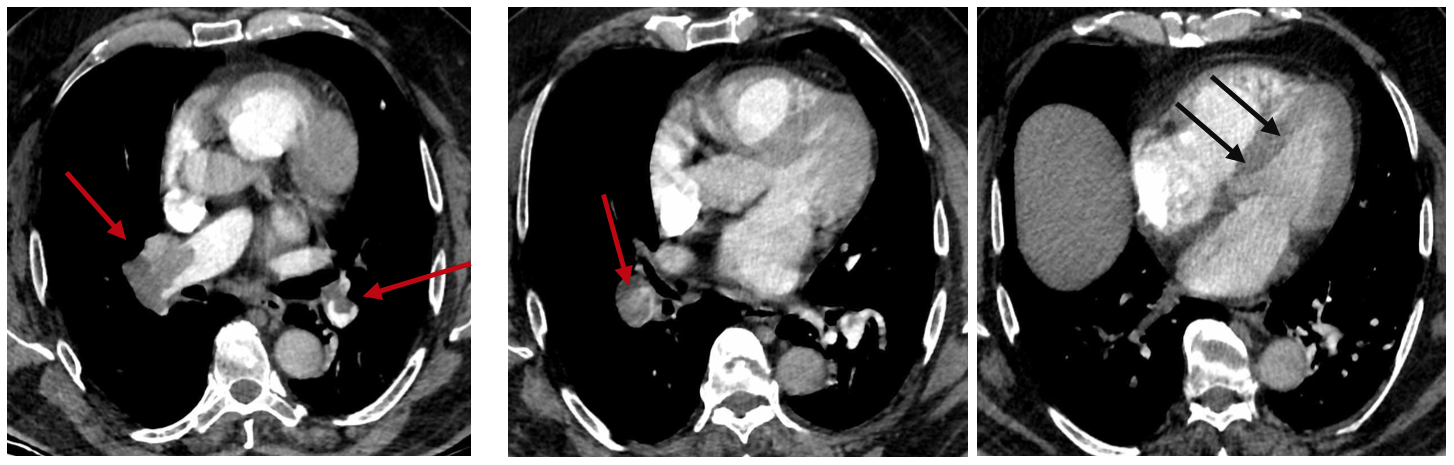
In the CT we can see the correlation with the plain radiograph. A massive thrombus occupies the right and left pulmonary arteries. (Red arrows).
Also the CTA shows signs of right ventricular overload with flattening of the interventricular septum ( Black arrows).
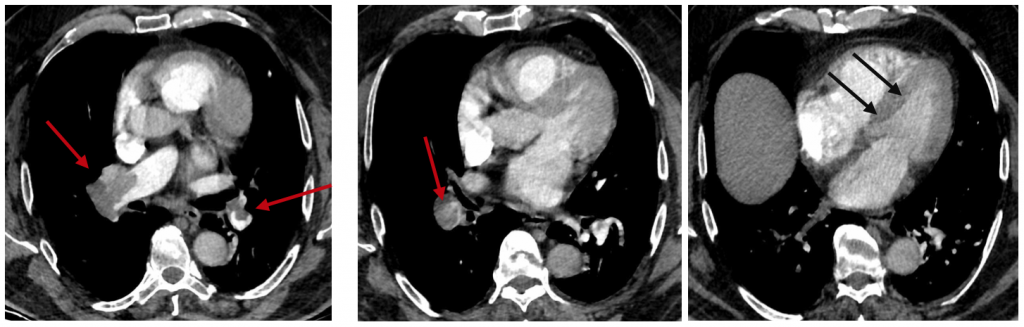
The diagnosis is then Pulmonary embolism with Palla sign
This is again another reason to look carefully at the Chest radiograph. Indeed, if you look closely in this case you can see also a lack of vessels in the right lower lobe ( Westermark sign), not so clear as in other cases, but present, indicating the lack of perfusion this area.
Now a bit more about our current problem COVID 19. In a recent Webminar conducted by Dr Adrian Brady at ESR ( ESR Connect ) Drs M.Sanchez from Barcelona and M.P. Revel from Paris commented the high frequency of pulmonary embolism ( 24-30%) in some of the hospitalized patients with COVID 19.
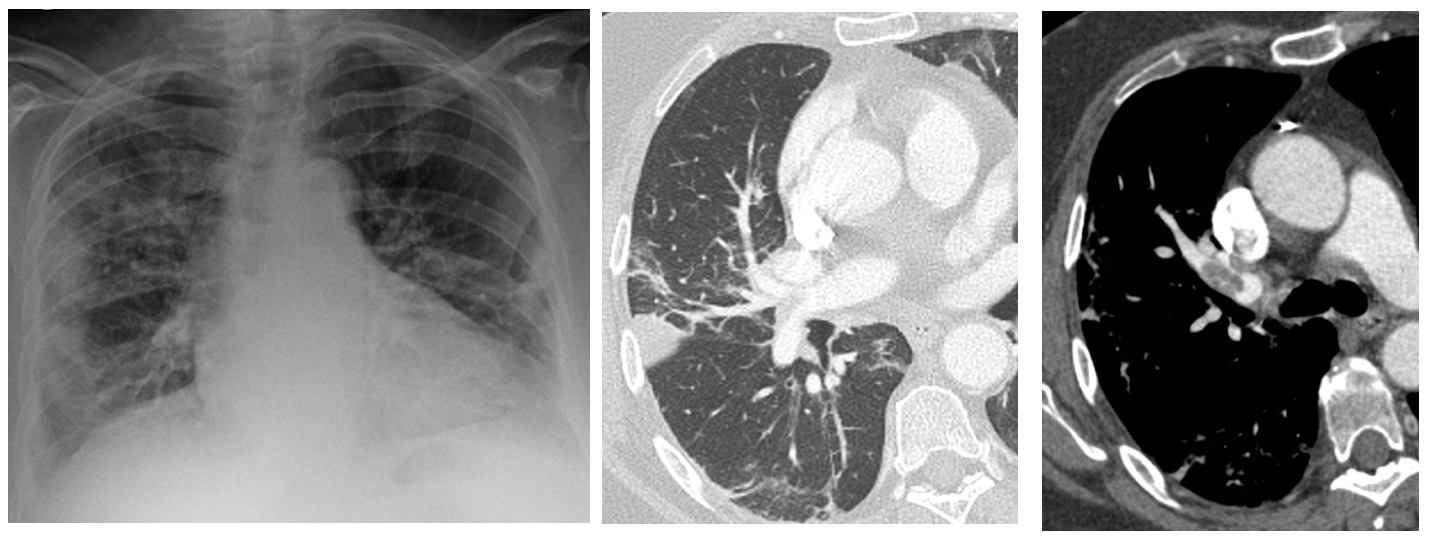
From Barcelona my good friend Dr. Marcelo Sanchez sends me this case. This patient with a positive COVID 19 PCR had severe distress and Dimer above 4000.
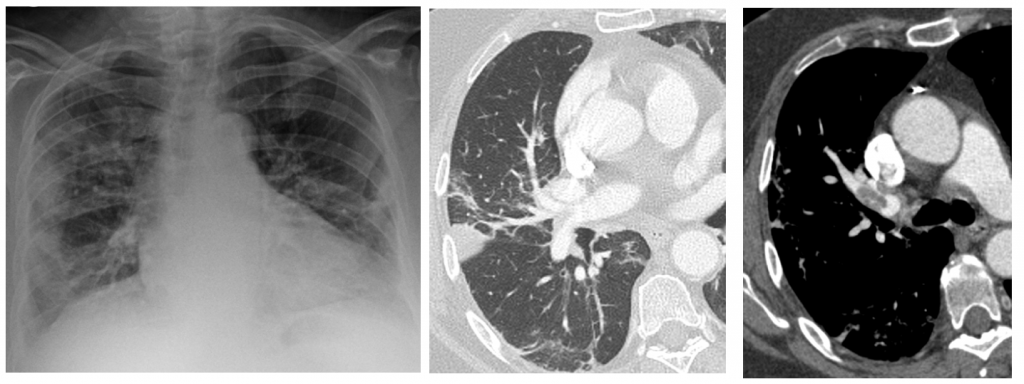
Patient with positive PCR for coronavirus. Portable radiograph and CTA: Bilateral, peripheral pulmonary opacities with a right pulmonary peripheral consolidation suggestive of pulmonary infarction. Pulmonary embolism.
Therefore, Pulmonary embolism has to be considered as a possibility in a COVID 19 scenario especially in patients with severe disease, respiratory impairment and very high D Dimer.



Pulmonary hipertension – angio CT
CXR AP view reveals enlarged bilateral pulmonary arteries and Lateral view shows reduced retrosternal space due to enlarged RV. Finding represent features of Pulmonary arterial hypertension.
Sorry CXR PA view… typing error
There is increased cardiothoracic ratio, interstitial pattern and widening of the hila bilaterally.Regarding the clinical information (orthopnea) I would suggest interstitium pulmonary edema. Heart echo next
Thank you so much for sharing this great inspiring and helpful too.Hope you continue to share more of your ideas.I will definitely love to read.