José Vilar and Friends Case 30 (Update: Solution + Bonus Case!)
Dear friends.
Life goes on and I expect that you all are in the best possible shape.
This time we abandon the chest and move downwards to the abdomen.
I propose a case from Hospital Universitario Dr. Peset, provided by Dr. Andrea Manrique.
This is a 52 year old woman with repeated urinary infections. An abdominal radiograph was obrained to rule out urinary lithiasis.

Let us see what you think this could be and what would you do.
Additional information:
OK. Let me add some more images:
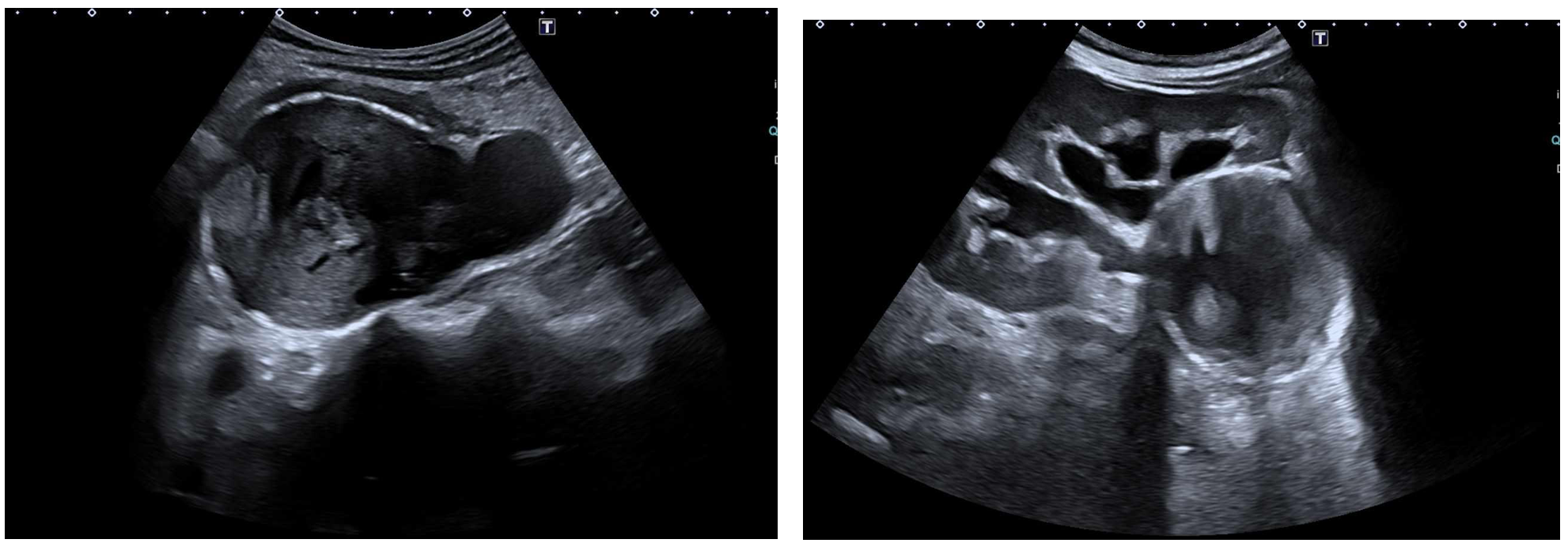
An abdominal ultrasound was performed. What do you see and does it point to any probable diagnosis?
Click here for the answer
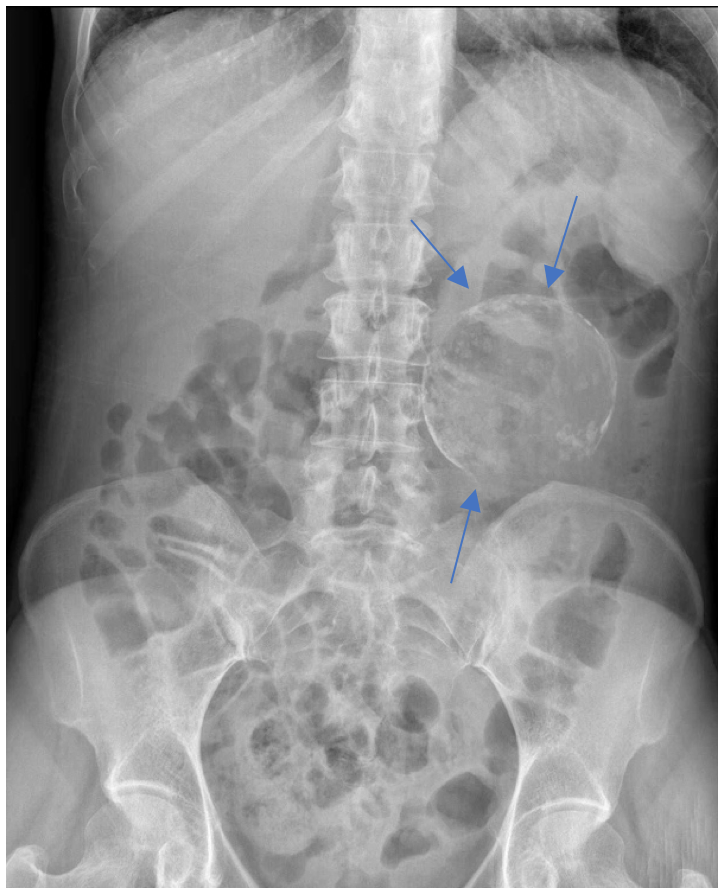
The plain radiograph of the abdomen shows a nonspecific air pattern I the intestine. A rounded calcification with a fine wall is seen in the left renal area with a discrete mass effect. No other calcifications are detected.
In view of this finding an ultrasound was performed.
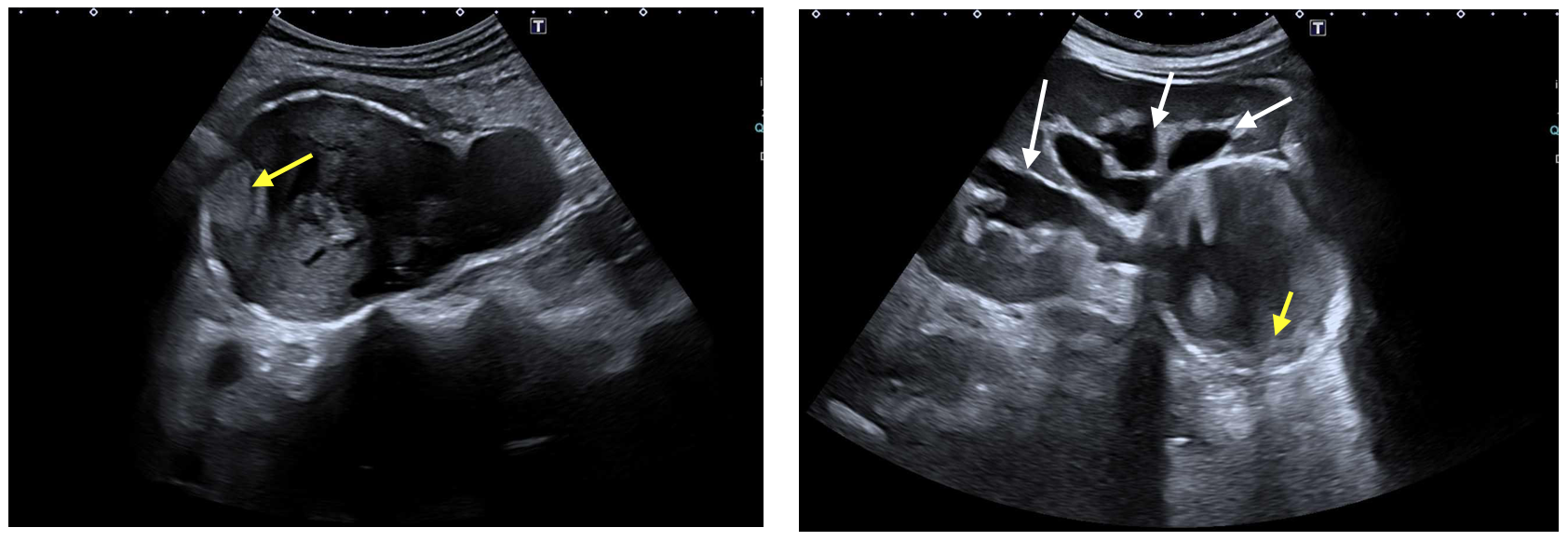
In the US study the lesion is well defined with hyperechogenic walls due to the calcium. There is some nodularity (yellow arrows) of the wall and a clear dilatation of the collecting system. (White arrows).
In view of these findings a contrast CT was performed.
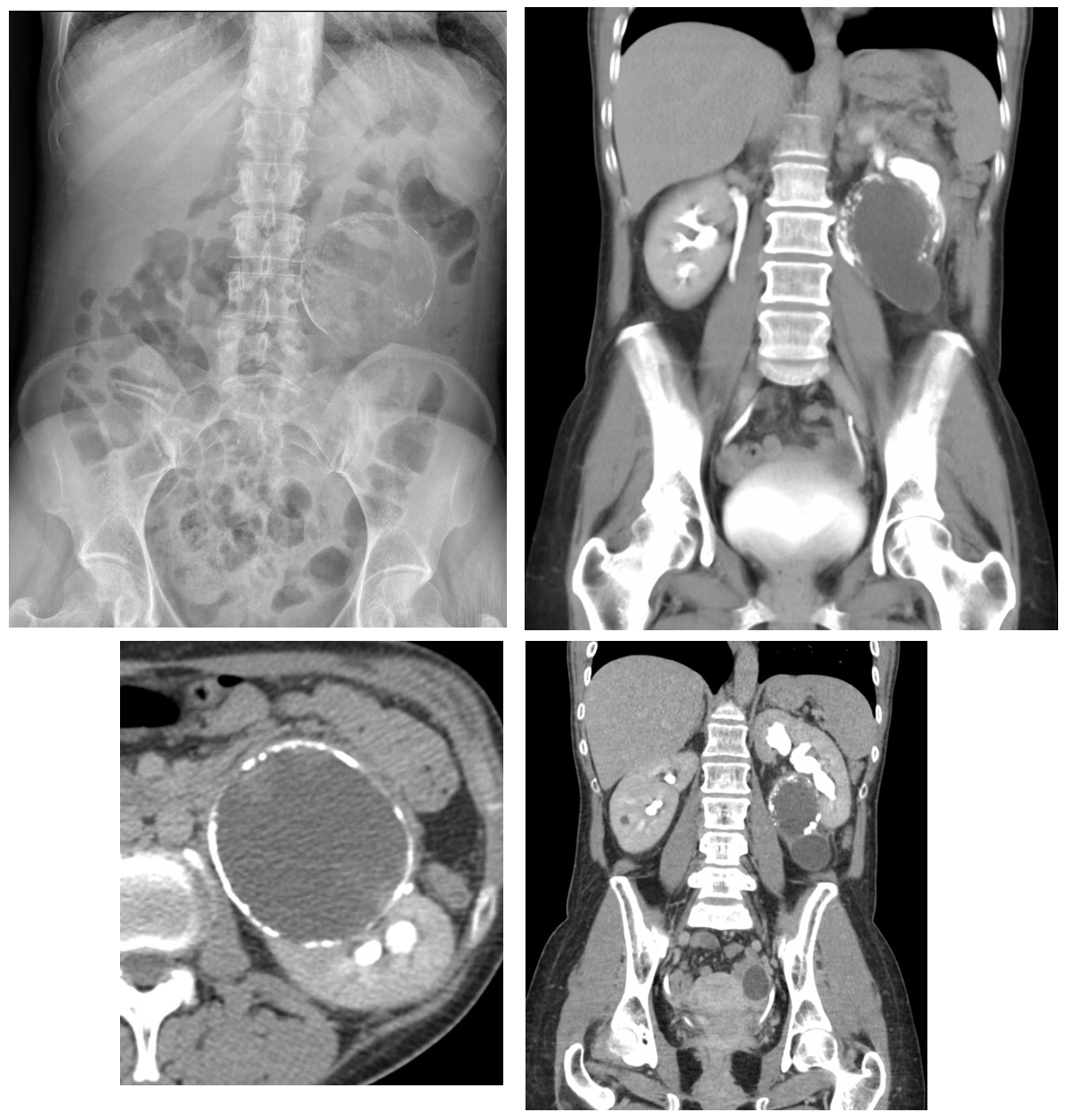
Contras CT: Coronal images: Left renal mass, extrarenal situated medial to the left lower pole with extrinsic compression of the ureter and hydronephrosis. No uptake of contrast in the wall.
Comment: The finding of this left renal lesion was incidental. The patient’s symptoms were not related to this lesion.
In the presence of a renal mass with calcium the differential diagnosis is very wide, from Hypernephroma to aneurysms, chronic infection, cysts with hemorrhage etc.
The first examination after we find this type of lesion is Ultrasound that will help characterize the lesion: Calcium in the wall, cystic component with some nodularity and lack of doppler signal were the main findings.
CT further informs about the relation of the mass to the kidney and nearby structures.
All these findings, can be applied to the Bosniak classification of renal cysts. In our case this is a category Bosniak II. (Thin wall no contrast uptake, hypodense). The probability of being malignant is very low, therefore surgery is not indicated unless there are other associated findings. In this case the presence of an important compression of the collecting system ,the age of the patient, and the then new minimally invasive surgical techniques, allowed to perform a perirenal cystectomy.
The pathology although there were no scolex identified, concluded that this was consistent with a hydatid cyst.
Although hydatid cysts are today less frequent in the western countries, we should always keep I our heads that cystic masses anywhere in the body may be hydatid cyst, particularly if you see nodular walls. Since we are particularly interested with the chest, remember that hydatid cysts in the lungs may show floating nodules ( floating lily), but do not calcify (unless complicated) since they do not develop a peri cystic layer.
Bonus Case: Patient under study for aortic aneurysm.
Look at the Chest radiographs and click here to see more…

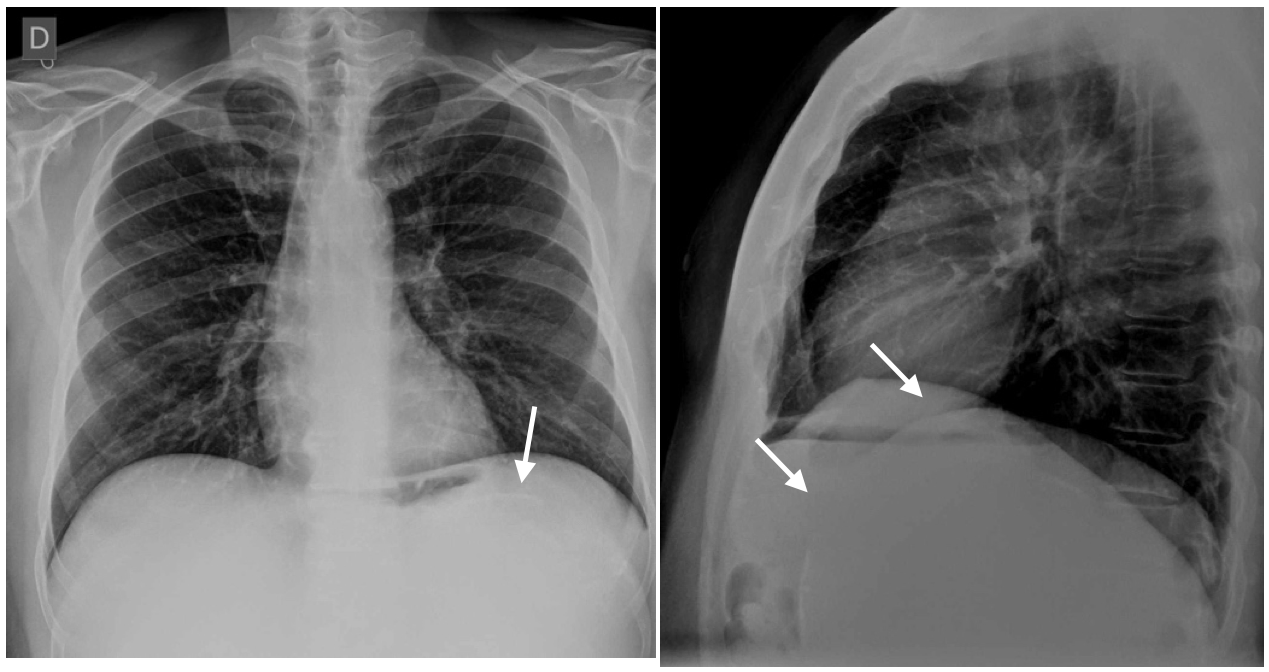
Very fine linear curvilinear calcification in the left subdiaphragmatic region.
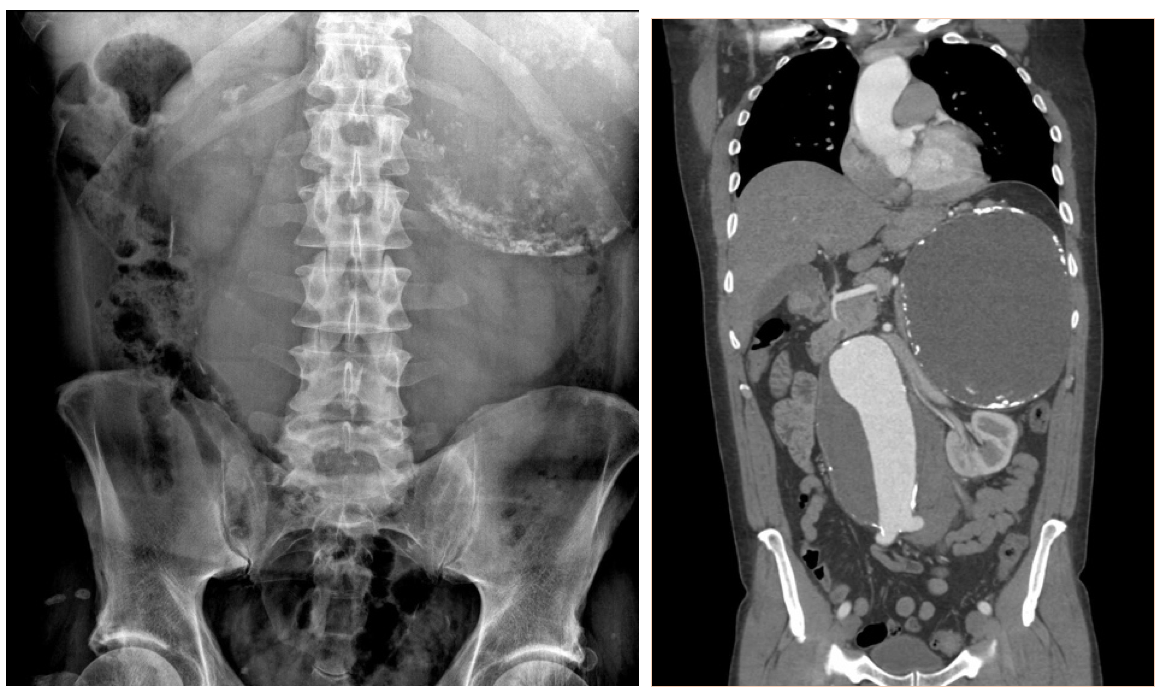
Large calcified suprarenal mass similar to the one in case 30.
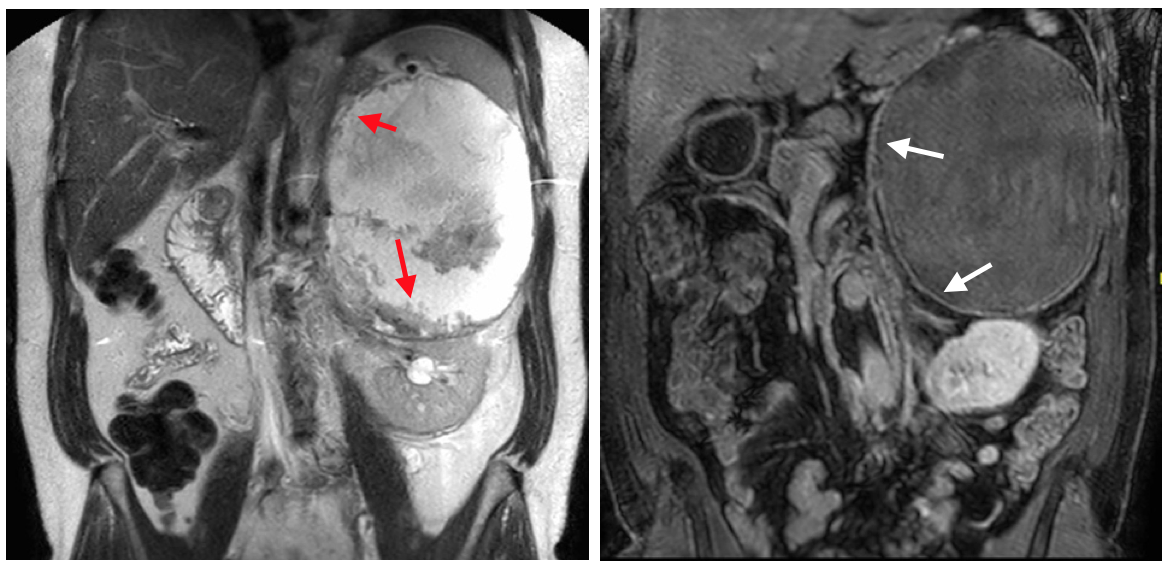
MRI. Cystic mass with internal membranes (red arrows). Late contrast image shows a thin capsular uptake (white arrows) but no nodular uptake.
Hydatid cyst (suprarenal).


Pancreatic pseudocyst with calcified walls or left kidney cyst with calcified walls
Un quiste hidaticio podria dar una imagen similar. Me llama la atencion el borde inferior incompleto, quizas nos esta diciendo algo (que no entiendo).
Si las Rx de torax ya me complican… Las de abdomen, ni hablar.
Aneurisma trombosado? Hubiese sido linda una foto con Doppler color