José Vilar and Friends Case 36 (Update: Solution + Teaching points!)
Dear Friends,
This is a 19 year old that came on a weekend at 4:30 am to the Emergency room with haemoptysis.
No previous pathology. No fever.
What do you suspect and what would you do?
Additional information:
Here is a CT of this patient. With this plus a close look at the clinical information you should think of a diagnosis.
Click here for the answer
Well done friends.
The findings in our case are:
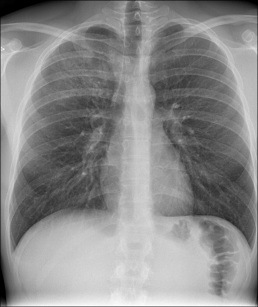
Chest radiograph. Ground glass opacity in right upper lobe. NO cardiomegaly or other findings.
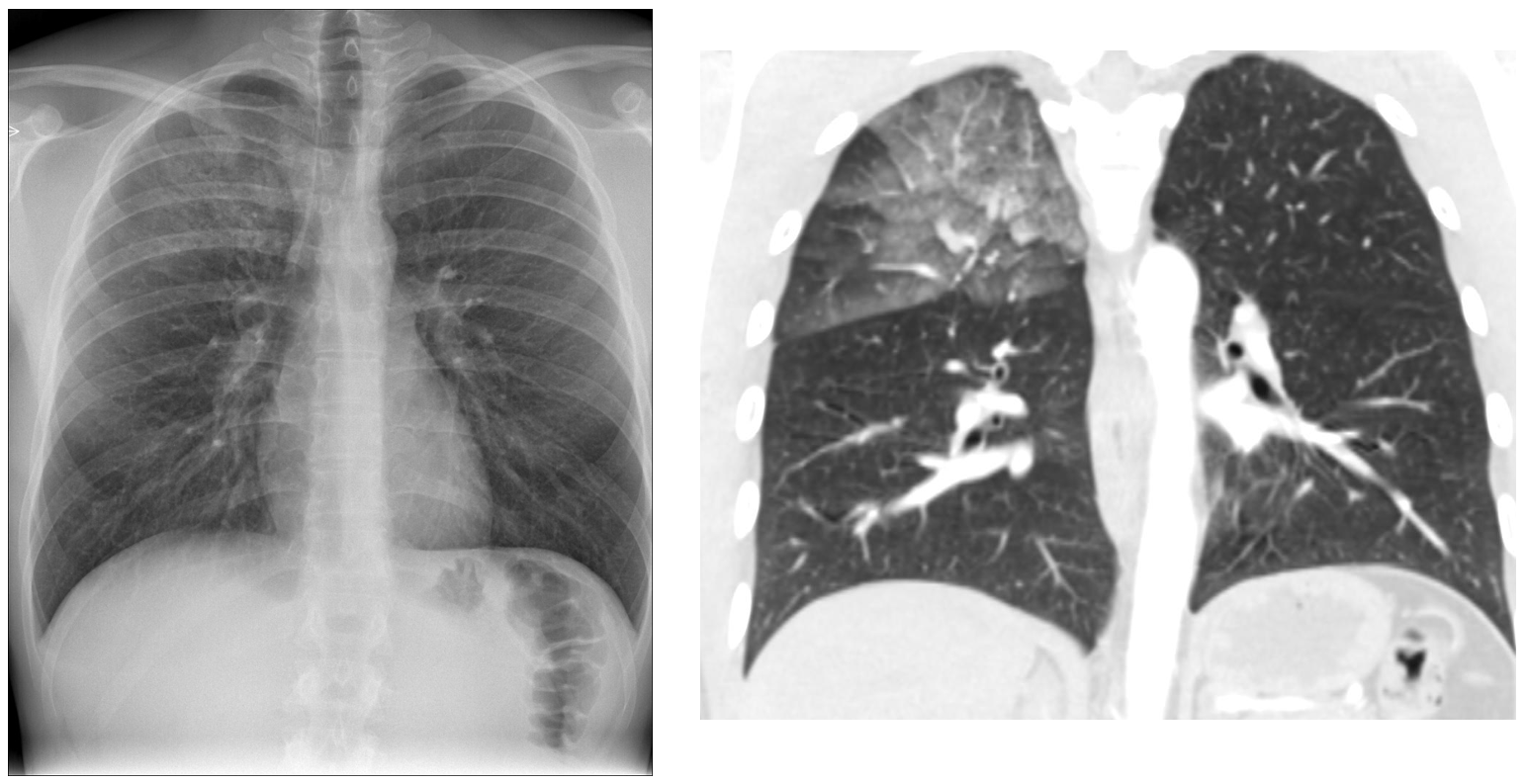
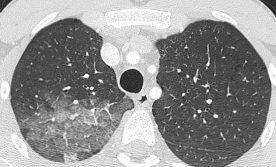
The CT confirms and correlates the presence of an air space pathology in the right upper lobe.
HRCT. The ground glass in the right upper lobe is better identified with thing slices showing interlobar thickening within the ground glass density. This is the typical “crazy paving” pattern.

Comment: The findings indicate an air space pathology with some interstitial involvement (interlobular septae).
Many diseases may produce this type of pattern ( crazy paving) thus it’s very important to correlate the clinical information with the imaging findings. In this case the clinical data that could help make the diagnosis are:
- Young patient
- No previous diseases
- Week end episode
- Haemoptysis
With all these findings in mind we arrived to the diagnosis of Crack or Cocaine induced disease Lung.
Pulmonary haemorrhage occurs as a complication of cocaine abuse. It may present clinically with haemoptysis and dyspnoea
The pulmonary manifestations of this pathology have been related to Levamisol that is often used as an adulterant or bulk with cocaine. This drug is an immunomodulatory agent previously used to treat cancer and later as an antiparasitary drug. It produces agranulocytosis and induces autoimmunity reactions and vasculitis. ( Almeida et al 2007).
The chest radiographs may present with unilateral or bilateral ground glass densities and the CT will show ground glass opacities, generally diffuse, with interlobular septal thickening (crazy paving pattern). Other findings that have been described are centrilobular nodules and tree in bud.
In our case the disease was localized while it’s more common to see it in a diffuse pattern presentation. In those cases, dyspnoea is usually present.
Tip: Always try to correlate the findings with every detail of the clinical information.
A couple of papers related to Cocaine induced pulmonary disease.



Con esta Rx con tenues opacidades difusas como en vidrio esmerilado a predominio del LS derecho, que me descartan consolidacion o masa pulmonar pediría una TC para confirmar signos de hemorragia alveolar difusa.
Después necesitariamos saber más antecedentes, drogas? Anemia? Autoanticuerpos?
Como descarte en paciente con anemia por la edad dejaría el hemosiderosis pulmonar idiopática
Right upper lobe ill defined opacity which could pulmonary hemorrhage
Hemorragia alveolar
The chest x ray finding shows patchy infiltration at right upper lung
CT scan shows focal ground glass opacity at posterior segment of right upper lobe with associated intra/ interlobular septal thickening. No subpleural sparing is seen.
Ddx includes pulmonary hemorrhage, pneumonia(pcp), pulmonary avelolar proteinosis or ARDS