New treatments give hope to hearing impaired

Watch this session on ECR Live: Wednesday, March 4, 08:30–10:00, Room E1
Tweet #ECR2015E1 #SF1B
Hearing loss can present many difficulties and obstacles to sufferers, and with ageing populations it’s set to become a major healthcare challenge. Many conditions such as congenital malformation of the inner ear or hypoplastic cochlear nerve can also lead to hearing loss, and sometimes deafness.
Fortunately, many new treatments are available to recover hearing, both partially and completely. Imaging plays an increasingly important role in therapy planning and follow-up, and there is hope on the research front, experts will show during a dedicated Special Focus session on Wednesday morning.

Microtia – congenital anomaly of external and middle ear, resulting in
conductive hearing loss. External auditory canal is not patent (arrow),
mastoid process is underdeveloped (arrowhead)
The prevalence of auditory problems in the Western world has doubled over the past 30 years. It is estimated that between 15 and 17% of the population will suffer hearing loss, due to ageing or congenital malformation, but also bad habits, according to Agnieszka Trojanowska, a radiologist at Lublin University Medical School, Poland, who will
chair the session.
“We start to see young adults in their early 30s with sensorineural hearing loss or other related problems because of high frequency noise, which is typical for listening to music. Twenty years ago, such a condition was linked with working in fabrics or on the street. But the good news is that even if you use your iPod a lot, the degree of hearing
loss is light to moderate, so this is not something that will considerably affect your life,” she said.
To treat hearing loss, it is important to diagnose the type of condition affecting the patient. Physicians need to differentiate between two different kinds of hearing loss: sensorineural hearing loss (SHL) and conductive hearing loss (CHL). Medical treatment and imaging for these two types are very different.
In CHL, sound cannot be transmitted to the internal ear. There is something that obstructs the sound wave and the obstruction is located either in the external or middle ear. This can be removed or treated; these patients
usually undergo a CT study and, in 99% of cases, radiologists are able to find the cause of CHL, Trojanowska explained.
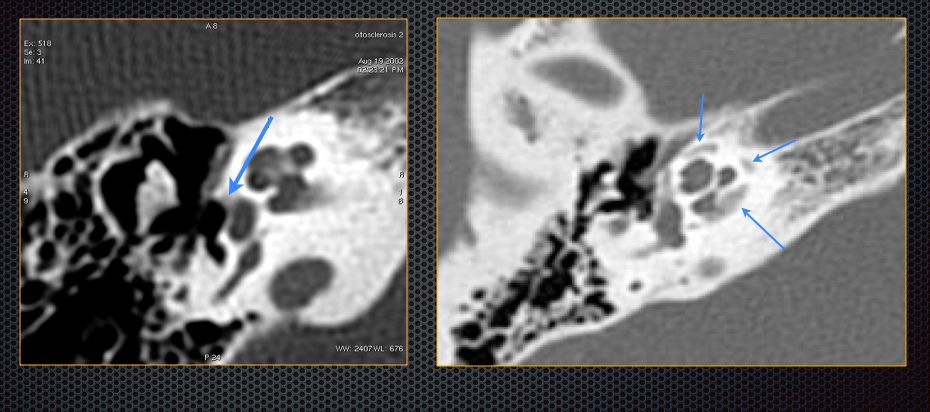
Otosclerosis – common cause of conductive or mixed hearing loss. Foci of
otospongiosis are visible in otic capsule (arrows)
“This is really great because we can help to diagnose these patients; there are absolutely no unsolved causes in CHL, everything is really simple. If we have enough experience in diagnosing temporal lobe disorders and have a good examination from the technical point of view, we can discover the cause of CHL,” she said.
Usually the reason is the presence of a post-inflammatory lesion in the middle ear, for instance cholesteatoma, or changes in the middle ear and ossicular chain; these changes usually develop due to inflammation of the ear. More rarely, squamous cell cancer, for instance a vascularised tumour, may also cause the disorder.
However, SHL is far more challenging to characterise because the cause lies within the internal ear, a complex region to show on film.
“This is the labyrinth, the cochlear nerve itself. It is much harder to image, and in most of the cases we need high-resolution MRI. We have to image the whole internal ear and, unfortunately, the whole auditory pathway, with the brain stem, the cochlear nerve, and the cerebellum. This means that there can be many reasons for SHL,” Trojanowska said.
Once the cause has been identified, surgeons can initiate treatment and chose from a very wide range of options to help rehabilitate patients.
Removal of disease and sound amplification are not always sufficient, in particular in SHL. This has inspired the development of electronic devices or implants, such as bone-anchored hearing aids, middle ear implants, cochlear implants and auditory brain stem implants, which can enhance bone conduction, provide mechanical stimulation of
the ossicular chain or stimulate the auditory nerve or auditory nucleus directly.
Some of these treatments have been used for decades, and their success in curing auditory loss, and even deafness, has led to expanding the number of patients and indications. For instance, auditory brain implants (ABI) were first used in patients with neurofibromatosis. Nowadays, children with severe congenital malformations of the
inner ear also benefit from such treatments.
These developments have implications for the work of the radiologist. Berit Verbist from Leiden University Medical Centre and Radboud University Medical Centre Nijmegen, the Netherlands, will focus on preoperative and postoperative imaging in inner ear and brain stem implants during the session. She will insist on the necessity for radiologists
to expand their knowledge to be able to help surgeons in the best possible way.

Mass in the middle ear causing conductive hearing loss. Based on
imaging findings it was diagnosed as glomus jugulotympanicum.
“For the preoperative evaluation of potential candidates we need in-depth knowledge not only of diseases, but also of treatment options and operation techniques in order to provide an accurate description of images in a way that
is relevant to the surgeon, thereby helping them to decide on optimal treatment choices in individual patients. For instance, the presence of vascular anatomical variants may hamper a surgical approach through the mastoid, and the presence of ossification in the inner ear may alter the choice of cochlear implant type. These imaging findings will influence the treatment plan, the choice of side of the operation, the choice of device, etc. Of course, imaging findings have to be combined with clinical findings, audiological findings, and cognitive status of the patient before making final decisions,” she said.
In the postoperative phase, radiologists might be asked to evaluate patients who do not present with the desired outcome. Again, radiologists need to be acquainted with the materials and devices used to be able to recognise normal postoperative images as well as complications after surgery.
SHL in the paediatric population is a crucial issue, and it will be tackled during the session. One child out of every 1,000 is born with SHL, usually due to some congenital disease or malformation of the inner ear. The consequences can be very serious for these patients, who may not be able to develop speech.
Radiologists have to image the inner ear to know if an implant can be put into the cochlear. Cochlear implantation is increasingly used because it has a very high success rate and the procedure is quite simple, quick and safe.
In more complicated cases, such as aplastic or hypoplastic cochlear nerve or absence of cochlea (congenital malformation), MRI may also help to determine whether the cochlea is well developed and contains a nerve. Some children are born without any cochlea and cannot benefit from this treatment.
MRI is also useful for evaluating adults who are candidates for cochlear implantation, by helping to find the cause of hearing loss – for instance dissection of the vertebral artery or small infarction in the
cerebellum.
After implantation, if the implant stops working, MRI can help to determine the causes, which may be implant misplacement or anatomical changes in the cochlea or surrounding structures.
“The radiologist is now the partner of the ENT surgeon, helping him or her to decide upon the type of the implantation and the qualification for the implantation. So this is like a multidisciplinary team, and there are many ways we can help these patients,” Trojanowska said.
In most cases, if the nerve is present, patients can recover hearing with an implant. Surgeons are also starting to use bilateral implants in order to have stereotactic hearing, a significant improvement in the quality of life.
Trojanowska also wants to address sudden hearing loss, an increasingly frequent condition. “We as society have to take into consideration the fact that there is a greater percentage of sudden hearing loss, which is mainly caused by infarction and haemorrhages of the brain. Our population is ageing, so the percentage of brain infarct is increasing,” she said.
Next to diagnostics and individual treatment planning, imaging also plays an important role in research on auditory rehabilitation. Verbist will show in her presentation how useful imaging has become in planning the outcome of novel treatments, by evaluating implant designs, giving feedback on surgical techniques and correlating intended
results with outcomes.
She will explain how imaging of cochlear implants (CI) helps to show the large variability in outcome in this patient group.
“We have been able to reach a better understanding of the reasons for that variability, particularly regarding the cochlear implant. The implant has several contacts, and every contact stimulates several neurons of specific frequency. We’ve been able to help in understanding how the position of such a contact influences the outcome,” she said.
The inner ear is a very small structure and it differs from one individual to the next. “So for instance if you implant a CI of a certain length in a large inner ear, it will not be as deep as in a very small inner ear. Also the
type of implant used and the surgical approach influence the final position. Those are the things that we can look at,” she explained.
She prepared her presentation with an oncologic surgeon, emphasising the need for a multidisciplinary approach in ENT patients. “It’s really necessary to keep up with all the developments. I always try to provide reports that are really useful to the surgeons, so I try to understand what their questions are, what is the information they need to talk to their patients about and to treat,” she said.
Special Focus Session
Wednesday, March 4, 08:30–10:00, Room E1 #ECR2015E1 #SF1b
SF 1b Up-to-date imaging for hearing loss
» Chairman’s introduction
A. Trojanowska; Lublin/PL
» New devices in the treatment of hearing loss
B. Ozgen Mocan; Ankara/TR
» Pre- and postoperative imaging in middle ear implants
E. Loney; Bradford/UK
» Pre- and postoperative imaging in inner ear
and brainstem implants
B. Verbist; Leiden/NL
» Panel discussion: Changing demands for imaging
in hearing loss


I am very interested in this article as I have a 7 year old female child who has been shown by MRI to have a weak hyperplastic nerve to her left ear. She is profoundly deaf to she left ear as well, right ear is fine. She had her first few baby words which disappeared as the disabilities progressed around 18 months so she now has no speech. I would like advice in the best possible treatment since tests show that both her cochlear are good. Consultants are now at a stage to review the best possible treatment and outcomes