José Vilar and Friends Case 27 (Update: Solution!)
Hello friends,
I hope you are doing well wherever you are. Here things are not too good but for the moment I am well.
Here is a case just brought from Dr Peset University Hospital in Valencia.
71 year old man who had a syncope and is brought to the Emergency Room. The COVID 19 ARN (RT-PCR) is negative.
What do you think and what would you do?
Solution:
Dear Friends,
This case is intended to discuss some of the features of CV19, and the pandemia that is already installed in the entire populated world.
Our patient, 71 years old had a syncope and was sent to the ER. The COVID 19 ARN (RT-PCR) was negative.
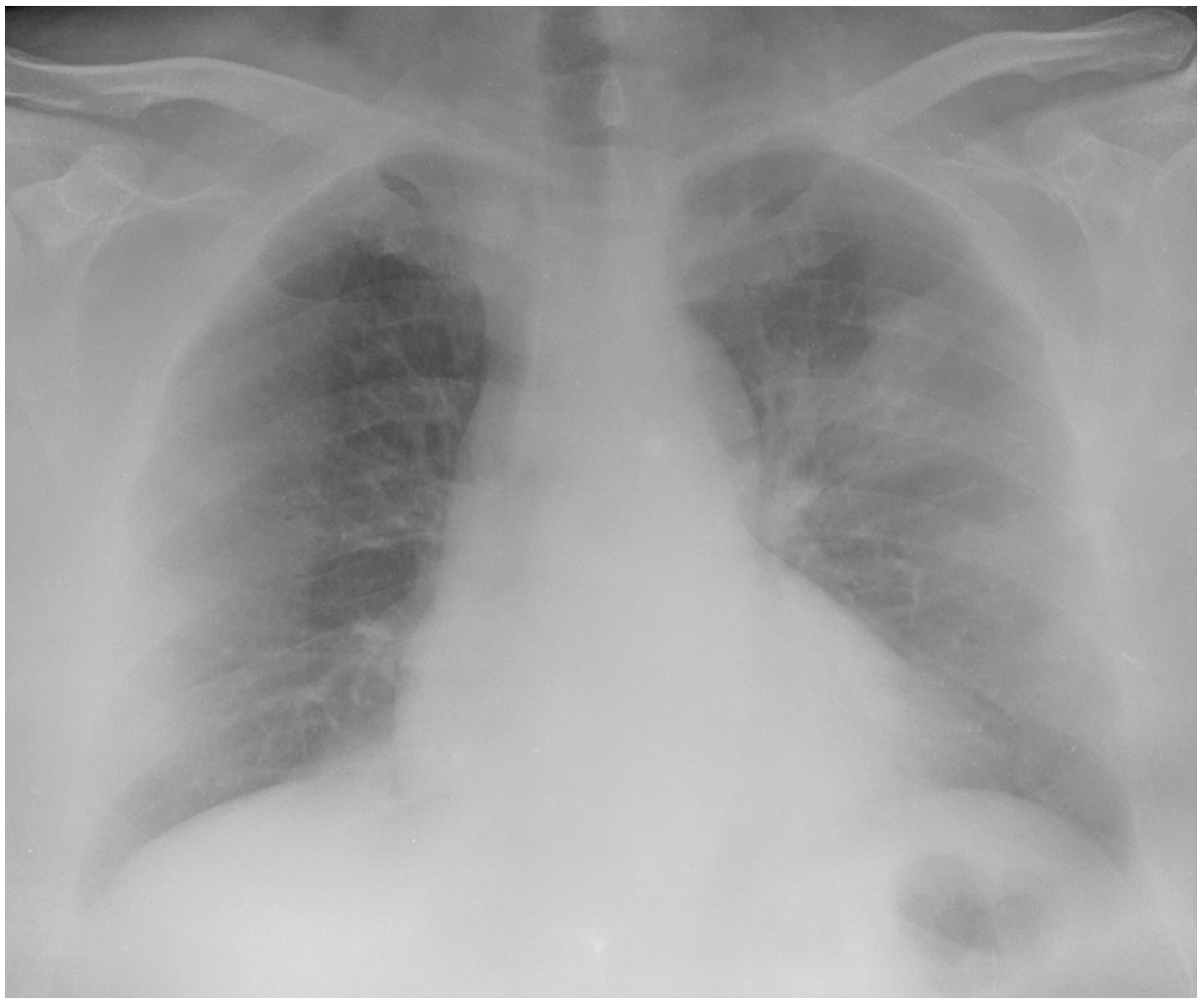
A portable chest radiograph showed two very poorly defined opacities in the middle lobe area and the left upper lobe. (arrows)
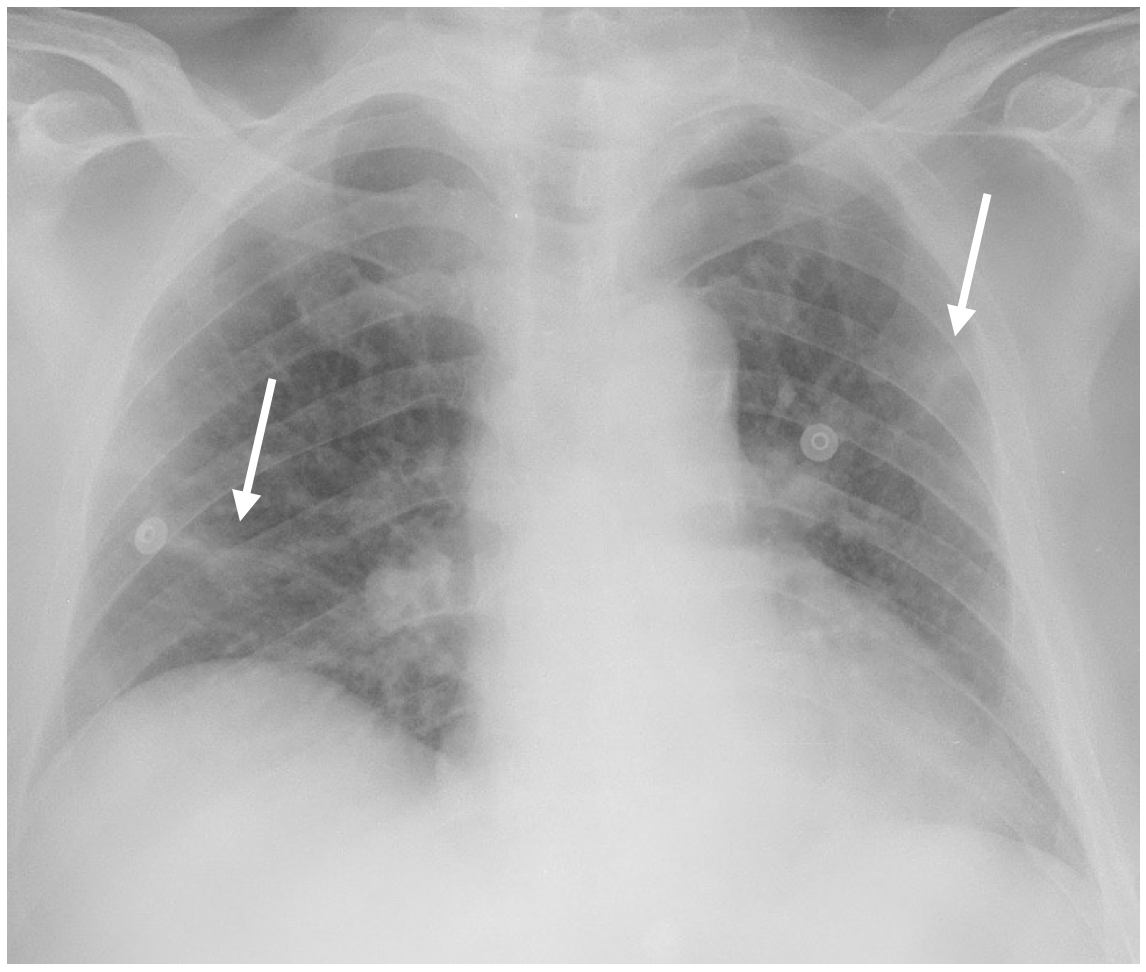
AS very well indicated by E. Lorente even in the absence of a negative test, the presence of pulmonary involvement suffices to treat this patient as positive for coronavirus.
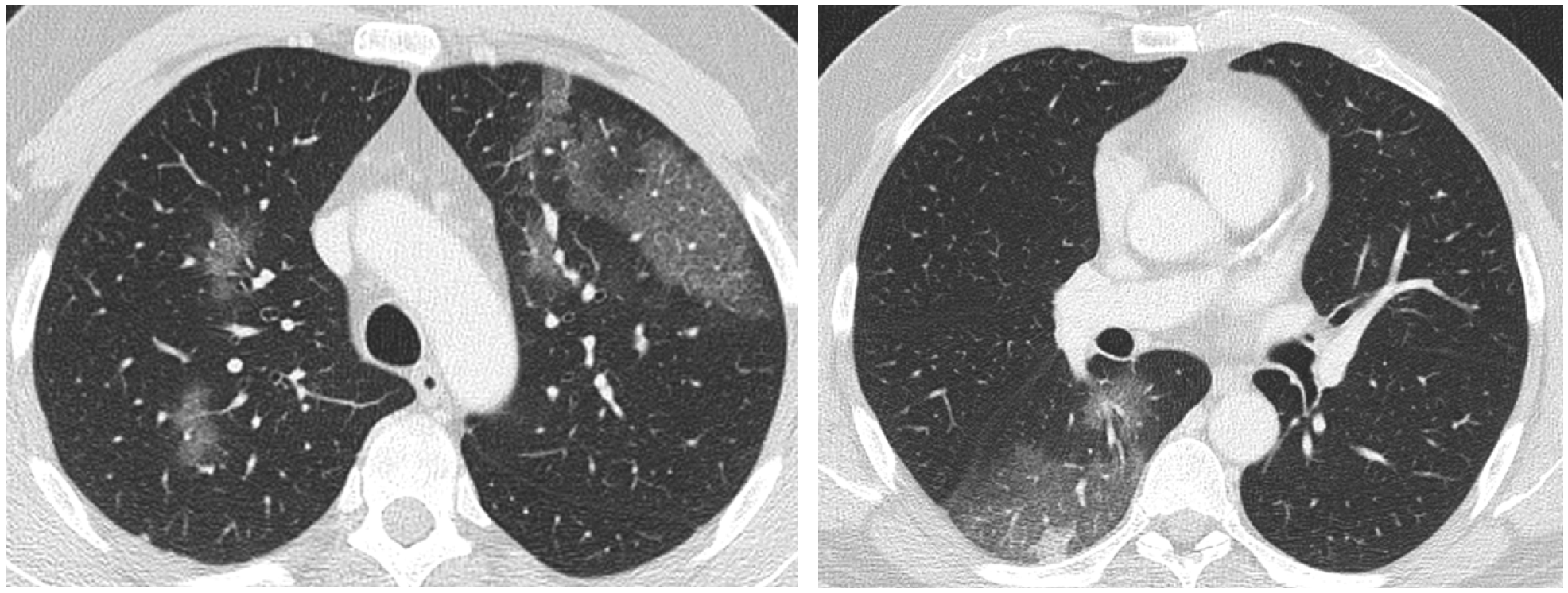
In view of the poor quality of the portable radiograph, a CT was performed the following day. Ii the CT, lung window settings, there are several patchy areas of ground glass density in both lungs, most of them peripheral.
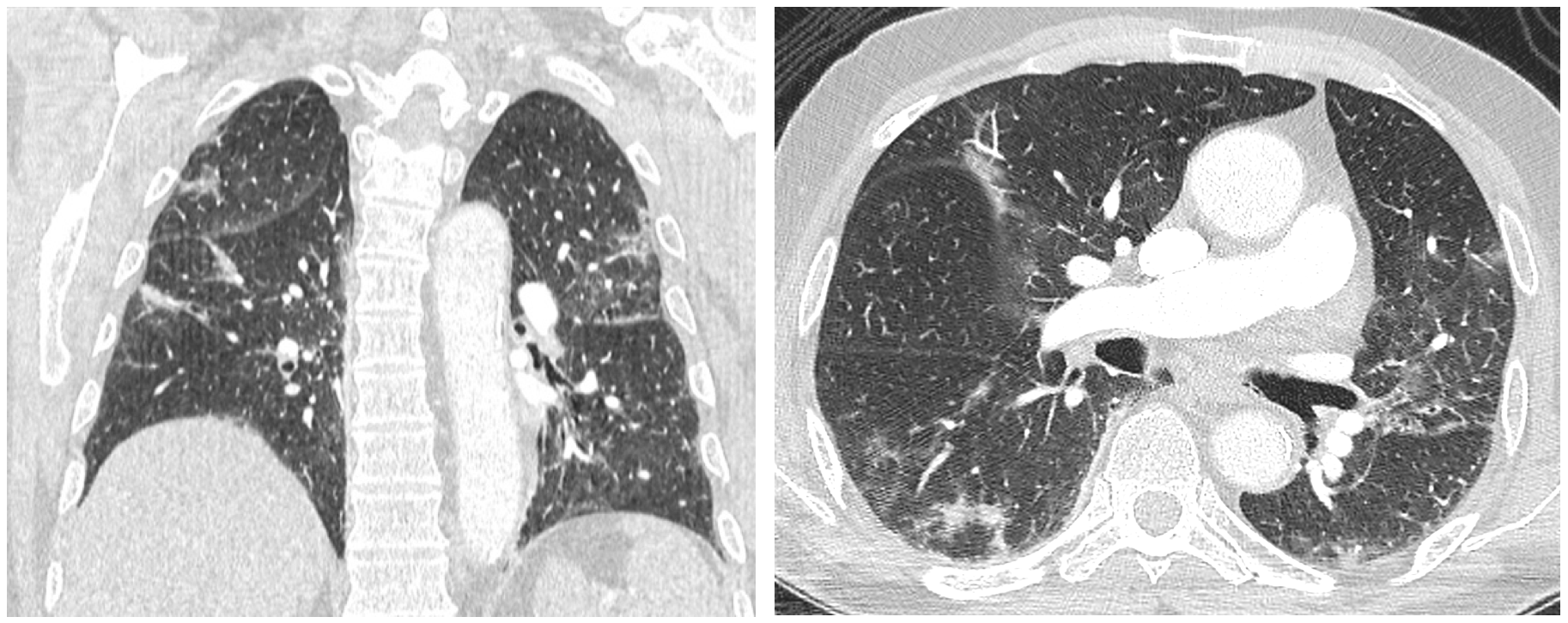
A second test was positive for CV 19.
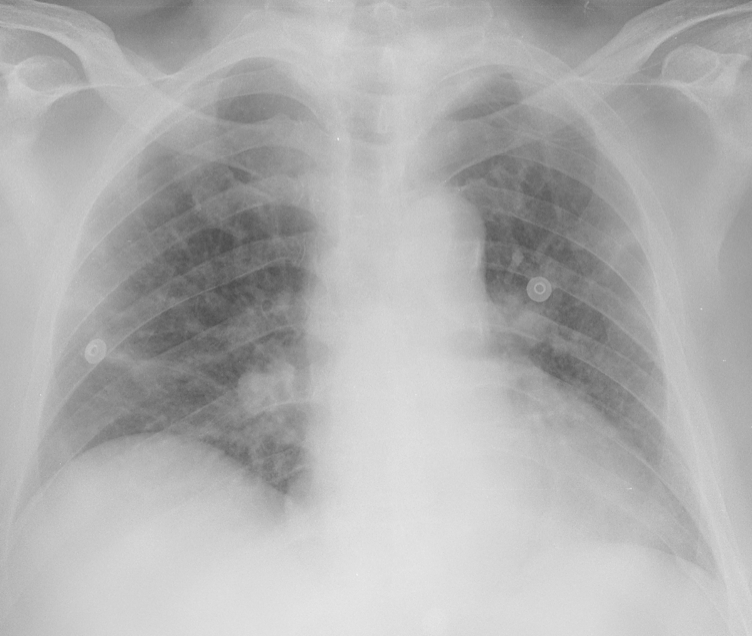
Another case: 50 year old patient with dry cough, fever and diarrhea.
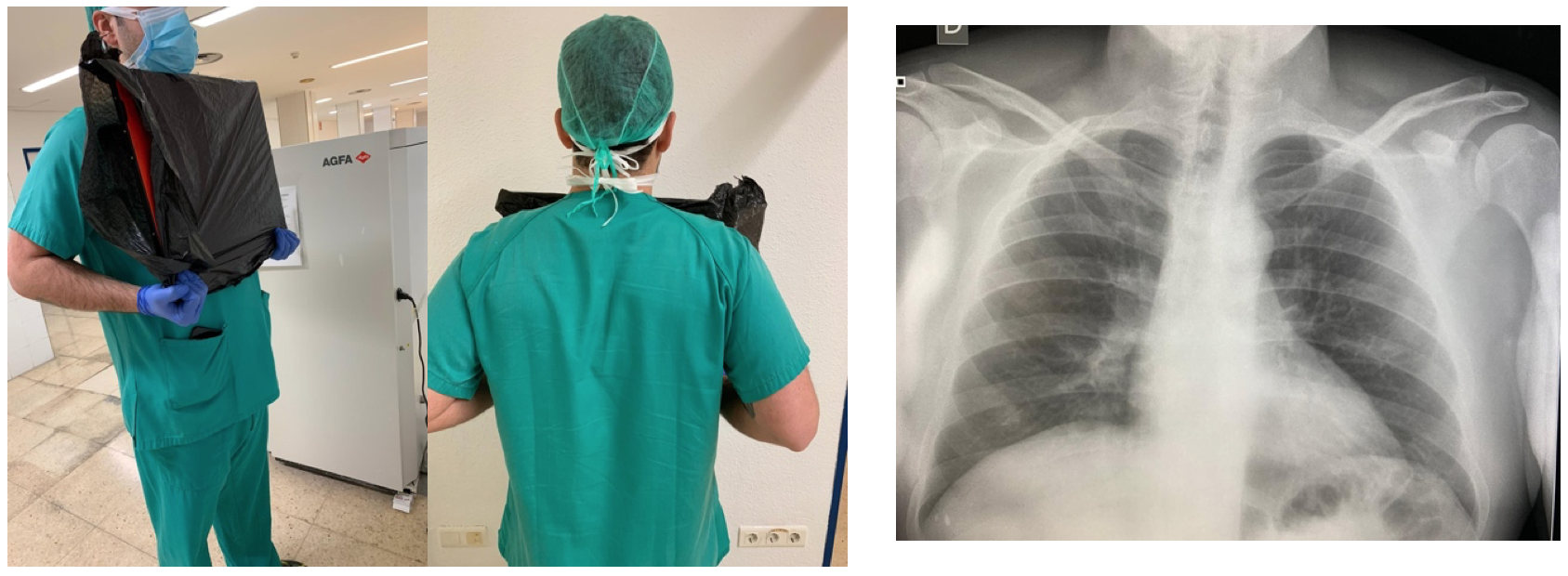
This portable CR shows clearly an opacity in the left upper lobe. Note how the scapulae may obscure the peripheral areas of the lungs.
The CT in this case shows involvement in both lungs. There is more information as compared to the portable radiograph, but this CT did not change the management of the patient.
These cases illustrate several interesting features of CV 19 related to radiology.
The presence of pulmonary involvement is very frequent and may help in the management of the patient.
Portable chest radiographs have a limited capacity because the supine position, the absence of a grid , the overlap of the scapula, and even the distance of the tube provide images difficult to interpret.
CT, as we know is much better to see pulmonary disease, but is it necessary?.
What can we do as radiologists:
- Facilitate the possibility of obtaining chest radiographs in a specific area isolated from other areas of the radiology department: Dedicated portable machines in ICU and Emergency areas.
- Not all hospitals have the possibility of having dedicated rooms, or have the newest technology (DR). You must adapt you department to what you have.
- When performing a portable (CR or DR) radiographs in the ER, when patients may stand up, one of our Technicians ( A. Cuenca) suggested a tip: To obtain the radiograph with the patient holding the cassette as indicated in these images.
The cassette is covered adequately in each patient, and the image obtained has the quality of a regular PA chest radiograph.

- CT is usually not necessary in our environment unless other pathologies (P. Embolism for example) are suspected or chest XR are inconclusive
- Another scenario is that of emergency patients that need immediately a CT and there is no time for a PCR. In those cases, apart from the CT of the specific anatomic region (Head, Abdomen, etc.) the chest is also scanned to rule out signs of COVID 19 and to protect all the potential personnel involved. If signs of CV19 are detected all the involved personnel can be alerted and proceed as programmed with other infected patients.
- Although we do not have experience with ultrasound of the lung, we know that it has become a very interesting tool, not only in the ICU, but also, as I am told, in primary care in some countries ( Italy for example) where family doctors may scan patients in their home and find if there is pulmonary involvement, and thus decide if patients have to be hospitalized.
Conclusion: Radiology has a major role in the diagnosis and control of COVID 19. The surprise (not for me of course) is that the old chest radiograph has come to the first raw in the management of this disease
Different societies have published documents related to the use of radiology in COVID 19 and I suggest you look in the webb if you have more questions. Our Spanish society (SERAM) has an excellent document (https://covid19.espacio-seram.com/index.php).
The Radiologica Society of North America has also released an excellent document:
( Consensus Statement).
https://pubs.rsna.org/doi/10.1148/ryct.2020200152
My best wishes to all of you, wherever you are.
Special thanks for their help in this topic to. Dr. Santiago Isarría (Hospital Universitario Dr. Peset, Valencia) and Dr. Pilar Calvillo ( Hospital Universitario y Politécnico. La Fe, Valencia).


There’s ill-defined bilateral alveolar opacities (more evident in middle lobe and left superior upper lobe). Due to epidemiologic context and despite negative PCR, these findings can be found on SARS-CoV-2 infection (it has been reported anosmia, syncope and other neurological disorders).
I would manage this case like a COVID-19 pneumonia and would repeat PCR in 2-3 days. CT scan could be performed, but I think it wouldn’t change pacient management.
Mitral stenosis
Peripheral subpleural infiltrates. Our centre has adopted CT chest imaging to be performed concomitantly if this patient were for eg to be referred for a CT Brain in view of his syncopal episode. If CT findings confirm ground glass change, subpleural sparing, ‘reverse-halo sign’ and no definite alternative diagnosis – isolation and repeat testing for COVID would be recommended.