José Vilar and Friends Case 43 (Update: Solution!)
Dear Friends, let me challenge you with two cases of the same disease.
Case A: this is a case also brought to me by Drs Isarría and. Dr. Ruiz from Hospital Universitario Dr. Peset. Valencia.
73-year-old male with cutaneous lesions.
Case B: This is a case from my files: a 50-year-old man with neurological symptoms

My questions about these two cases are:
Where is the pathology in case A and case B?
What is your diagnosis?
Additional information:
Well, friends, you are very good and some of your comments fit perfectly this case.
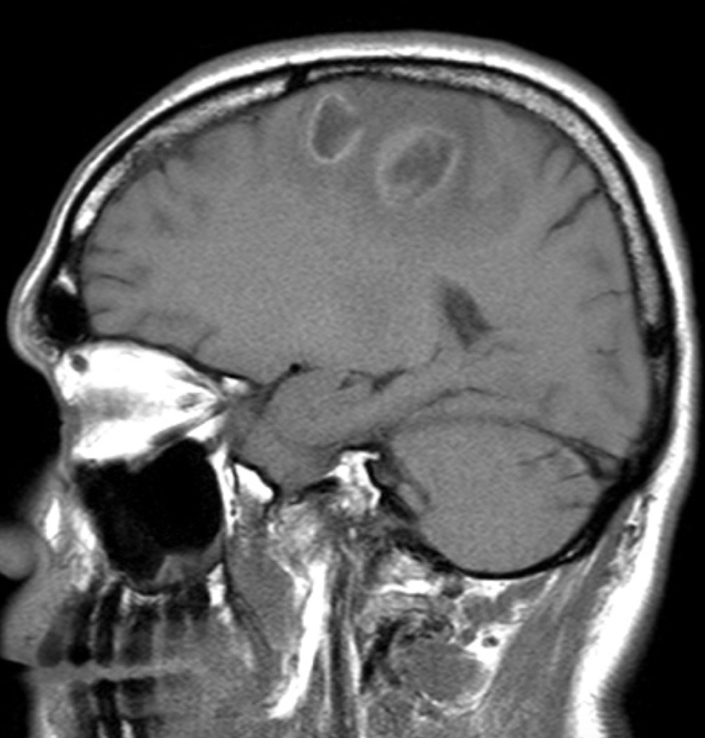
Regarding case B, let me add an image to see if you can explain the findings.
Click here for the answer
Well, this case was followed by many people and, what is more important, was diagnosed by most of you very precisely, and by a few very quickly. I am proud of you.
Let me run through the images and the findings.
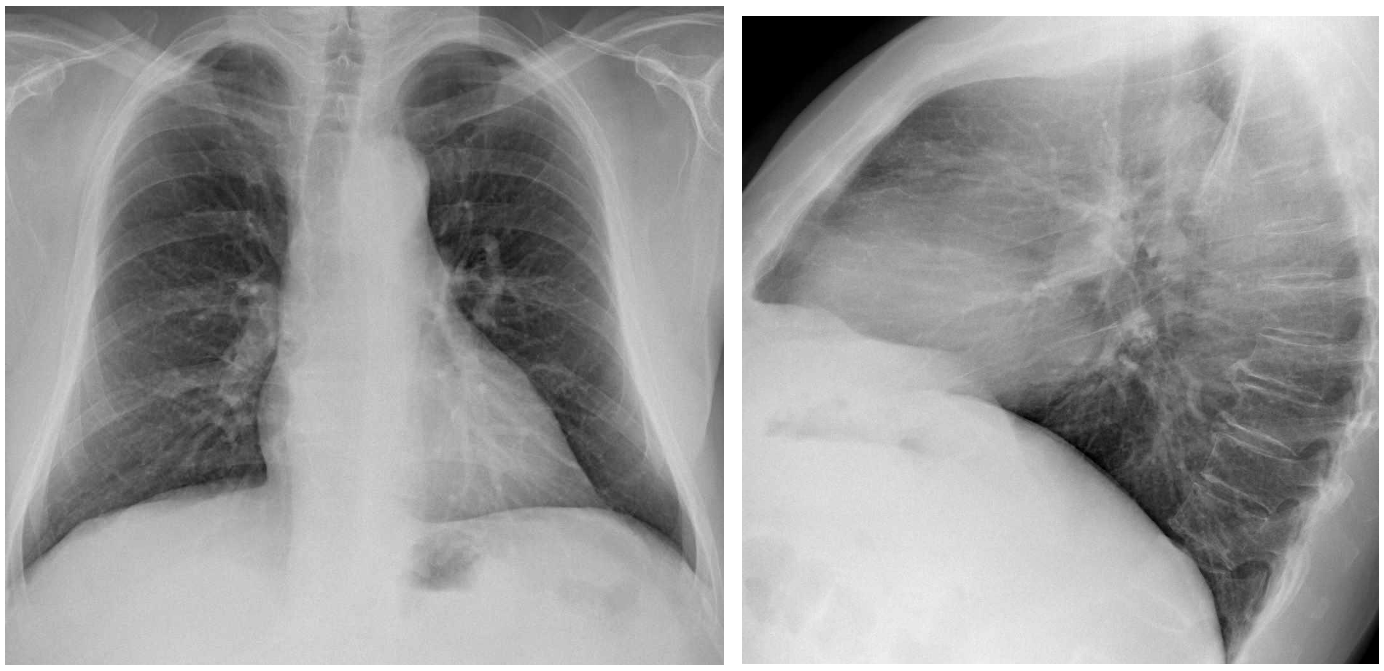
CASE A:
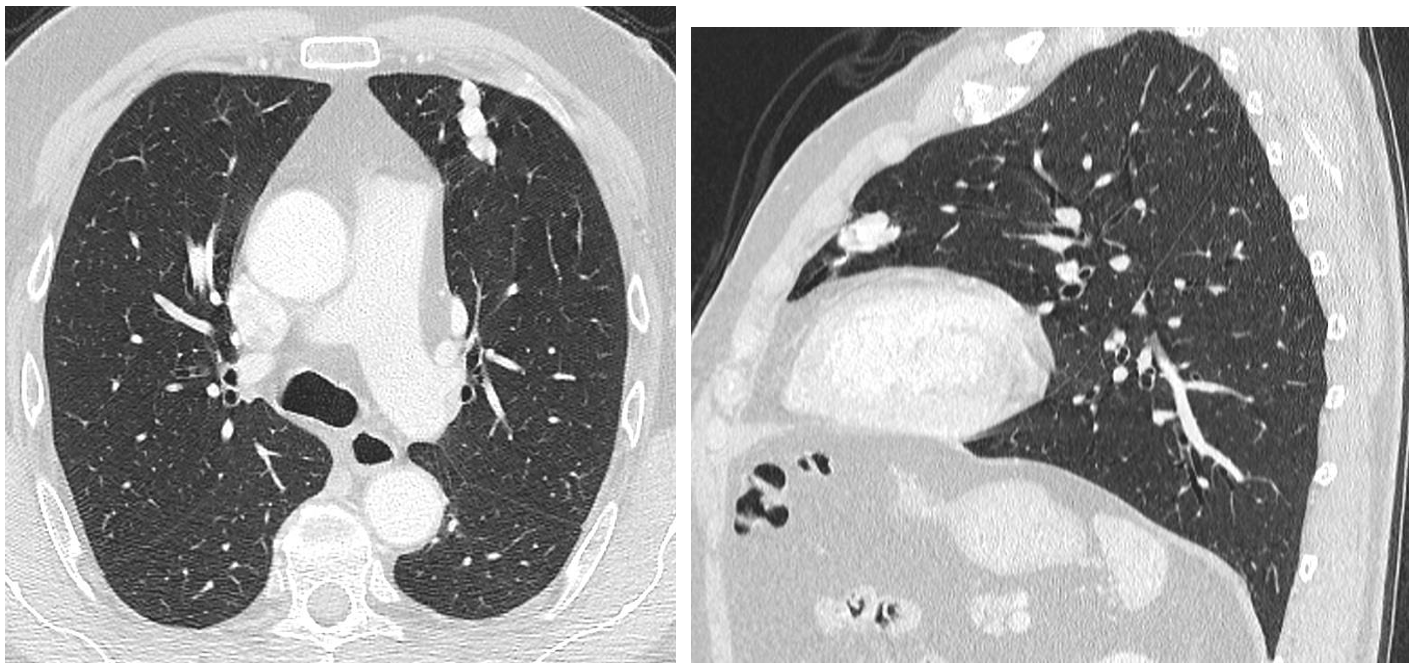
A tubular structure is seen in the left lung (arrow) and also identified in the lateral projection in the anterior clear space (arrow). This suggests that the lesion is a vessel. The differential diagnosis could be between an abnormal meandering vein (abnormal tortuous vein draining into the left atrium), or an arterio-venous malformation,
The CT shows the lesion with a vessel like morphology. The contrast images and MIP show that this long vessel has an arterio-venous trajectory and a central nidus, indicating that it is an arteriovenous malformation (AVM).
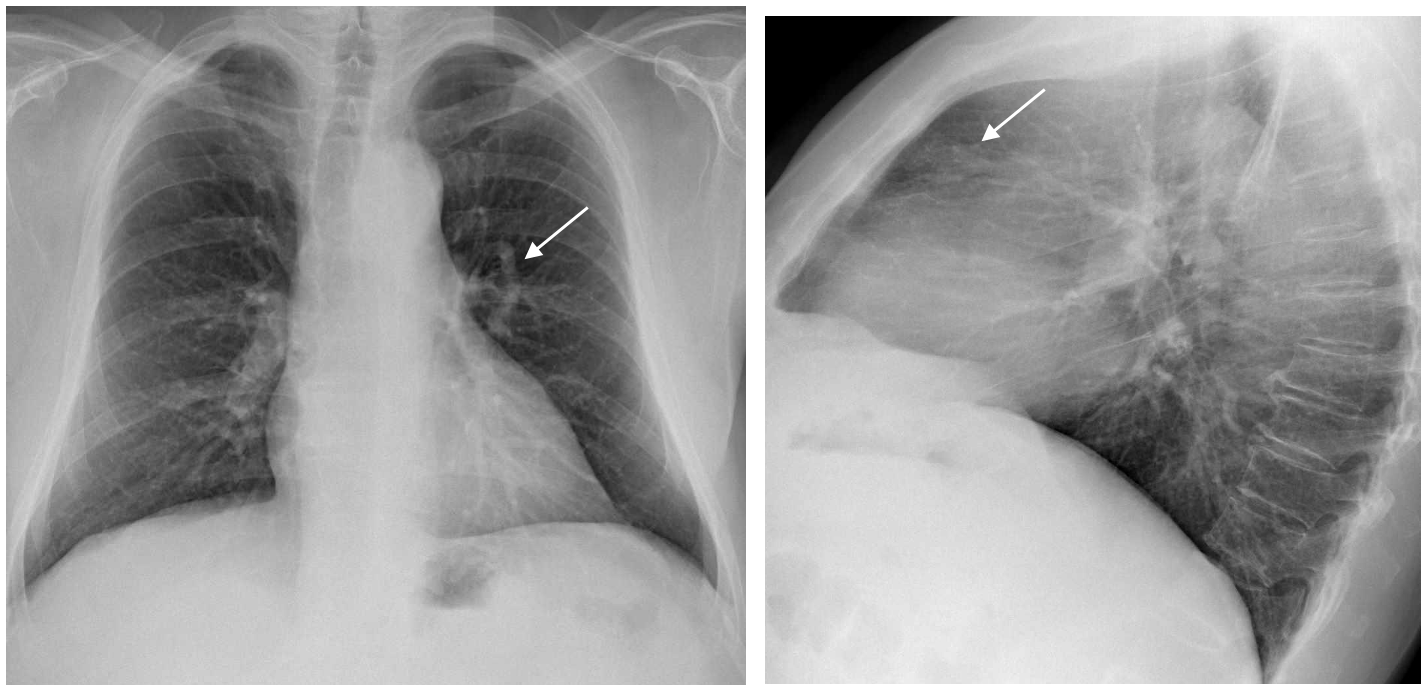
CASE A:

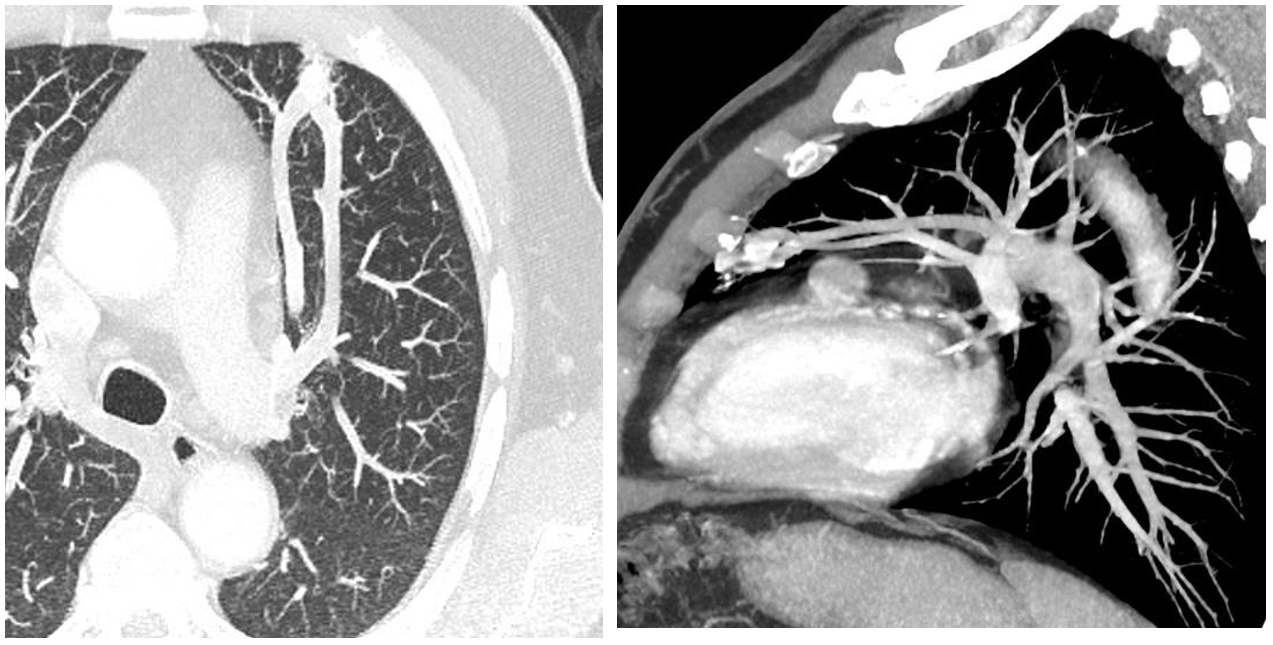
In this case another tubular lesion pointing towards the hilum is seen in the left costophrenic region.

The contrast CT shows that the Vascular structure has a peripheral nidus, an artery and a vein, better seen in the 3D reconstruction (Small arrows): This is another Arterio-venous malformation, but this patient had more findings related to his neurological symptoms.

Brain MRI (Sagittal contrast T1 weighted sequences) show hypointense rim enhancing lesions consistent with abscesses.
DIAGNOSIS: Both cases are examples of arteriovenous malformations in the lungs. The first one (Case A) is a case of Rendu-Osler-Weber syndrome also called hereditary hemorrhagic telangiectasia. This patient indeed had telangiectasias, and recurrent epistaxis. Along with the AV malformation these are criteria of Rendu-Osler-Weber syndrome.
This is a rare inherited disorder characterized by abnormal vessels in the skin, mucous membranes, and organs such as the lungs, liver, and central nervous system. The main criteria for the diagnosis of this entity are:
- Telangiectasias
- Family history
- Repeated epistaxis
- Arterio-venous malformations
This was the case in Case A.
In Case B, the AVM was isolated and not clearly related to other criteria of Rendu-Osler-Weber syndrome.
Regarding pulmonary AVM:
The main radiologic findings described in the lungs are seen in our two cases. A vessel like structure in the lung, with a feeding artery and a draining vein identified in contrast CT.
Arterio- venous malformations may be solitary or multiple. The chances that the patient has a Rendu-Osler-Weber syndrome are higher when the lesions are multiple.
Pulmonary Arterio-venous malformations may complicate with haemotysis or shunting problems such as paradoxical emboli, as in case B, due to the fact that there is a left to right shunt.
In symptomatic cases the AVM can be resected or preferably embolized as we did in this case (B).
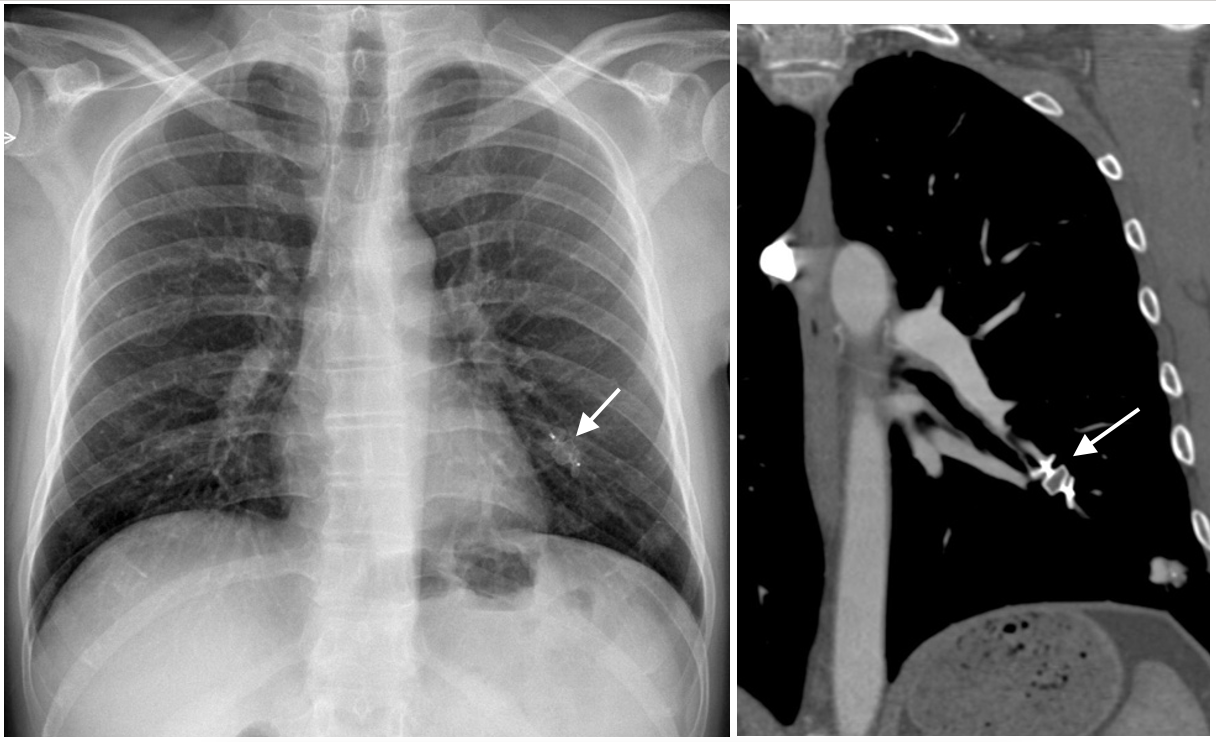
After permanent occlusion via embolization of the AVM the Amplatzer device is seen in the left lower lobe. (Arrow)
Points to remember:
- If you see tubular structures in the lung in a chest radiograph, think of AVM or other vascular malformations, and proceed to a contrast CT.
- Contrast CT will easily reveal if this is an AVM showing a feeding artery, a draining vein and the connecting nidus. Remember to look carefully for additional AVMs in cases of Rendu-Osler-Weber syndrome.
- Brain complications may occur in left to right shunts (paradoxical embolism), especially at the foramen ovale, but also in pulmonary AVM.


For case A there is tubular like structure left perihilar area,
Case B nodular opacity in left Lowe zone (near costophrenic angle),with tubular like structures connected to left hilum in keeping with AV malformation
The diagnosis might be Hemorragic hereditary Telengectasia
As patient with skin lesion it might be telengctasia, and the other patient with neurological problem it might be Av malformation in the brain
remembering your very first sentence that both cases are having the same disease i am commenting on the cases.
case-1- pathology is in ribs in the form of thin ribbon like ribs, erosions, notchingetc the right upper ribs and left 3rd rib. suspicion of cervical rib rt side, soft tissue thickening left chest wall plexiform neurofibromatosis. mild kypho scoliosis with ant mild compression of vertebra.
left paravertebral soft tissue shadow lateral to descending aortic shadow.
case-B shows convex soft tissue shadow rt upper dorsal paraverebral region- neurofibroma or lateral thoracic meningocele
left costo phrenic angle region shows tubular shadow ending with nodular opacity like that of AVM
POSSIBLE DIAGNOSIS -NEUROFIBROMATOSIS TYPE-1
Case A: There is a nodule located at the left retrocardiac space (left lower lobe).
Case B: There is a nodular lesion at the left costophrenic angle with a prominent vessel leading to this.
The findings are most probably AVMs.
The cutaneous lesions in case A are telangiectasias and the neurological symptoms in case B are caused by cerebral AVMs or aneurysms.
The diagnosis is Osler-Weber-Rendu syndrome.
I have been thinking about the differential diagnosis list of hypervascular pulmonary lesions/ possible AVM, combined with cutaneous lesions, bone lesions and neurological symptoms. Also the two cases being adult males.And the fact that AVM can be congenital or acquired. For Oslo-Weber-Rendu and NF1 we have criteria, some of which are clinical and we do not have that part of the information. There is also great mimickers like sarcoidosis and metastasis that can simulate AVM. But at the end I started thinking about liver cirhosis, both patients being adult males and that AVM can be a manifestation of liver cirhosis.I stretched futher thinking about hepatocellur carcinoma and A1-tripsin deficiency in males.So I think liver chirosis with the risk for hepatocellular carcinoma should also be on the differential list. And in everyday work I will gather as much information for the patient as possible.
CECT Brain with two hypodense lesions in the frontal lobes,showing ring enhancement and surrounding edema. most likely Brain abscesses
As there is Pulmonary AV malformation it increase the risk of Brain abscess due to direct mix between venous and arterial blood without filtration at capillaries level
So the diagnosis still going with Hrerditary H aemorrgic Telengectasia (osier-Weber-rendu) with pulmonary AV malformation and complicated by Brain abscesses
Again thinking about differentials for the ring-enhanced lesions surrounded by edema on this MRI image, I am thinking mainly about abscess and metastase/malignancy. I am also contemplating tuberculotic granuloma a little bit, but it somehow does not fit.
I am not thinking so much about brain AVM, because I think they usually do not go with so much edema and look slightly different on MRI.
Abscess goes well with the possibility about pulmonary AVM and their neurological complications due to septic/aseptic paradoxal emboli, that can lead to stroke or abscess in the brain. Again it is diffucult to distinguish abscess from metastase/malignancy just based only on this image, so malignancy still cannnot be excluded.DWI can be helpful.Also chest CT.
The most probable diagnose for me is a neurological complication from pulmonary PVM.Still as a mimic malignancy should still be contemplated.
Excellent discussions ! I will give you the answer next Monday.
Waiting for that Sir
Thank for your time and for sharing these interesting cases.
Appreciated