Today I am showing a case provided by my former resident and good friend Dr. Nadine Romera. Images belong to an 87-year-old man with TB in the past. He presents now with loss of weight and low-grade fever.
What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
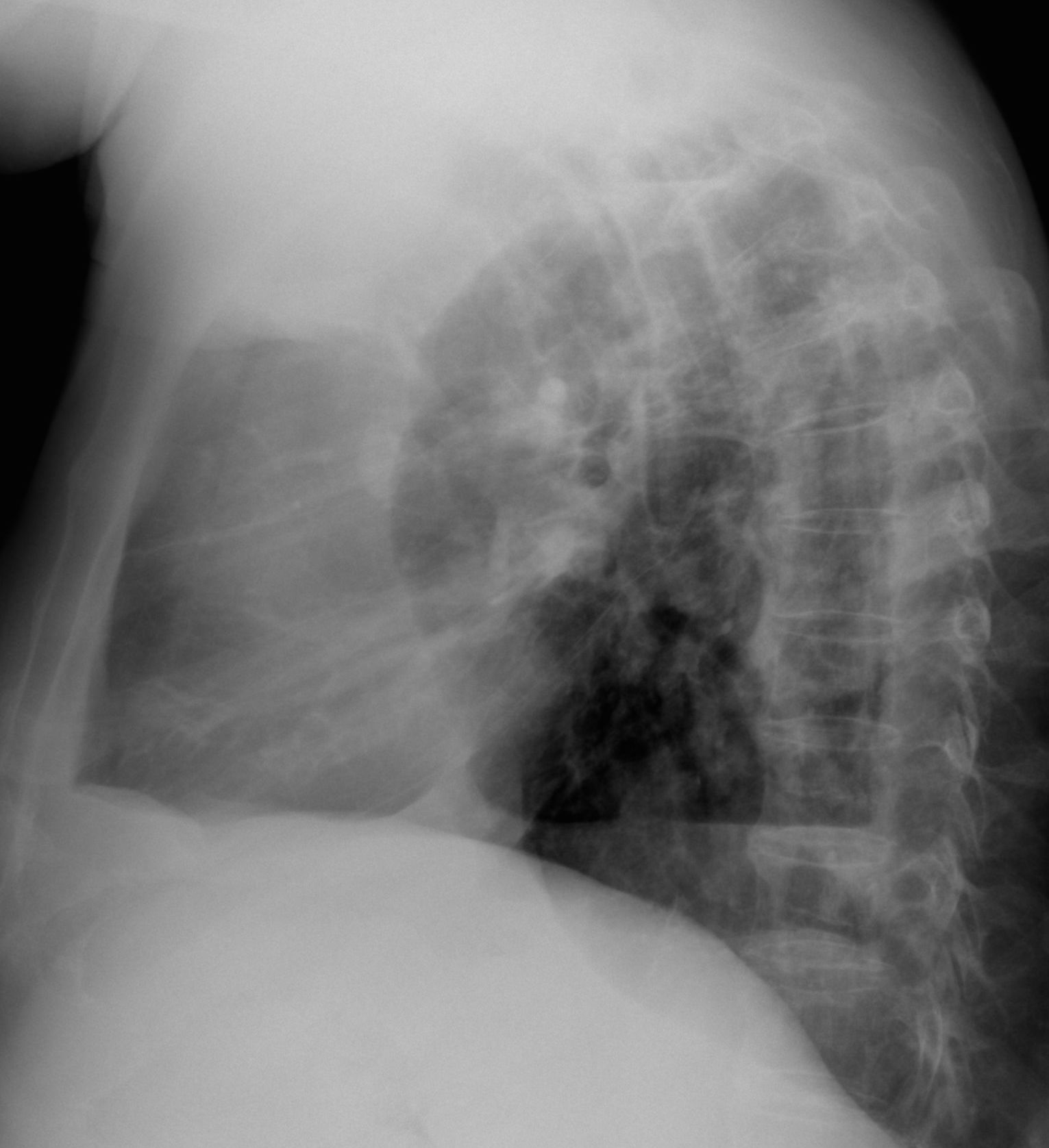
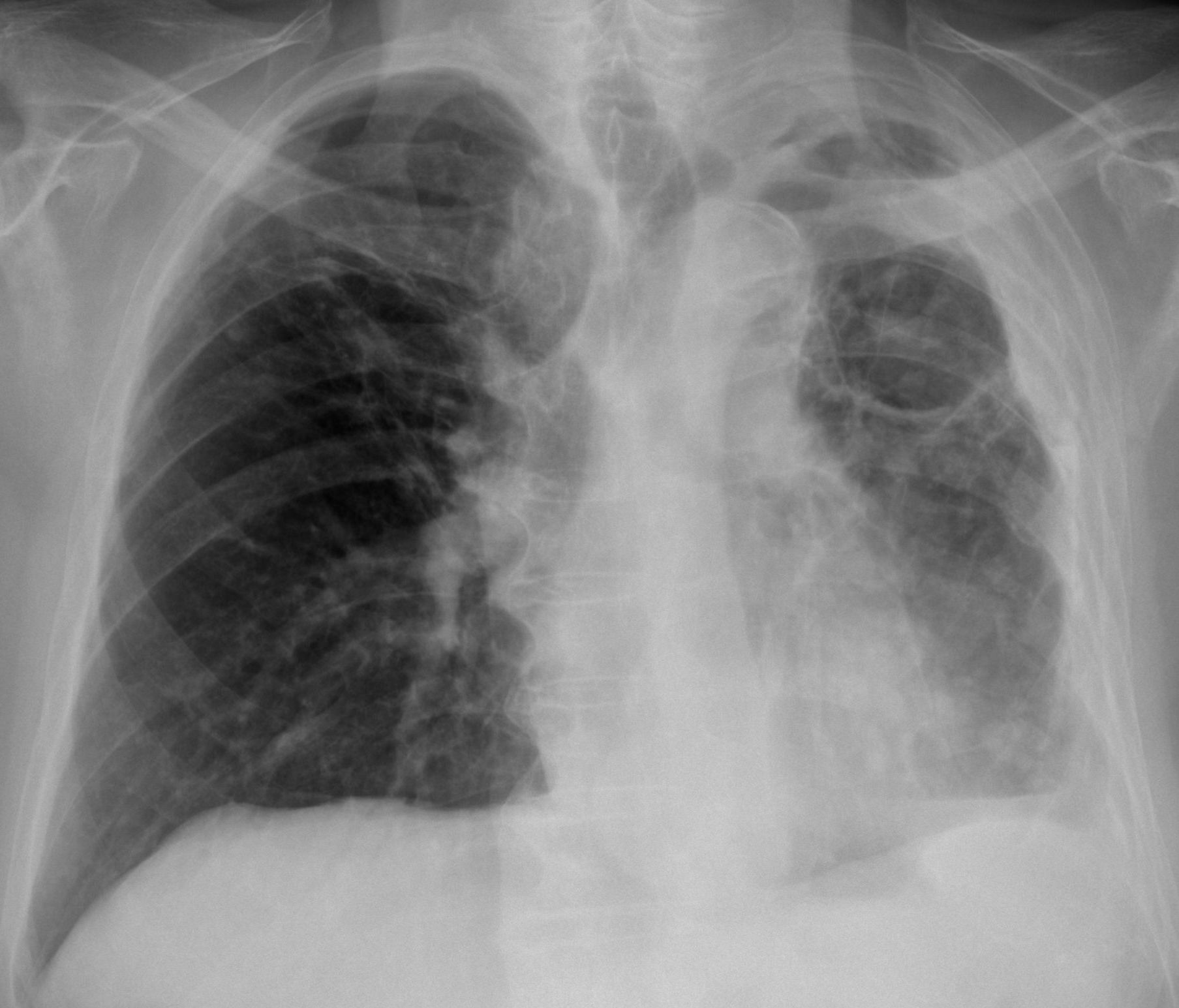
Findings: PA radiograph shows a small left hemithorax with pleural thickening (A, arrows). Chronic changes in both lungs are visible. In addition, two air-fluid levels are seen in the pleural space (A-B, red arrows). With these findings, the first diagnosis that comes to mind is chronic pleural disease with broncho-pleural fistula.

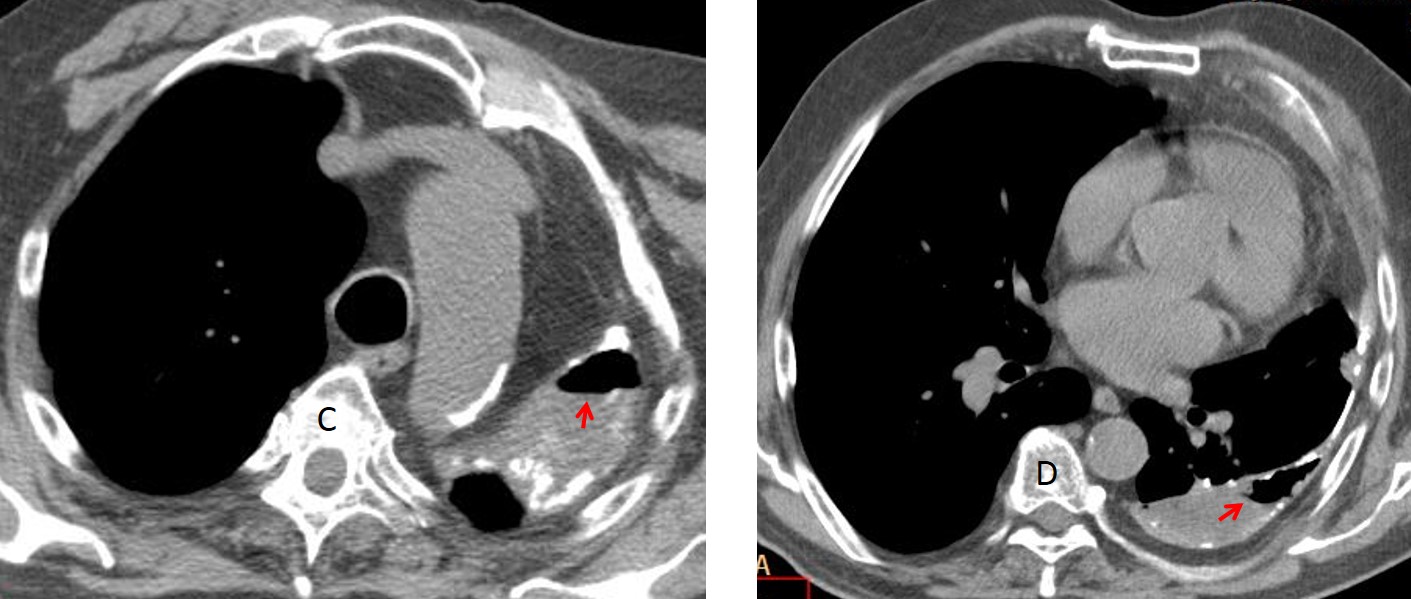
Axial CT shows the calcified pleura with loculated fluid and air-fluid levels (C-D, arrows), confirming the suspicion of broncho-pleural fistula.
CT also demonstrates a small pleural mass that was overlooked in the initial examination, made in October 2014 (E, arrow). A follow-up CT three months later shows an increase in size of the mass (F, arrow) with a rim of increased uptake in PET-CT (G, arrow).
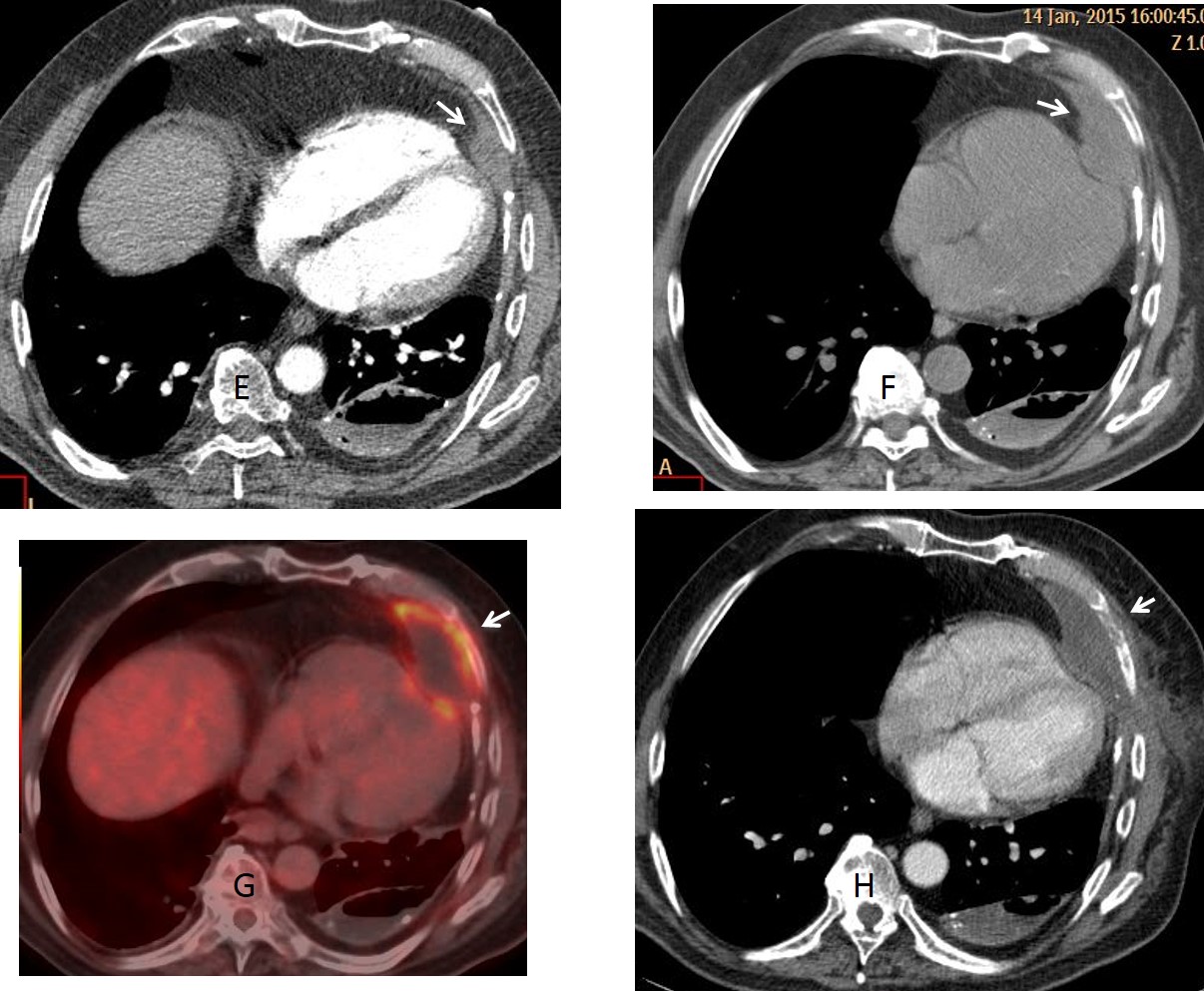
Percutaneous biopsy came back as lymphoma. While in treatment, CT one month later shows invasion of the overlying rib (H. arrow).
Final diagnosis: Chronic pleural changes with broncho-pleural fistula and secondary lymphoma.
Congratulations to all of you who made the correct diagnosis. Cannot single out anyone. The lymphoma is obviously not seen in the chest radiograph and, as a matter of fact, was missed in the first CT.
Teaching point: the presence of an air-fluid level in chronic pleural disease is practically pathognomonic of broncho-pleural fistula. In this particular case, the associated lymphoma is a serendipitous finding. It is well know that malignant tumours are a complication of long-standing inflammatory pleural disease (see Caceres’ Corner case 34)


Dear sir
Subject in subtle rotation .
Subtle tracheal shift to left.
Destroyed lung architecture left side.
Doubtful cavity formation left upper lobe with thin walls.
Veil like haziness left lung lower zone with obscuration of left CP Angle – pleural thickening/ minimal effusion.
Subtle infiltrates Rt lung upper zone.
Doubtful SPN insitu left upper zone cavitory focus.
Unfolding of Aorta with aortic knuckle calcification.
Changes of osteopenia
Volume loss in left hemithorax with diffuse pleural thickening/effusion and air-fluid level in left hemithorax, likely in pleural space. Suggest tuberculous empyema.
left pleural effusion with left upper lobe collapse(or operated tb lung but i can’t see old ribs fracture) and bullae with Air fluid level on the left cap.
i can see also mediastinal calcified lymph nodes and pleural calcifications post tb
– reactivation tuberculosis?
– aspergilloma?
– ca?
I see air-fluid level on the left side, my be from hydropneumothorax.
I suppose there is a tuberculous empyema or even bronchopleural fistula (BPF) which is a rare complication after reactivation of TB.
I see tracheal deviation to left, with smaller left hemithorac suggesting volume loss in that side. There are two big thin walled cavities in which one of those has an air fluid level. I think it’s reactivation TB with TB empyema.
Reduced left lung volume with air fluid level in left basal lung region. Probably thin walled cavity in left upper zone. Left lateral chest wall and apical pleural thickening. Hyperinflated right lung with deviation of trachea to left and midline herniation of right lung. No significant mediastinal and hilar lymphadenopathy.
Impression left sided reactivation of pulmonory TB with left lung empyema. Ct will be helpful for further management.
…in attesa del “triplete” provo io a fare goal al mitico Professore….esiti di pachipleurite TBC, con ipoespansione del polomone sx e “shift” a sx dell’ombra cardiomediastinica….il nuovo: il livello idroaereo confinato nel cavo pleurico posteriore a motivo delle vecchie aderenze pleuriche….il livello idroaereo potrebbe essere determinato dalla necrosi casesosa di una adenopatia , colliquata in un bronco…ovvero da una caverna tbc aperta nello cavo pleurico…
I don´t know why the low participation, because the case is reasonably easy and most of you are right.
Although there is a surprise diagnosis on Friday!
Fibrosis apical izquierda asociado a retracción de la columna traqueal, asi como la presencia de espacio aéreo anómalo en relacion a caverna, se observa engrosamiento pleural difuso,con ligero derrame pleural y mayor luscencia en region paraahiliar derecha en relacion a atrapamiento aéreo.
There is a large well defined mass seen retrocardial in the azygoesophageal recess; Lymphadenopahy? Oesophageal pathology? Extramedullary haematopoiesis? Neurogenic tumours? other?
Esophagopleural fistula can not be excluded.
Back here after a long time 🙂
I see the air/fluid level on the left and the suspected mass in retrocardial projection, but can’t find the latter on the lateral.
My guess would be inflammatory pleural disease.. Now I’m curious 🙂
Be patient. Only a few hours left.
Mesothelioma?