Today we are presenting chest images of a 47-year-old woman with a cough. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
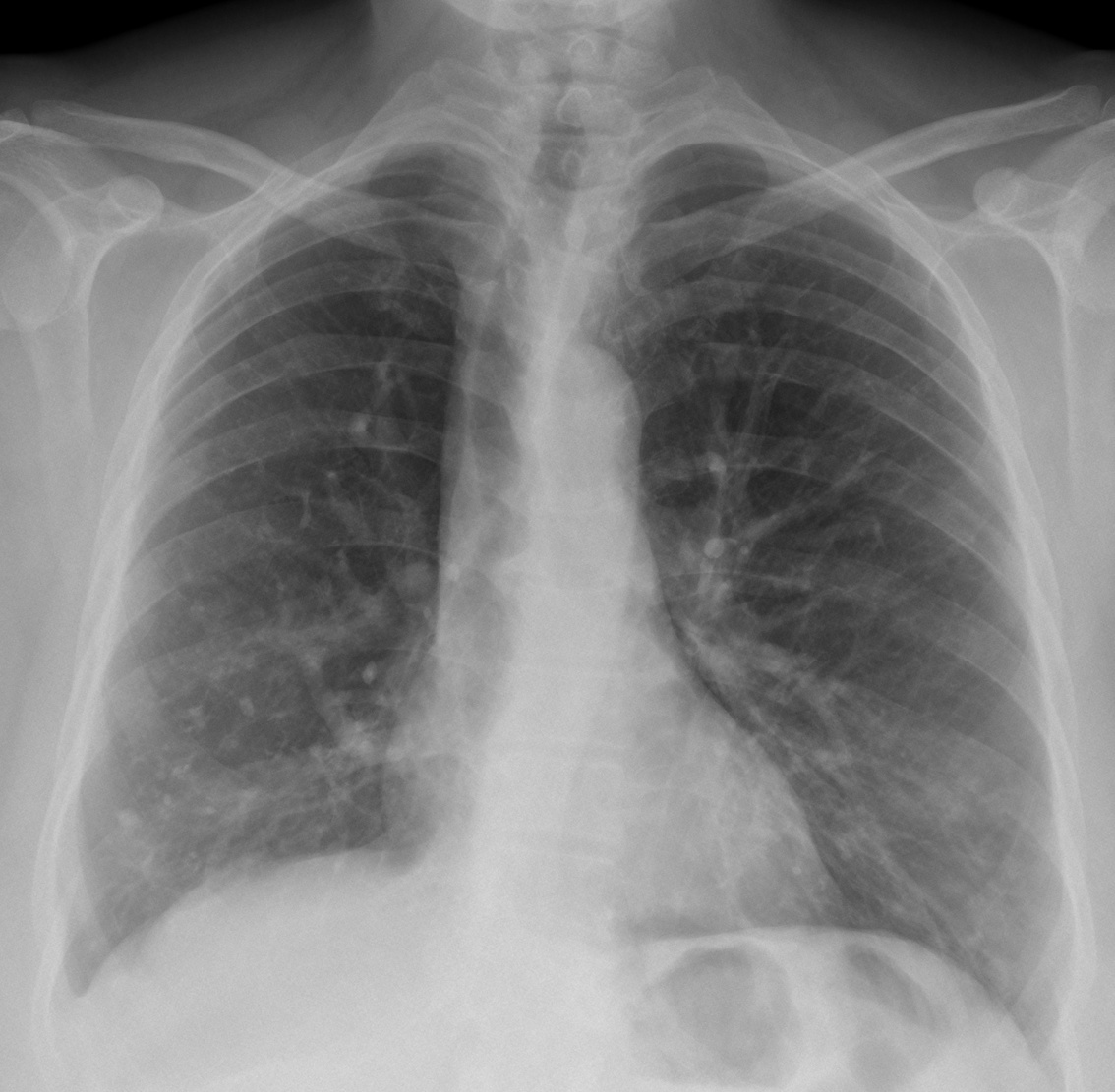
Findings: the PA radiograph shows an obvious downward displacement of the right hilum (A, red arrow). The intermediate bronchus has a vertical course (A, arrow), practically following the path of the trachea.
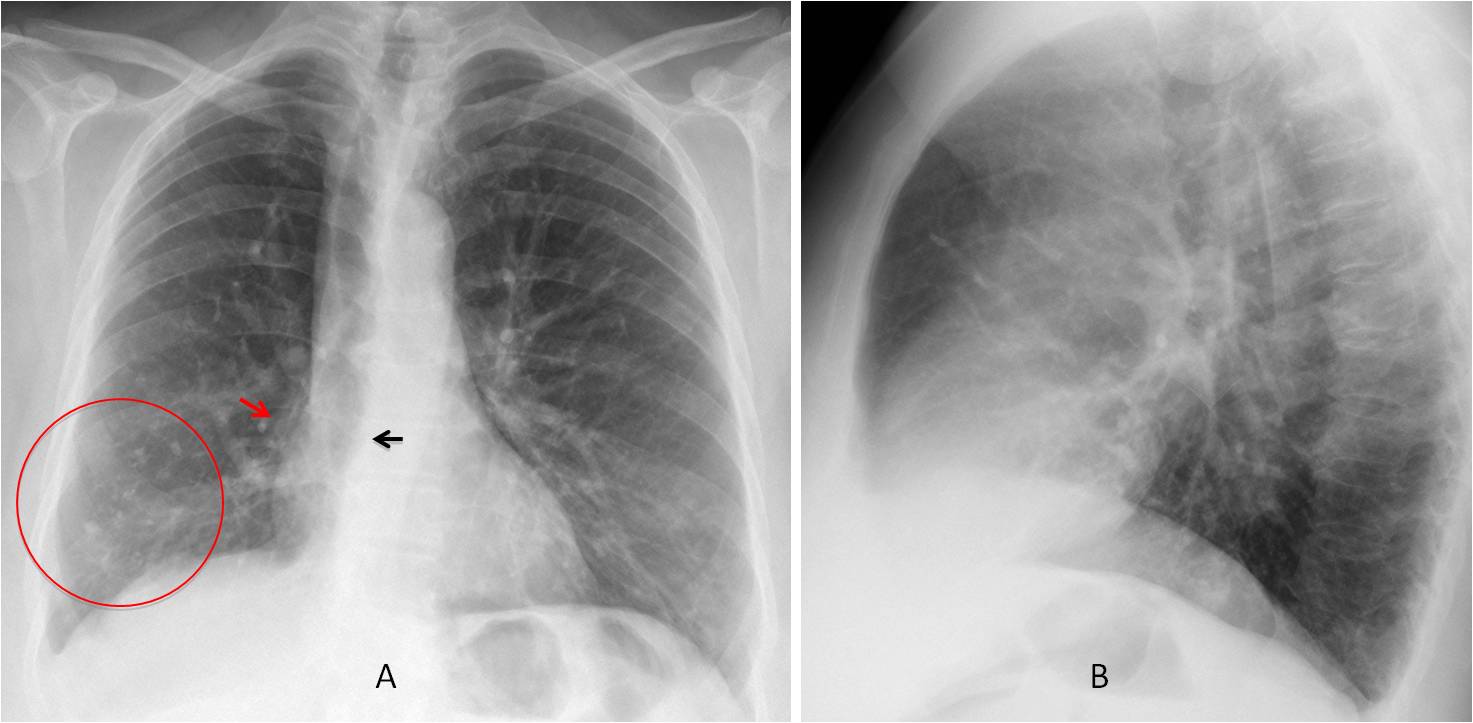
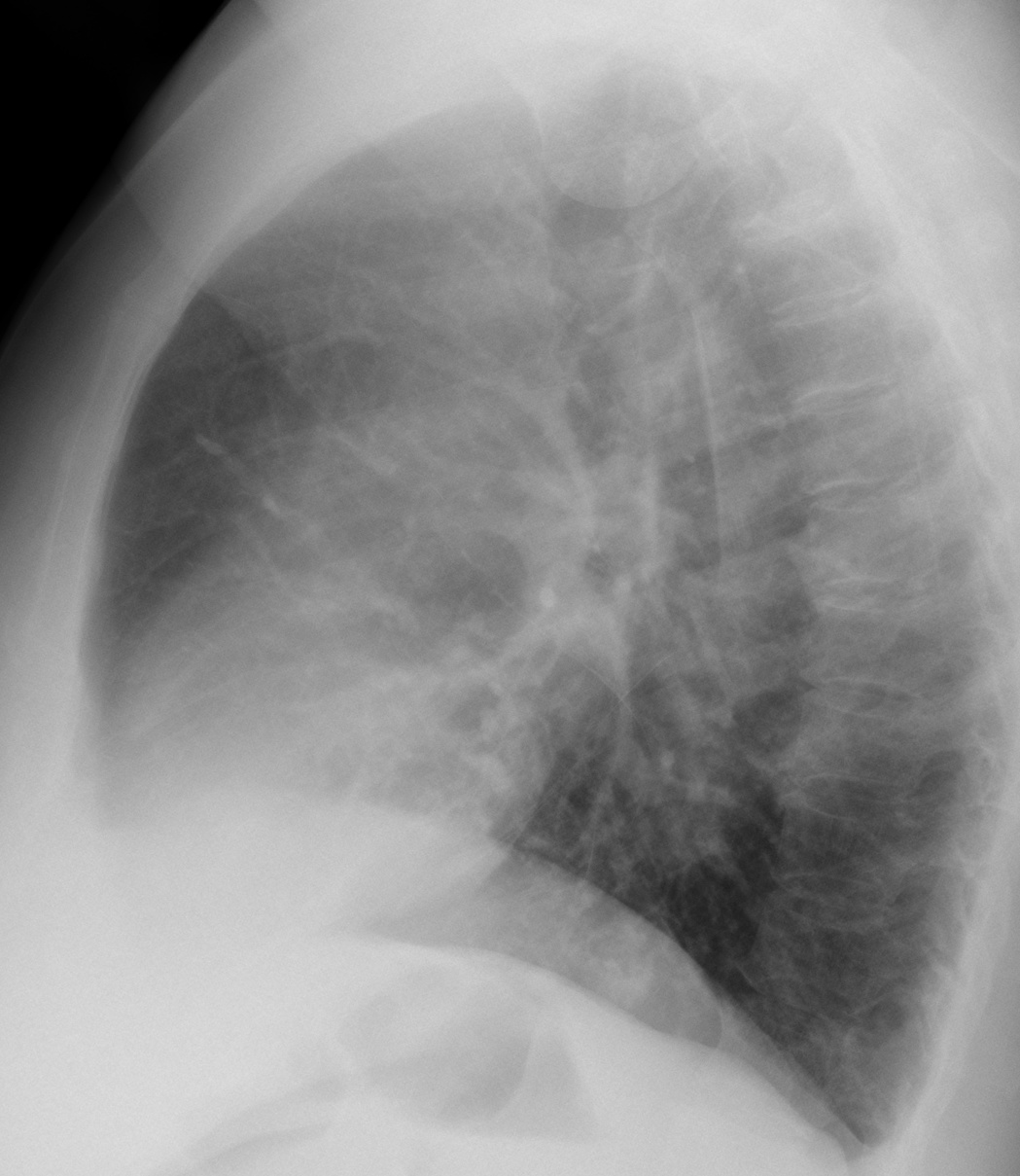
These findings are highly suggestive of marked RLL collapse (see Dr. Pepe’s Diploma Casebook case #79). There are calcified granulomas at the right lung base (A, circle). The lateral view does not offer any additional information.
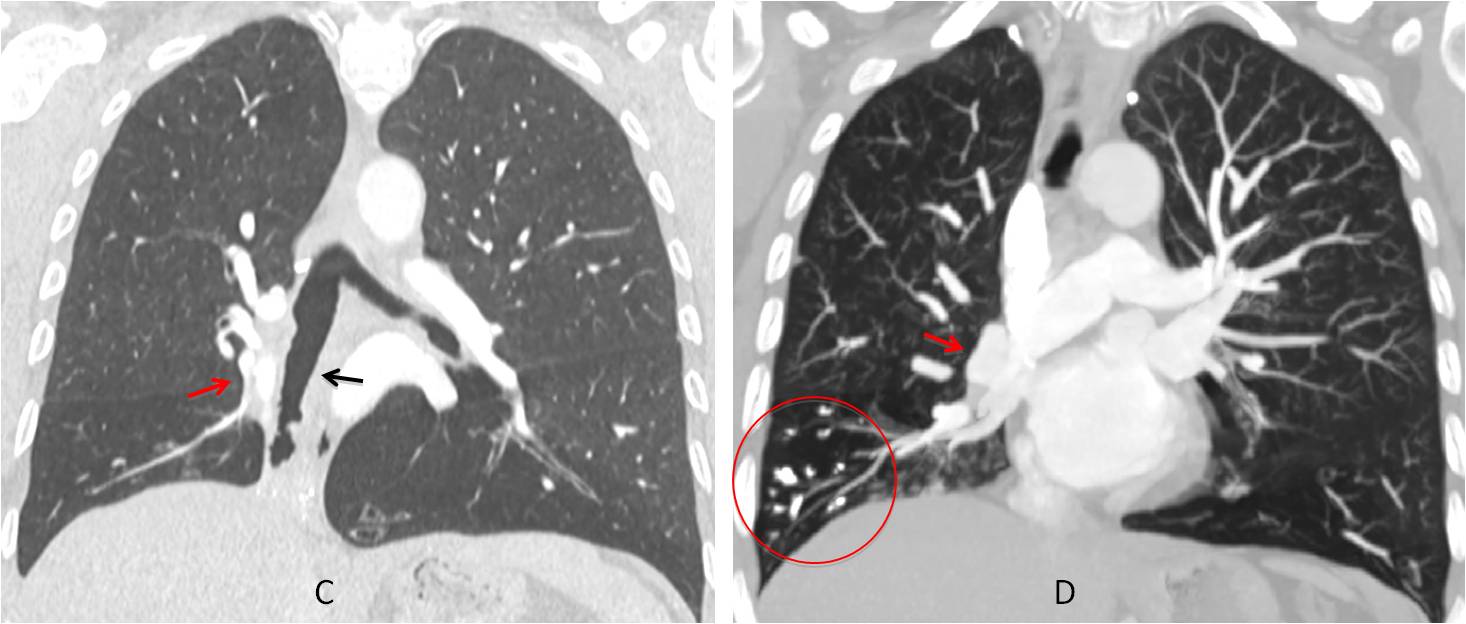
Coronal CT confirms the vertical path of the intermediate bronchus (C, arrow) and the downward displacement of the right hilum (C-D, red arrows). Calcified basal granulomas are seen (D, circle).
Axial and coronal CT show a small triangular shadow with coarse calcium (E-F, arrows), which represents a markedly collapsed RLL.
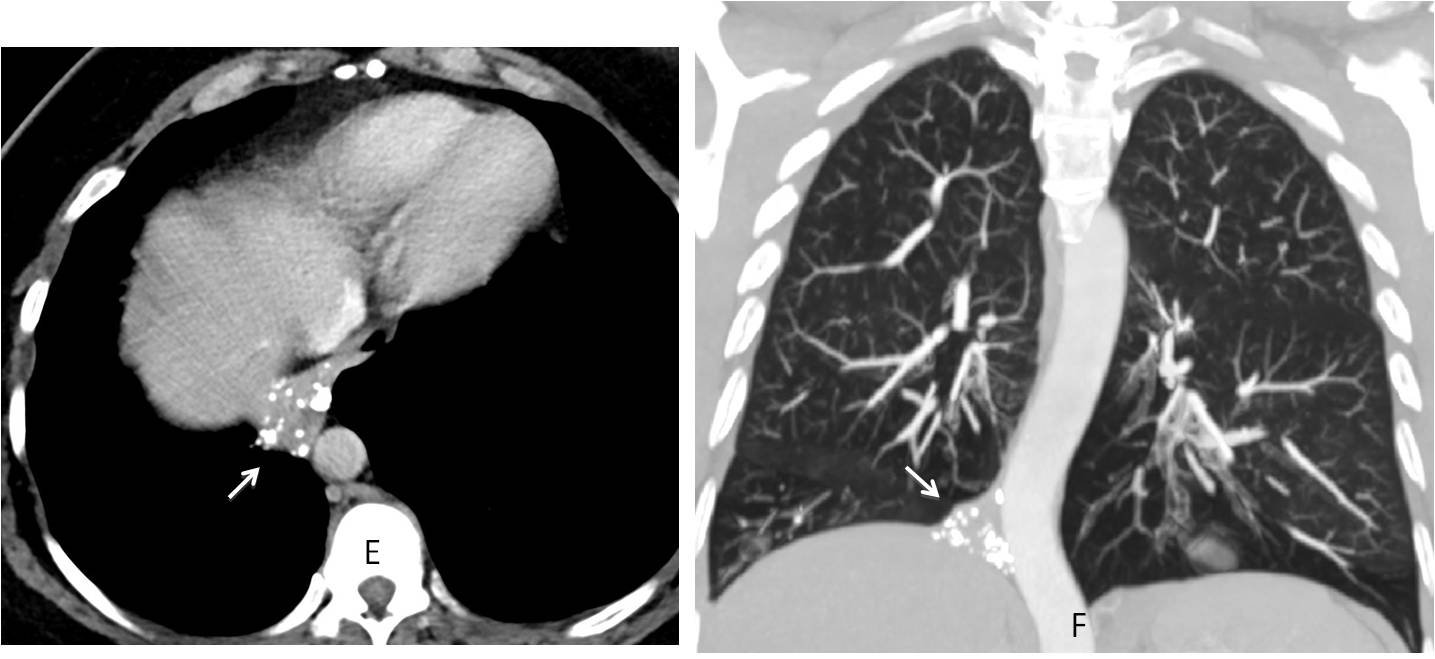
Final diagnosis: marked RLL collapse secondary to previous TB.
Teaching point: remember to look at the hila! A displaced hilum is an excellent sign to suspect lobar collapse.


pleural plaques
Where?
Abnormal vessel close to the right border of the heart. Anomalous pulmonary vein draining to right heart. Right to left shunt cause volume overloading of pulmonary arteries, that are very well visible and quite wide to the distal parts of the lungs. Although congenital , partialy anomalous pulmonary vein return could be diagnosed in adult.
inferior rib notching 6,7,8. coarctation of aorta.
few granulomas right lung field
Patient does not have systemic hypertension
Scimitar syndrome
pulmonal pletora?
As Sherlock Holmes said to Watson: “You see, but you don’t observe”
Tracheomalacia
Right sided tracheal shift– right upper love segmental collapse.
On frontal view: 1. Following airways there are trachea and carina deformation 2. Aortic contour deviation to the right in descending part of aorta 3. In the lungs: symmetrically intensified the shadows of pulmonary vessel system in hilar and prehilar zones – increased width of the vessels (increaseed/slowed blood supply/flight). In the right lung on the level of anterior parts of 5 – 7 ribs – diffuse single shadows, probably pleural plagues (ask for patients’ anamnesis morbi, working anamnesis); Blunt right costophrenic angle 4. There is no evidence of the surrounding soft tissue and the chest bone tissue pathology, but there is an S-like scoliosis deformation of thorasic spine – probably of II grade – which affects on the location of the mediastinum – there is not normal mediastinum contours, edges and shape; mentioned trachea deformation.
On lateral view: 1. Increased kyphosis 2. There is evidence of both increased left and right heart ventricles 3. It is noticed the “second” trachea behind the main radiograph trachea visualisation – it looks like tracheal trifurcation 4. There doubt about top of superior part – the additional horizontal wide shadow in the middle and inhomogeneous shadow of the first visible thorasic vertebrae – suspicion fracture (which could be denied because of no trauma and complains of back pain)
It could be scimitar syndrome (because of increaseed/slowed blood supply/flight, and the suppose of tracheal trifurcation (as an additional finding)), cough could be a symptom of recurrent pulmonary infection, but there is no visible evidence of small right lung and hemithorax, mediastinal shift to the right (dextroposition of the heart), indistinct right cardiac border, increased right lung opacity or precise shadow of vertically oriented curved tubular opacity (anomalous draining vein) in right inferior hemithorax coursing toward right cardiophrenic angle (it could be obscured by the heart in cases of pronounced cardiac dextroposition, but not in this case) or diminished right pulmonary vascularity.
It is recommended to persue CT angiography/Echocardiography to look for other associated congenital heart diseases in symptomatic patients
Wow!Nice discussion, although you missed some findings. See the answer tomorrow.
Maybe I miss the not normal right hila – maybe because of error of bronchial and vessels branching. And also I didn’t mentioned the more evident shadow of superior vena cava….Oh! I see! – The absence of bronchus lobaris superior dexter!
that is why there is a shift to the right of the superior part of mediastinum
….micronodulia alle basi,bilateralmente….lieve sbandamento a dx della colonna d’aria tracheale, con sottile ispessimento del profilo mediastinico, da questo lato….leggermente sollevata la cupola diaframmatica….la TAC chiarirà il tutto…..sospetto per k polmonare con atelettasia e metastasi….
Caro amico, no TAC needed. Dr Pepe made the diagnosis with the plain film 😉
Scimitar syndrome
Scattered nodular opacities in the right mid and lower zones.
Small right sided pleural effusion.
Trachea deviated to the right.
Ascending aorta not well visualised in PA view.
Descending aorta is shifted to the right.
The linear opacity lateral to the right heart border may be due to scimitar, but how does that explain right volume loss or right shifts?
A curvilinear vessel seen in the right lower zone adjacent to the right cardiac border. There is hypoplasia of the right lung with associated deviation of the trachea and mediastinum to the right.
The pulmonary vessels are prominent and rapidly taper, suggestive of pulmonary arterial hypertension. The heart is normal in size and contour.
Inferior notching is seen of the 6th-8th anterior ribs on the right.
Appearances are those of pulmonary venolobar syndrome with associated pulmonary arterial hypertension.
1. Left lung is small. There are abnormal tubular structures on the left hemithorax. Therefore pulmonary hypoplasia with anomalous venous retirn
2. The hila are abnormal in the lateral view: there is almost a donut but with a cleft and there could be a noch in the anterior portion of the trachea. Could it be a pulmonary ring?
3. There are calcified nodules in both lower zones: chicken pox pneumonia? Hemosiderosis related to valvular disease?
4. The anterior portion of the right hemidiphragm is blurred. Diaphragmatic duplication?
Corrigendum
1. Right lung is small. There are abnormal tubular structures on the left hemithorax. Therefore pulmonary hypoplasia with anomalous venous return?
2. The hila are abnormal in the lateral view: there is almost a donut but with a cleft and there could be a noch in the anterior portion of the trachea. Could it be a pulmonary ring?
3. There are calcified nodules in both lower zones: chicken pox pneumonia? Hemosiderosis related to valvular or associated cardiac disease?
4. The anterior portion of the right hemidiphragm is blurred. Diaphragmatic duplication?
exaggerated bronchovascular markings on both sides.
right pleural effusion .
dilated oesophagus with few basal reticular shadowing most likely systemic sclerosis