The case of this week is a pre-op radiograph for a knee prosthesis in a 57-year-old woman. What do you see?
Check the image below, leave your thoughts in the comments section and come back on Friday for the answer.
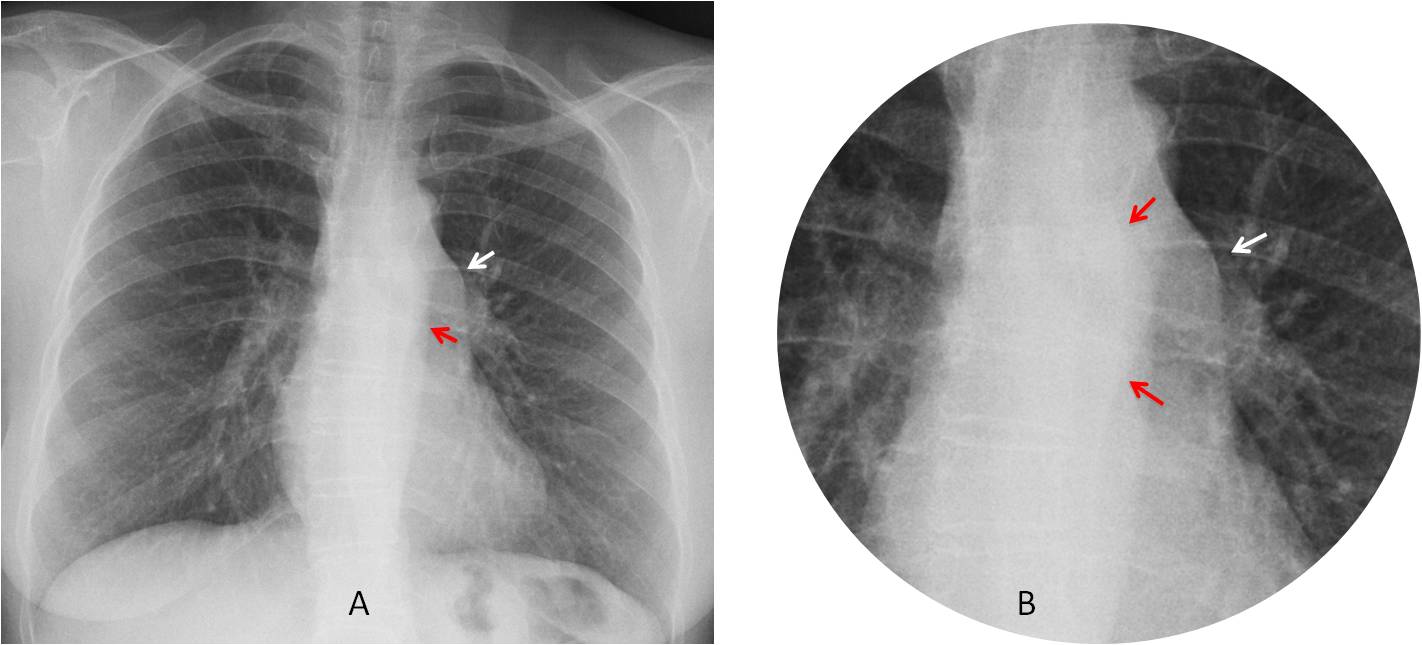
Findings: the PA chest radiograph shows a localised bulging of the left paraspinal line, better seen in the cone down view (A-B, red arrows). In addition, there is an obvious prominence (A-B, arrows) of the pulmonary artery arch (See
Dr. Pepe’s Diploma Caesbook case #52).
The location of abnormalities in both posterior and middle mediastinum suggests enlarged lymph nodes and I considered lymphoma a good possibility (and I was wrong).
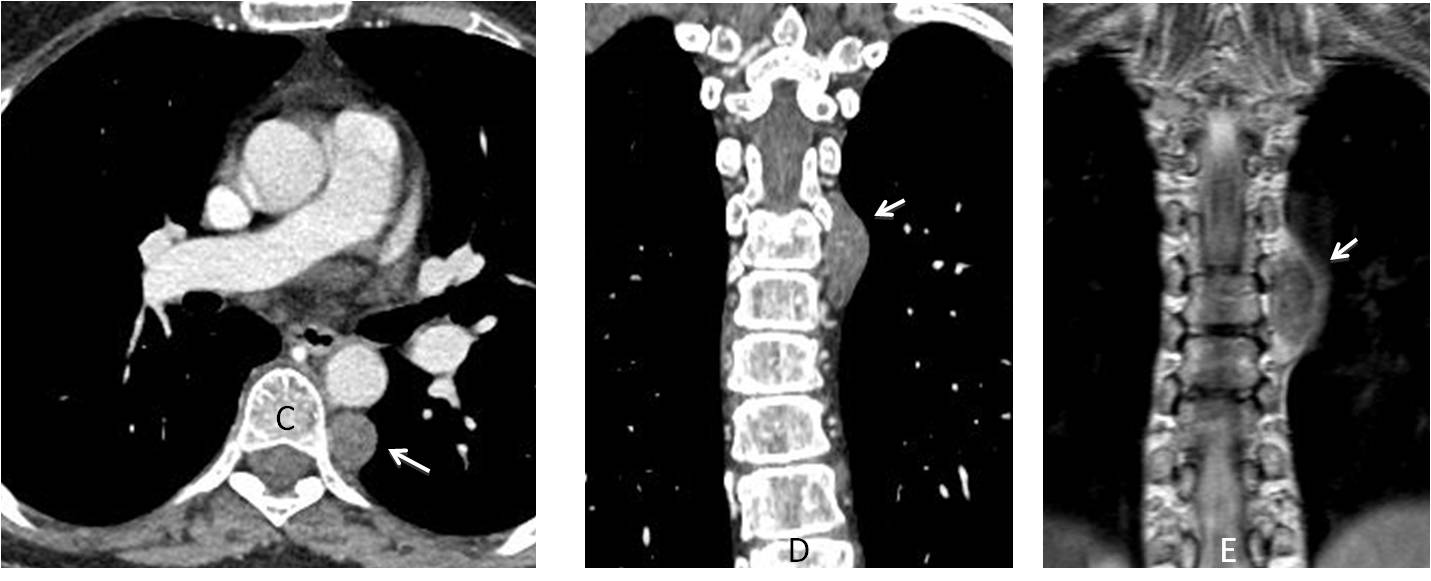
Enhanced CT and MRI confirm a solid posterior mediastinal mass, compatible with neurogenic tumour (C-E, arrows).
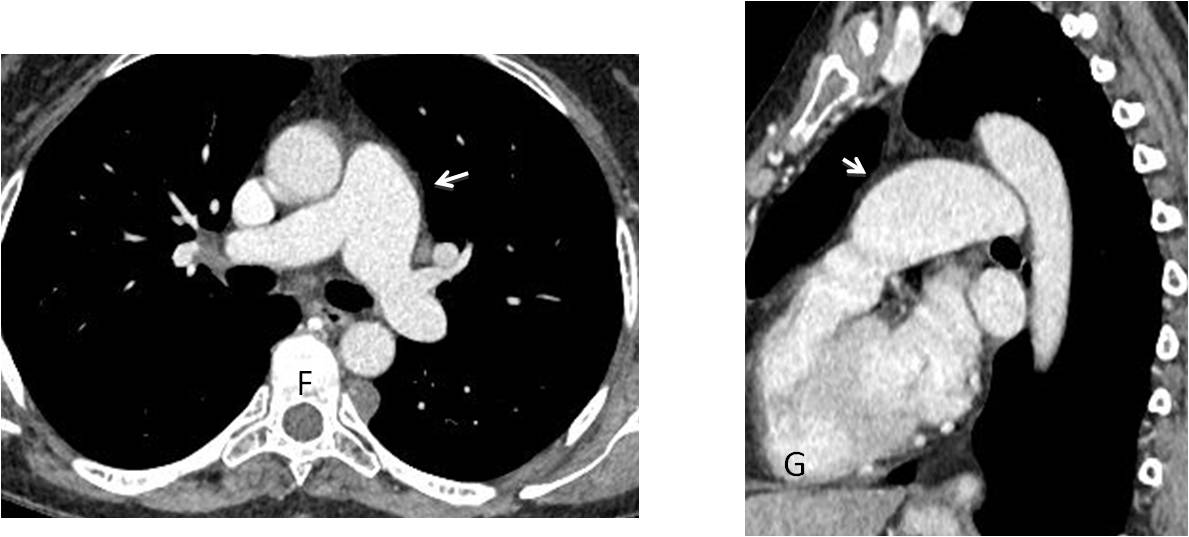
Enhanced axial and sagittal CT show a dilated main pulmonary artery (F-G, arrows). Further studies failed to demonstrate a gradient across the pulmonary valve.
Final diagnosis: unsuspected schwannoma and idiopathic dilatation of the pulmonary artery.
Congratulations to Diogo Pinheiro and M.A. Fahmy who teamed up to make the correct diagnosis
Teaching point: this is another case of satisfaction of search. Most of you saw only one abnormality, either the posterior mass or the prominent artery. I saw two, but still I did not fare any better!



Bulging left paraspinal line. Posterior mediastinal lesion. Ddx includes neurogenic tumor, extramedullary haematopoiesis, and vascular abnormality.
Loss of the cardiac waist in keeping with dilated pulmonary artery.
Minimal scoliotic list of the lower thoracic spine.
Clear lung fields.
Mmmm, I think there is an irregularity of the left hemi-diaphragm, may be sub phrenic cause, ? Gastric mass.
Yes, I agree as well with Diogo for the bulging of left para spinal line with a soft tissue, may be the cause of the slight scoliosis.
I agree with Diogo
Bulging noted at the aortopulmonary window with no associated vascular changes .. Enlarged LN is suspected for CT, no scilhouting of the descending aorta, middle mediastinal pathology
Agree with bulge in left paraspinal line.
No cardiomegaly, but cardiac apex uptilted – ?RV hypertrophy.
I go for a Posterior mediastinum paraspinal ganglioneuroma- Because of the shape, age and location.. Maybe we should look for Men 2b with tendency to marfanoid habitus associated with lower limb problems.
Extramedullary hematopoesis is less probable cause I dont think there are signs of splenomegaly which we usually could see in such case
…Diogo ….l’idea iniziale….Uil….la diagnosi finale…..
Not so fast, dear friend 🙂 Aren’t you overlooking something?
anterior mediastinal lesion
left hilar malignant mass
Left para spinal homogeneous opasity opposit D6 and D7. Right list of mid dorsal spine. No pulmonary lesion. Posterior mediastinal mass is considered