Muppet is so happy to have reached our 50th case, that he wants everybody to get the right answer. Here we have radiographs of a 52-year-old man with mild fever, blood-tinged sputum and left chest pain.
1. Carcinoma of the lung
2. Tuberculosis
3. Pulmonary embolism
4. None of the above
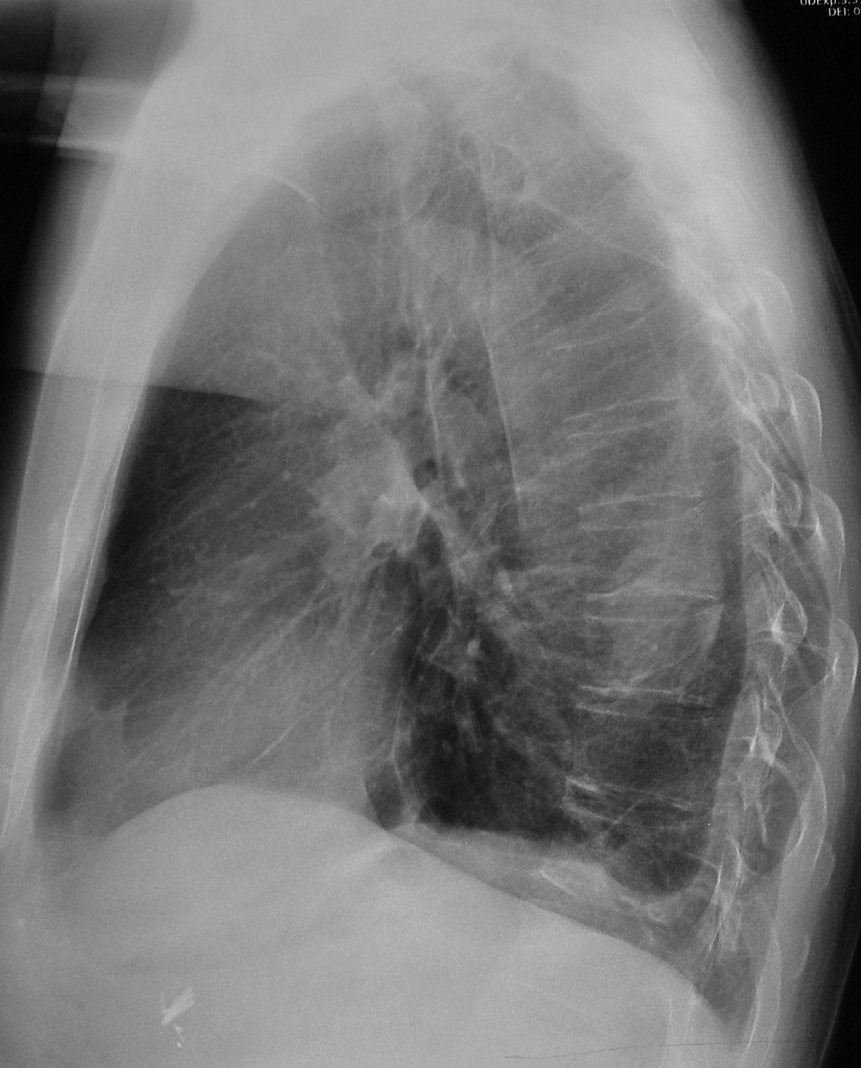
Findings: PA chest radiograph shows blunting of left costophrenic angle. There is medial displacement of left major fissure (arrows), indicating LLL volume loss. The left hilum is denser than the right one, suggesting a hilar mass. However, the left hilum is normal on the lateral view (
red arrow).
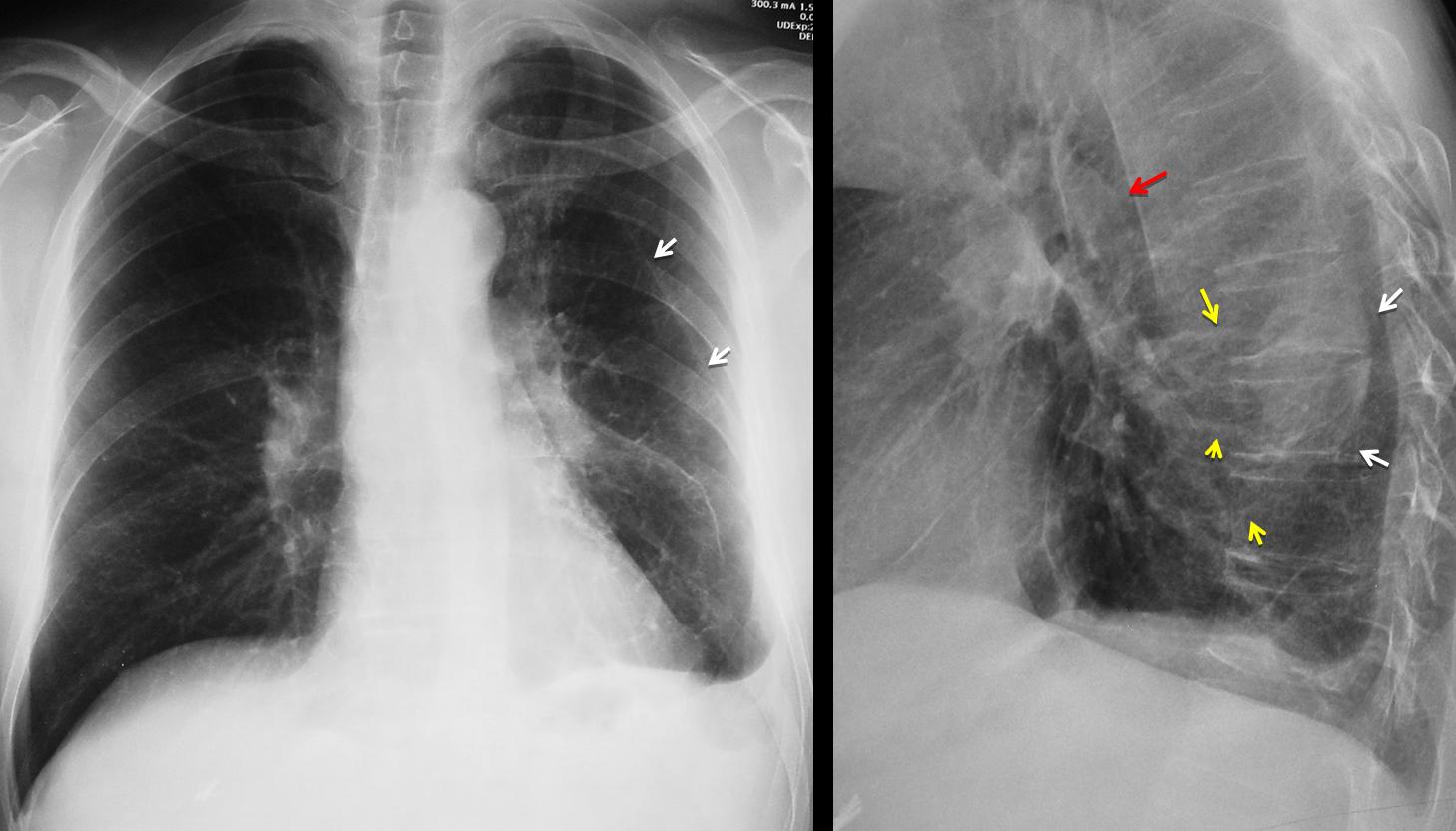
Its apparent increased density is due to a posterior ill-defined opacity (arrows), which is superimposed in the PA view and gives the false impression of increased hilar opacity. The clue to the diagnosis is identifying curving vessels (yellow arrows) leading to the posterior opacity, which should suggest rounded atelectasis. Axial and sagittal CT confirms the diagnosis by showing the atelectasis (A) the curving vessels and the thickened pleura.
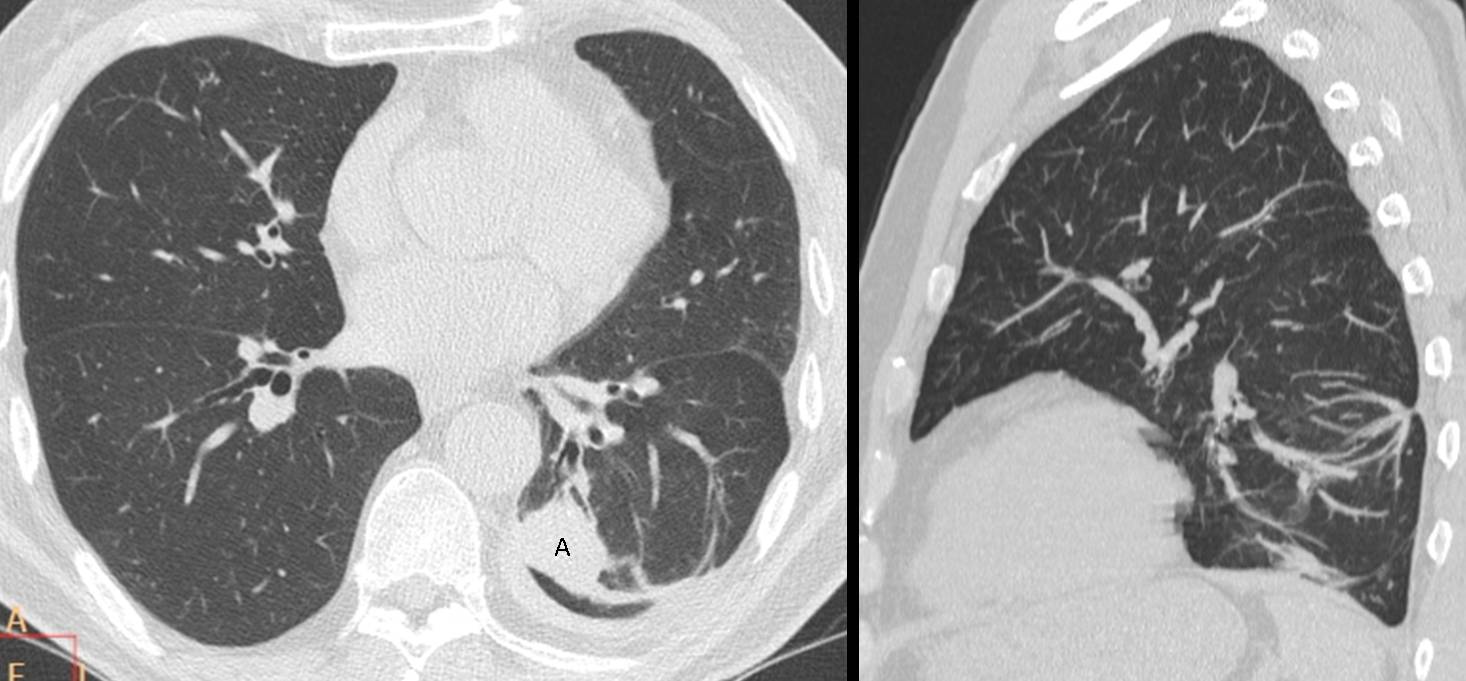
Final diagnosis: rounded atelectasis of LLL.
Congratulations to Dr. Strangelove, who was the first to mention the diagnosis (even though he called Muppet tricky).
This case was chosen as homage to Muppet’s first case, shown here on September 9, 2011. I quote:
“When we put together a peripheral rounded lesion, loss of volume and pleural thickening, rounded atelectasis immediately comes to mind and it is the correct diagnosis in this case. The typical findings of this condition are confirmed with CT.”
Teaching point: rounded atelectasis are not uncommon. Remember the four findings which suggest it: peripheral rounded opacity, loss of volume, curving vessels and pleural thickening.
Quoting again from case #1:
“Rounded atelectasis anchors in thickened pleura. Do not suggest the diagnosis if the pleura looks normal.”




carcinoma of lung
PE
I think the left hilum is enlarged in the left with pleural effusion in this side. Could be lymphnodes or a mass. TB is an option but the age and signals in radiography make carcinome more probable in my opinion.
Potrei mai lasciare solo il “galactico” ?: ecco la mia risposta “ragionata” sulla clinica e sulla semeiotica radiologica. Vi è un ilo sx addensato e “tronco” verso il basso, con oligoemia distrettuale. Vi è una opacità “ovoidale” posteriormente a livello di T7-_T8, adagiata sulla pleura, con versamento basale. Vi è il dolore all’emitorace sx, con febbricola( da necrosi), vi è tosse striata di sangue( proveniente dal focolaio infartuale). Se i D-Dimeri, sono elevati….tutto quadra per EP, con i segni di Westembark ed Hampton hump .
Bilaterarel apical rude calcifications.
Enlarged and dense bilateral hila. More obvius in the left where linear tracts and pseudonodular images extends towards the upper zone.
Linear atelectasis in lingula.
Left pleural effusion.
Dense seudonodular image centered at the level of D7-8 on the lateral. not clearly visible on the PA bcause it may be hidden behind the left hila where an abnormal countour could correspond to it.
Colecystectomy clips.
My hypothesis would be pulmonary neoplasm in the upper segment of the left inferior lobe with bilateral hilar adenopathies. Anyway, with TBC sequelae in both pleural apex and left uuper lobe.
Muppet disagrees with you about the dense left hilum
Muppet is tricky !
Round atelectasis
3
carcinoma of lungs
Round atelectasis is a good possibility. But there`s an round opacity in left hilum. TB associated with round atelectasis?
Muppet disagrees with you about the dense left hilum
linear opacities in the lul paramediastinal with luftsichelsign around aortic knob
ovoid opacity on the left not very dense – possibly pleural??
basal pleural effusion on the left
i would do a ct, its suspicious for carcinoma.
Congratulations.
I believe Muppet is not tricky this time. True answer is C.
The peripheral opacity in the LLL and the pleural effusion as well as the clinical data, strongly suggest pulmonary embolism. The left lung also contains some chronic lesions e.g.: parenchymal bands and UL fibrotic tracts, which could be due to remote tuberculosis.
Anyway, what happened yesterday to the FC Barcelona?
Sorry, description is fine, but final diagnosis is wrong. Muppet tricked you!
FC Barcelona had a bad day. It happens to the best of us. Even to Muppet.
Gli ANCA come sono?
As far a I know, ANCA are OK
looks to be tuberculosis…
I said Muppet is tricky because of the alarming symptoms. Well, may be there is here a lesson Muppet wants we to learn: we should trust radiological signs when they are clear and coherent. Nice case !
PD: Before posting the answer I googled “round atelectasis hemoptysis” and quickly I got several cases.
If symptoms were that important, clinicians would not need radiographs!