
Dear Friends,
Muppet is traveling abroad on a dangerous mission. If he doesn’t make it back, he hopes you will remember him fondly. For this reason he is showing a clear-cut case of pre-op radiographs in a 81-year-old patient with prostate carcinoma and right shoulder pain. Diagnosis?
1. Lung carcinoma
2. Fibrous tumour of pleura
3. Chest wall metastases
4. None of the above

Click here for the answer to case #53
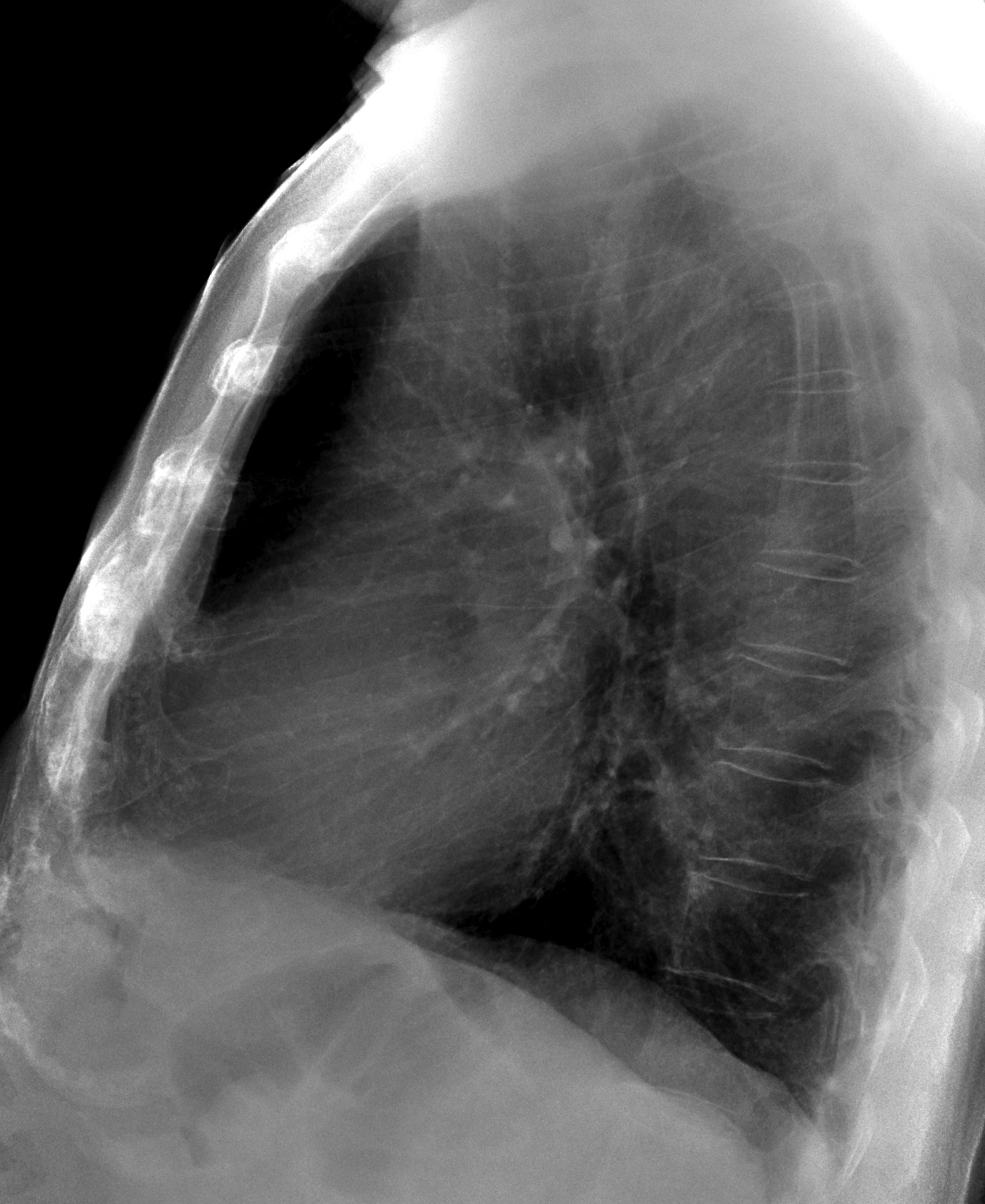
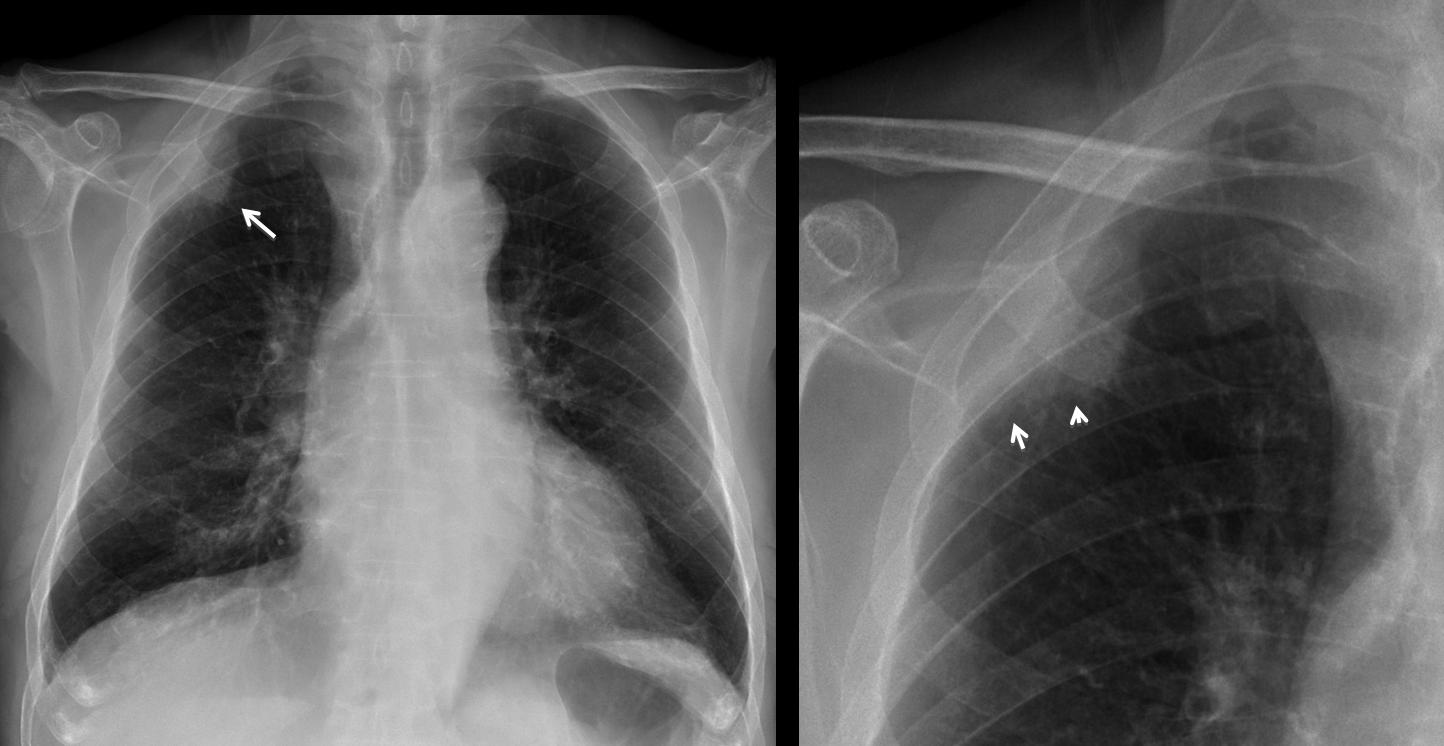
Findings: PA chest radiographs show a peripheral lesion (arrow), better seen in the cone down view. Although the upper limit has an obtuse angle, the border is not sharp and is clearly indistinct in the lower aspect (arrows). These findings are typical of a pulmonary process and exclude an extrapulmonary lesion (options 2 and 3).
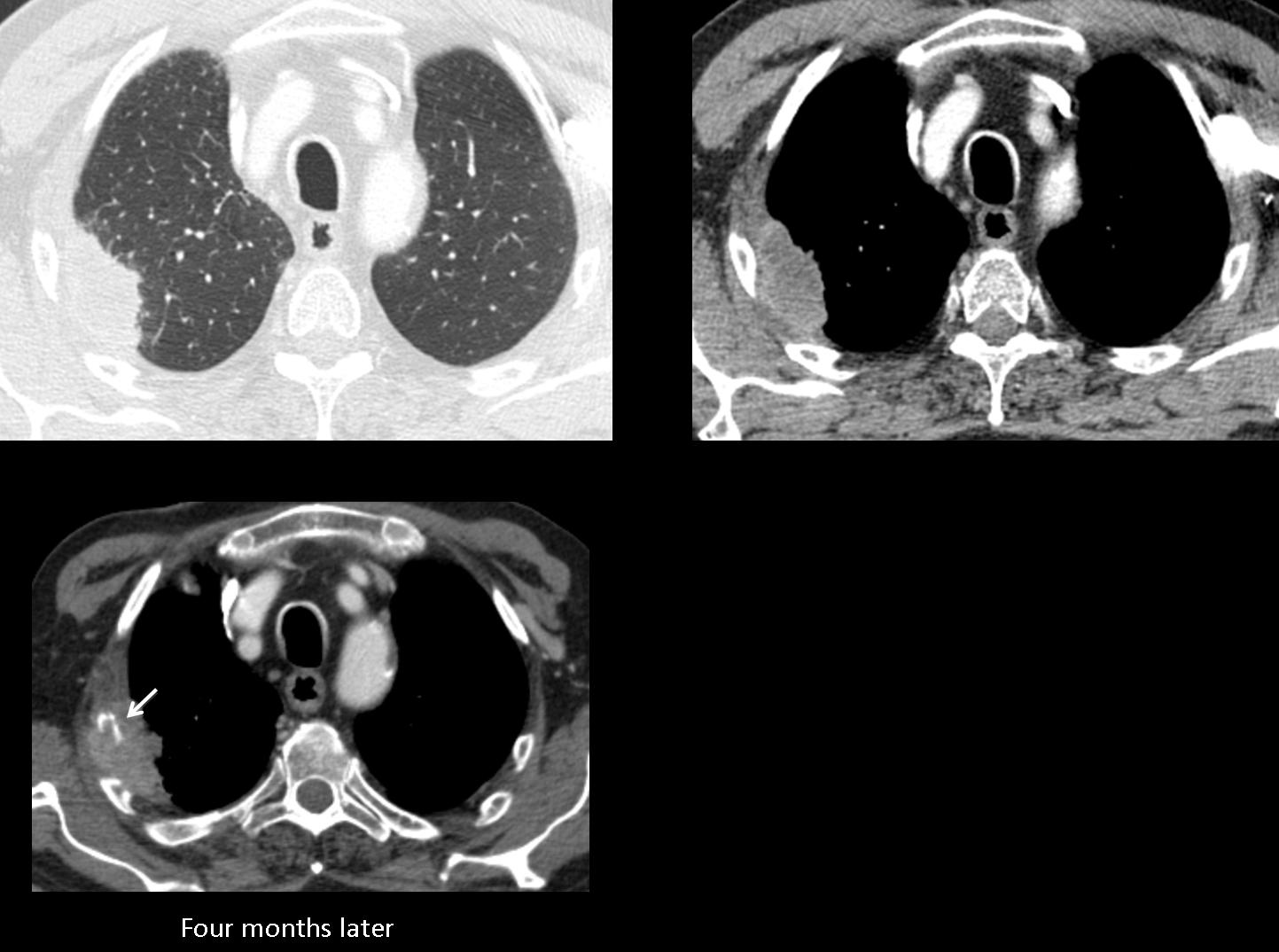
CT confirms the pulmonary location of the lesion and the fuzzy border.
Four months later there is obvious invasion on the underlying rib (arrow).
Final diagnosis: peripheral lung carcinoma
Teaching point: extrapulmonary lesions have obtuse angles at the borders and are sharply defined. If one of these characteristics is missing, we should suspect a peripheral pulmonary process (see discussion of case no. 1)


May the force be with you, Muppet!
We wish you to come back soon
There is a RUL mass also encroaching the chest wall, thoug ribs seem preserved
I think it could be a Pancoast tumor, so the right answer is 1.
Congratulations! You are right and the first!
The consolidation has acute angles in relation to the lung, making it most probably an extrapulmonary mass, besides the pleura appears thickened, I think it is a pleural tumor
Pleural mass that is not accompanied by signs on the wall aggressive torácica.Una good option pleural fibrous tumor.
I think it is a pleural tumor.
I think it is a pleural fibrous tumor..
I think it is a pleural fibrous tumor..Not extending to ribs…
Also the fibrous pleural tumor associated (by up to 20% of cases) hypertrophic osteoarthropathy.
However in this clinical setting can not completely rule out metastatic origin.
Ovunque tu sia, “galactico” ,buona domenica!La sede della formazione spazio-occuoante è extra-polmonare e non si associa a lisi costale; inoltre non vi è versamento pleurico, il che è indizio di patologia non maligna.Escluderei allora, il Cr polmonare, la metastasi pleurica,il mesotelioma maligno ed un linfoma della parete pleurica.Tale formazione circonda a manicotto l’apice polmonare, improntando e dislocando dolcemente medialmente la trachea. Le opzioni allora rimangono tra il T.fibroso solitario della pleura ed il lipoma. Chiaramente la TC fa la differenza.
Ovunque tu sia, “galactico” ,buona domenica!La sede della formazione spazio-occupante è extra-polmonare e non si associa a lisi costale; inoltre non vi è versamento pleurico, il che è indizio di patologia non maligna.Escluderei allora, il Cr polmonare, la metastasi pleurica,il mesotelioma maligno ed un linfoma della parete pleurica.Tale formazione circonda a manicotto l’apice polmonare, improntando e dislocando dolcemente medialmente la trachea. Le opzioni allora rimangono tra il T.fibroso solitario della pleura ed il lipoma. Chiaramente la TC fa la differenza.
Muppet surprised about the monotonous opinion of the majority. Basically, it is a matter of differentiating intra from extrapulmonary lesions.
Right. In my opinion it is a pulmonary lesion given that contact with the lung is irregular. There is also obvious pleural involvement and probably chest wall involvement (asymmetric thickening of muscular apical shadows outside de ribs). So, Pancoast tumor is the best option as Xose pointed out. But then, the whole case is confusing, because it is well known that lymphomas may present exactly this way, infiltrating several planes without rib destruction.
Yes, it could be any malignant lesion. The important consideration is that, with the described findings, you will be considering it intrapulmonary and therefore malignant.
OK. Extending the differential, may be even actinomycosis could produce this pattern.
Se la lesione è intrapolmonare, se è maligna, se il soggetto ha subito radioterapia,si può pensare ad un B-cell Linphoma del complesso BALT.
Thanks Muppet for these challenging cases.
Pleural tumors typically appear as well defined lesions with obtuse angle to the chest wall (Dynes Radiographics 1992). There is no rib destruction that could favor an extrapleural mass. Moreover, fibrous tumor are usually sharply marginated (Rosado Radiographics 2003). I would therefore consider subpleural adenocarcinoma as the main differential (Glaser Radiology 1985).
I believe you made a nice summary of findings. Answer tomorrow
I thinh this is a lung cancer in the upper right lobe, so a Pancoast tumor
Jose:
The radiology residents and house staff enjoy these cases. When I present them, I mention the source and also show a picture of you and Muppet. However, I am embarrassed that I do not know in what city and institution you practice. If you can give me that information, I would like to pass it on.
Many thanks,
Herb
Glad to be of help. Muppet shy, answering in the prívate circuit