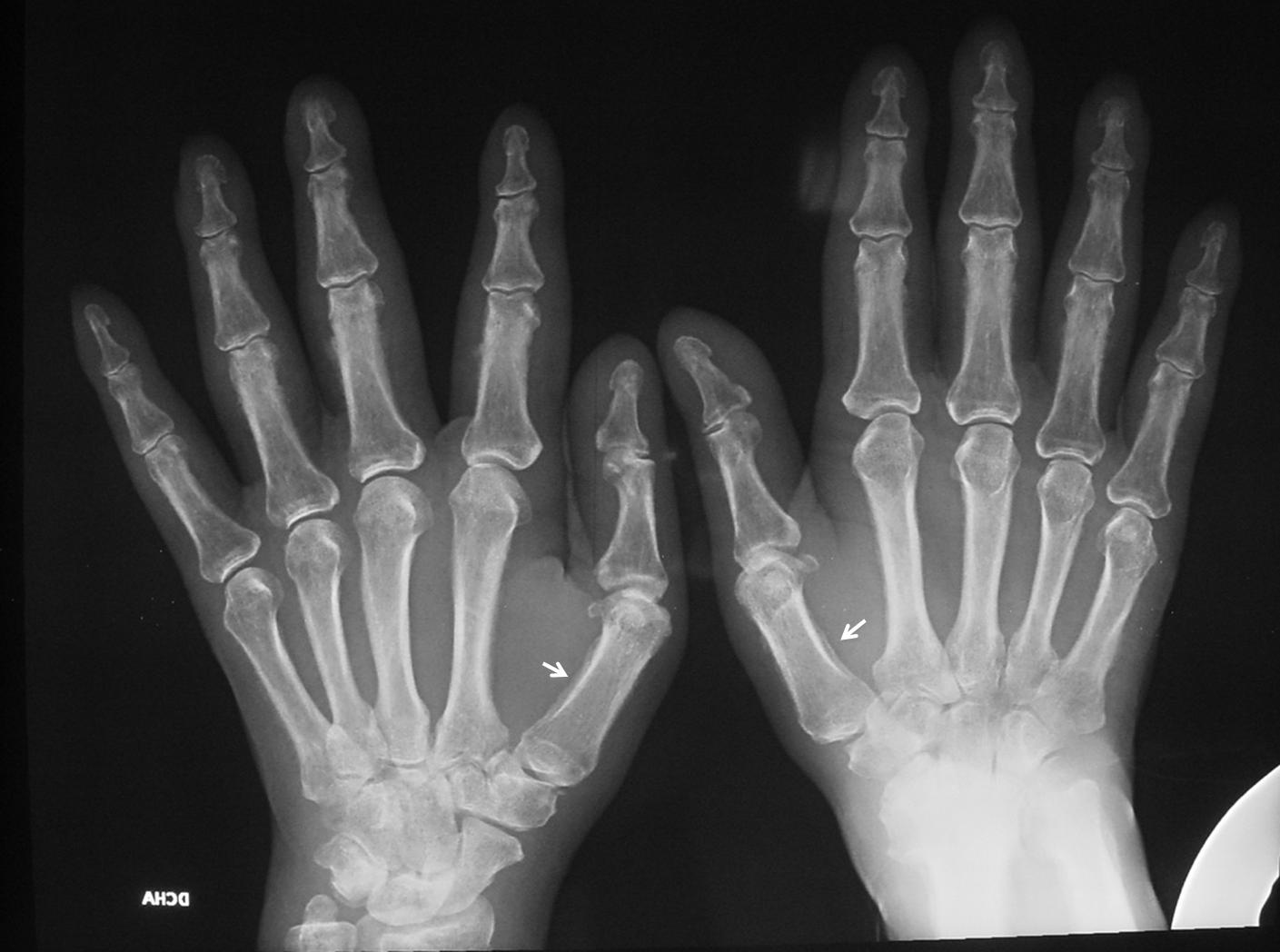
Muppet is running out of chest cases and wishes to show a bone case instead. Presenting an AP radiograph of both hands of a 59-year-old male with pain in the joints.
1. Rheumatoid arthritis
2. Psoriatic arthritis
3. Hyperparathyroidism
4. None of the above
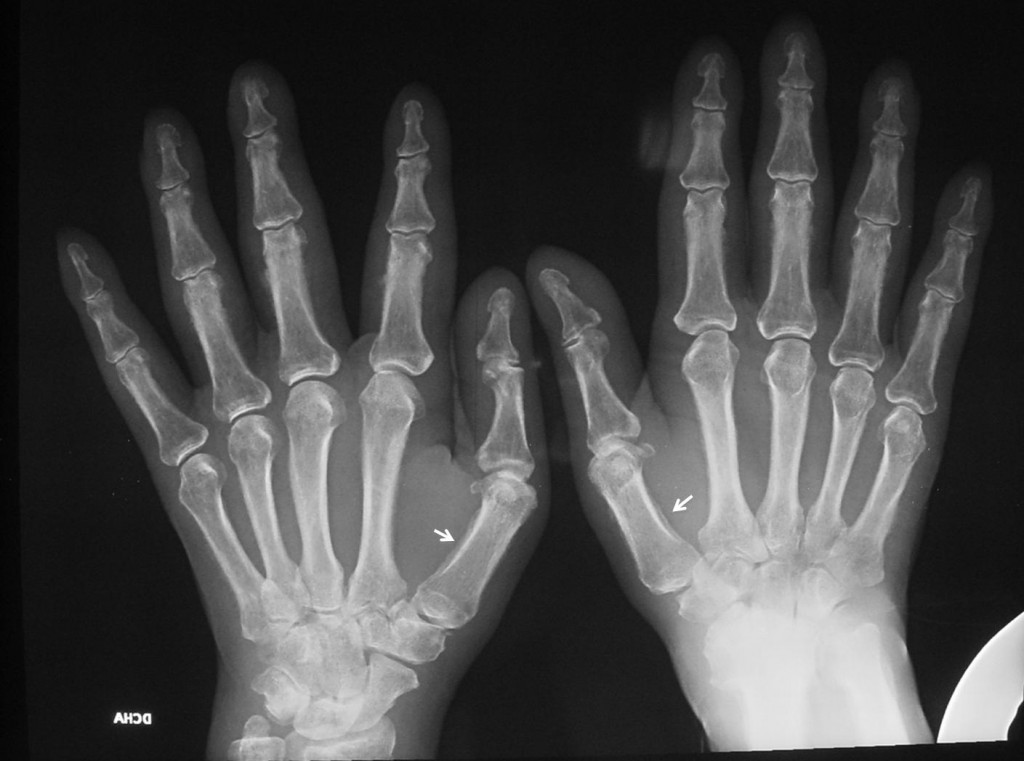
Fig. 1
Findings: the AP radiograph of both hands shows periostitis in the proximal phalanges, more obviously in the first metacarpals (arrows), and better seen in the cone down view.

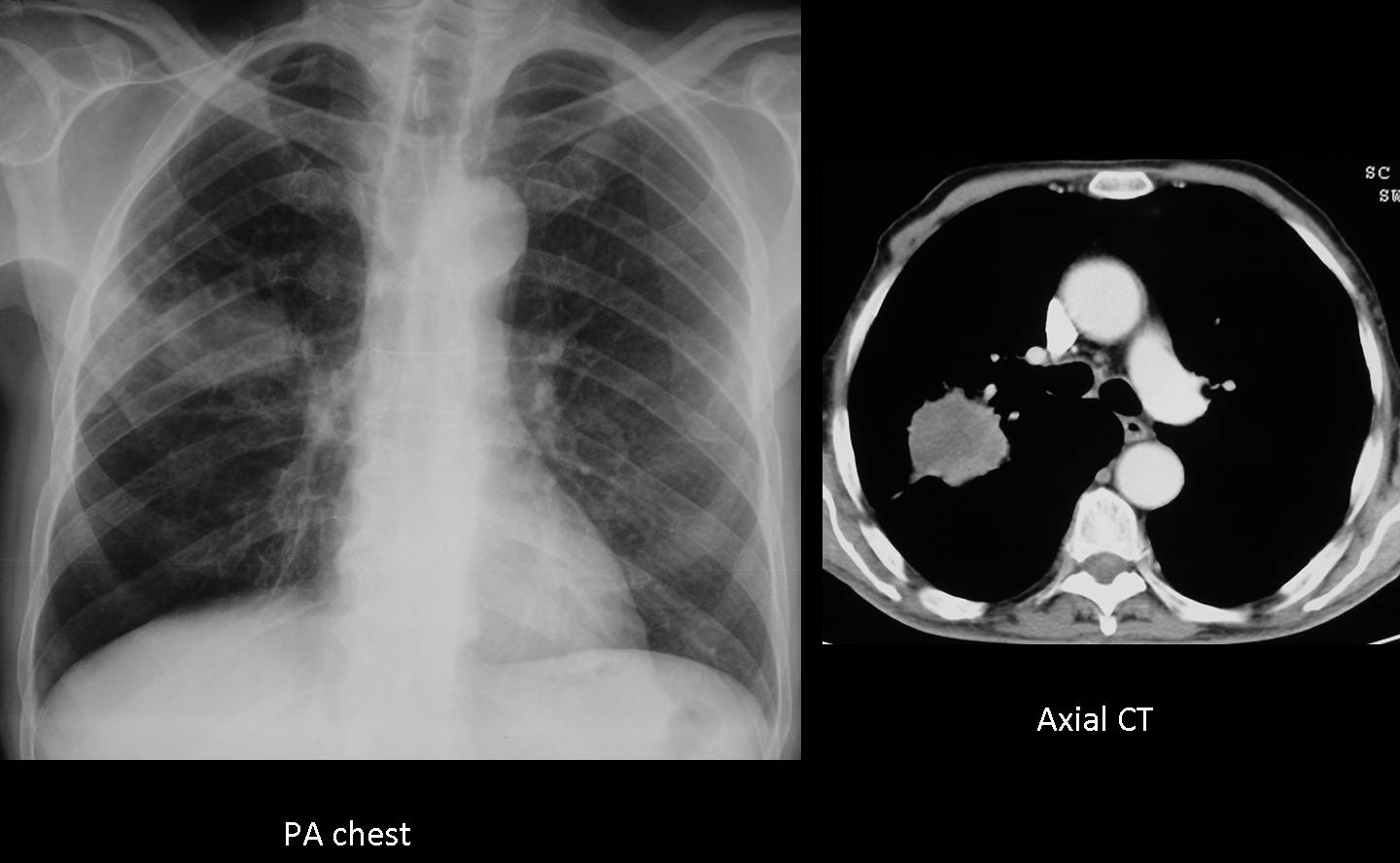
Fig. 2
There is also extensive periostitis in the bones of the forearm (arrows). There are not clear signs of arthritis.
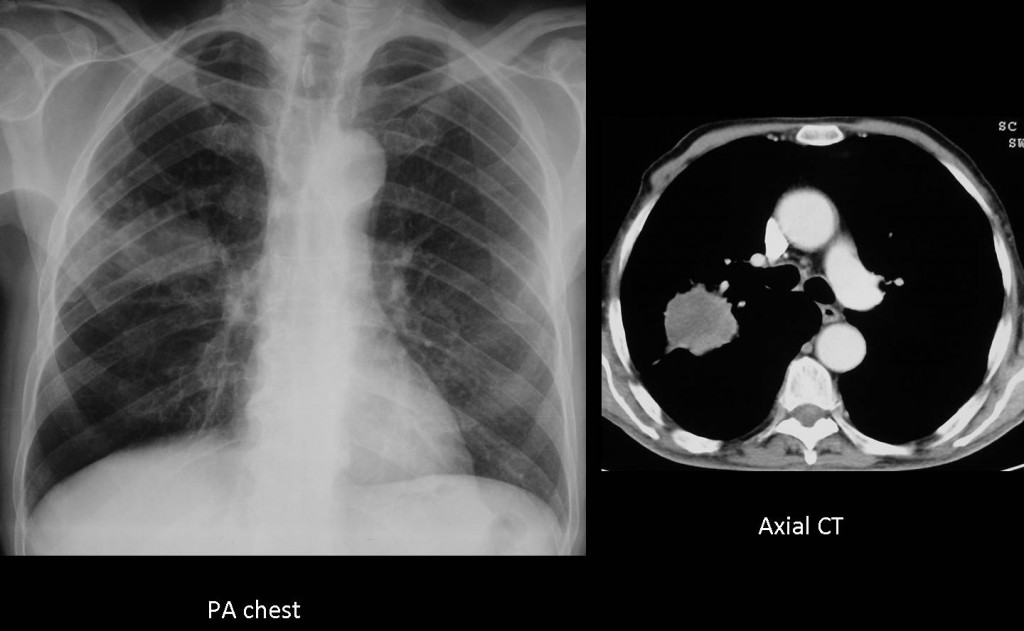
Fig. 3
Differential diagnosis includes disease with widespread periostitis (pachydermoperiostosis, thyroid achropachy, vitamin A intoxication, etc.). In an adult, hypertrophic pulmonary osteoarthropathy should be considered and a chest radiograph taken. In this patient, chest film showed a nodular opacity in the right lung, confirmed with CT.
Final diagnosis: hypertrophic pulmonary osteoarthropathy secondary to carcinoma of the lung.
Congratulations to Drs. Yp and Marcolino who made back-to-back diagnosis in an interval of two hours.
Teaching point: sometimes the initial symptoms of a lung carcinoma may be extra-thoracic (bone or brain metastases, hypertrophic osteoarthropathy) and it is important to know them to suspect the correct diagnosis.
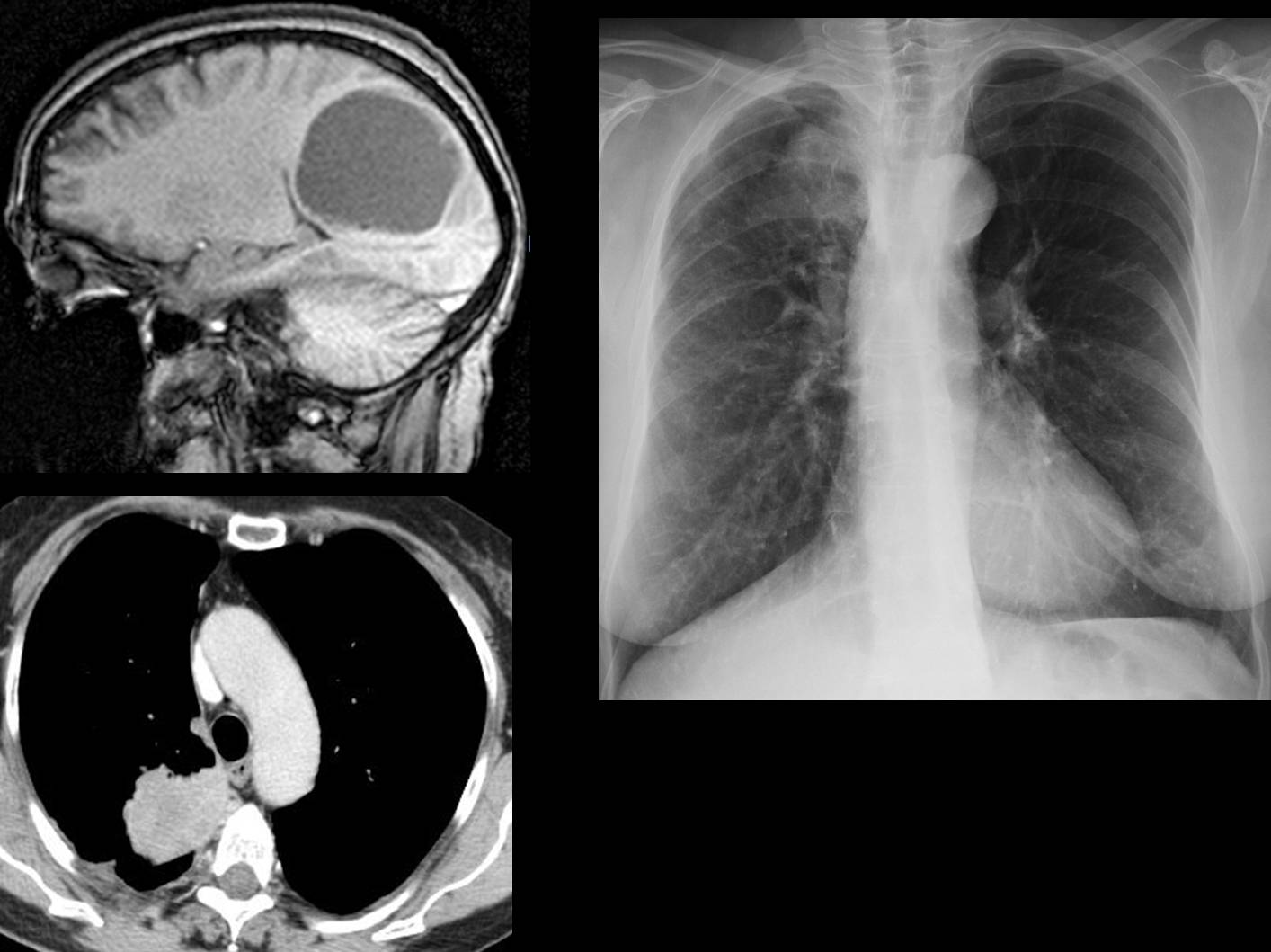
Below is a recent case (22 March), erroneously diagnosed as brain tumour, in which the primary lung tumour was discovered in the pre-op chest film.
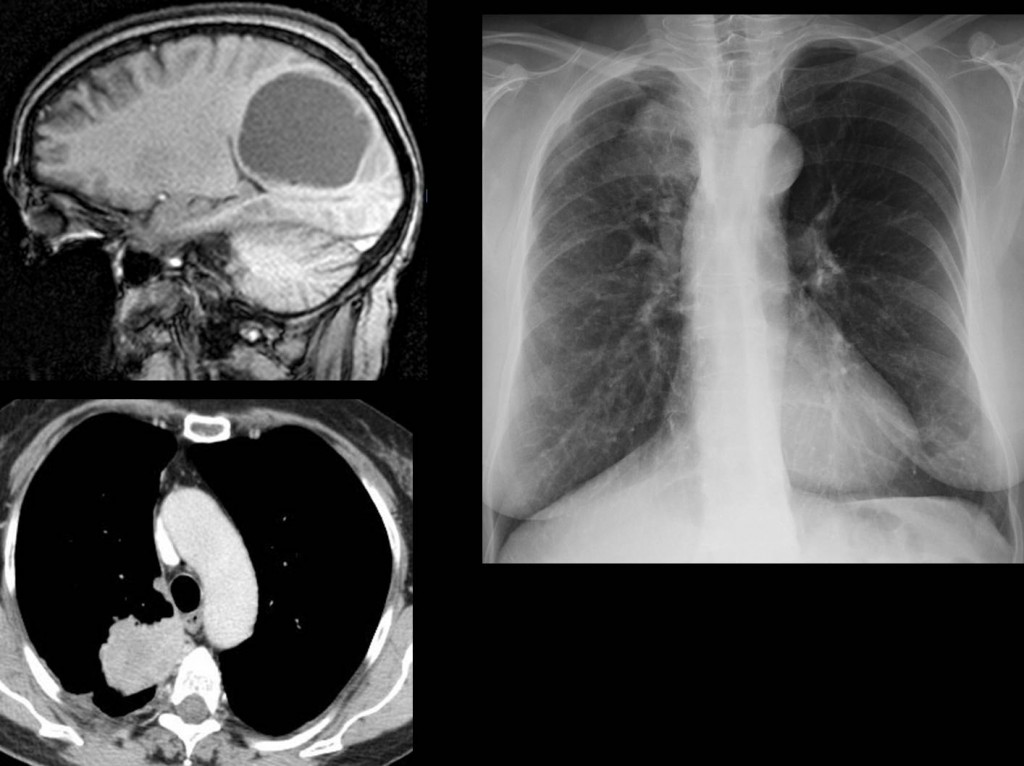
Fig. 4




the subperiosteal resorptions are quite suspicious for hyperparathyreoidism, so i go with answer 3.
4. In hyperparathyroidism subperiosteal bone resorption is identified along the medial sides of the middle phalanges.
joint spaces are preserved in distal joints..can’t be arthropathy..
it may be secondary hyper Hyperparathyroidism…sub periosteal resorption is pathognomonic for HPT , left wrist is almost destroyed with extensive sclerosis(like neuropathic joint).
Changes in left wrist are due to faulty positioning. It occurs whn both hands are radiographed together and the patient bends the wrist to be more comfortable.
Hypertrophic osteoarthropathy
Early psoriatic arthritis.
Alternatively hypertrophic (pulmonary?) osteorathropathy.
psoriatic arthritis is less likely no DIP involvement .. no obvious periosteal reaction. No brown tumours or diffue osteopenia or chondrocalcinosis.
Carpal bone erosions and sclerosis with juxtaaricular osteopenia favour rheumatoid arthritis.. but no marginal erosions and male patient put the diagnosis in quesion.. Anyhow I would go with 1. rheumaotid arthritis or 2. none of the above
– Clubbing fingers.
– Joint pain.
– Periosteal reaction of tubular bones, sometime linear e regular, without underlying osseous abnormality.
– Periosteal reaction involving the diaphysis of a long bone (distal ulna).
These clues suggest hypertrophic pulmonary osteoarthropathy.
Muppet needs to rule out lung cancer;)
thyroid acropachy
Hypertrophic osteoarthropathy
Hypervitaminosis A
Pachydermoperiostitis
I would consider hyperparathyroidism,(answer 3).
I would consider hyperparathyroidism,(answer 3). Blood analysis would follow…
none of the above
Any ideas?
There is soft tissue swelling in fingers in both hands simetrical,that means inflammation.it could a seronegative arthitis but i now the sausage-digit sign in Psoriatic arthritis is in one digit. it could be periosteal reaction in Psoriatic arthritis but no simetrical.Gout there is not because deposit of crystals is near the joins…
Hyperparathyroidism no way.
It looks like thyroid acropachy but thyroid acropachy is painless.i dont know…..
I agree with you about excluding hyperparathyroidism. It does not have subperiosteal resorption, which is the hallmark of the disease. But there is other condition (already mentioned) with widespread periostitis.
Profesor Caceres did you mean Hypertrophic osteoarthropathy? it’s often in the hands?.Hypertrophic osteoarthropathy produce pain but i thing in the long bones.
Hypertrophic osteoarthropathy occurs in the hands. I don´t know how often (will ask Muppet), but I have seen it many times.
Thank you profesor for your beautiful case.
i think Muppet is gonna be angry with me if you ask for..:)have a nice weekend
maybe is non carpal bone erosions…we dont have the prof.view to prove it if there is deposition disease.or CPPD or something else?
thyroid acropachy
Il pattern osseo non è di tipo erosivo iuxta-articolare: no AR.Il pattern osseo non è di tipo riassorbitivo( tunnelizzazione corticale) in sede metadiafisaria: non IPerparatiroidismo. Anche l’artrite psoriasica è di tipo distruttiva e , di solito mono-articolare. La risopota è la 4: quello che mi soprende è la “tumefazione ” della parti molli della dita, il che potrebbe indicare una entesopatia(ECD-Doppler), siero-negativa.NB nel caso precedente ho mancato in pieno il bersaglio: scusa!Cosa dice Alice?
The last case was really mean 😉 i was absolutely convinced of the bone metastases!!
Both hands Ap view.
Bilateral symmetrical soffit tissue swelling is seen at 2′,3′,,’4 digits.
Bilatera linear l periosteal reaction along the ulnar side of 1st metacarpal bones .
Bilateral Symmetrical spotty fluffy periosteal reaction at mid shaft of 2’3’4 proximal phalanges .
Erosion at right trapezium and left pisiform
Normal DIP and PIP joints .
Normal carpal joints .
Provisional diagnosis is seronegative arthropathy as psoriasis and Rieter,syndrome .
Hand involvement is in favor of psoriatic arthritis .
Visible periosteal reaction excludes rheumatoid arthritis .
No visible sub periosteal bone resorption , so hyperparathyroidism is less likely .
Diagnosis : psoriatic arthritis.
rheumatoid arthritis
S. di Reiter: la triade classica include l’artropatia , con dita a salsiciotto e periostosi.Risposta n 4.
No. 4 Hypertrophic osteoarthropathy as mentioned above (first by Yp)