This is just the first of many weekly cases I’m going to show here on the ESR blog, to help you prepare for the European Diploma in Radiology. They are all typical of what you might expect to find in the exam and I will guide you through each one and remind you of the key points to consider.
To start off, I’m going to follow in the footsteps of my good friend Jose Caceres (although I will be more compassionate), and show you a chest case. If you have any comments or questions, please leave them in the comments section under this post. The answer will be posted on Thursday.
1. Myeloma/metastases
2. Fibrous tumour of pleura
3. Extrapleural fat
4. All of the above
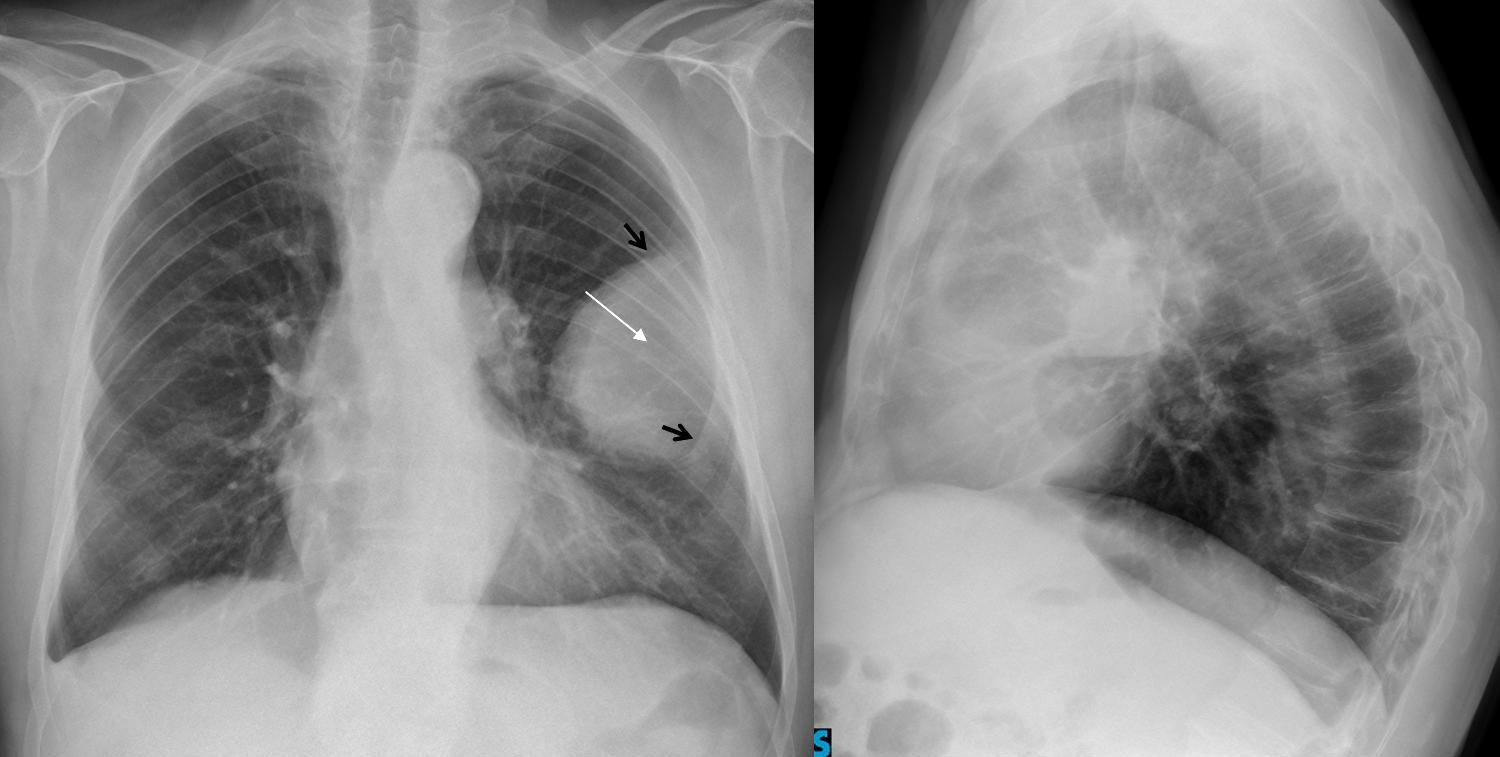
Findings:
There is an extrapulmonary mass in the left hemithorax with destruction of the anterior aspect of the 4th rib, which is not visible (white arrow), whereas the anterior 3rd and 5th ribs are easily visible (black arrows).
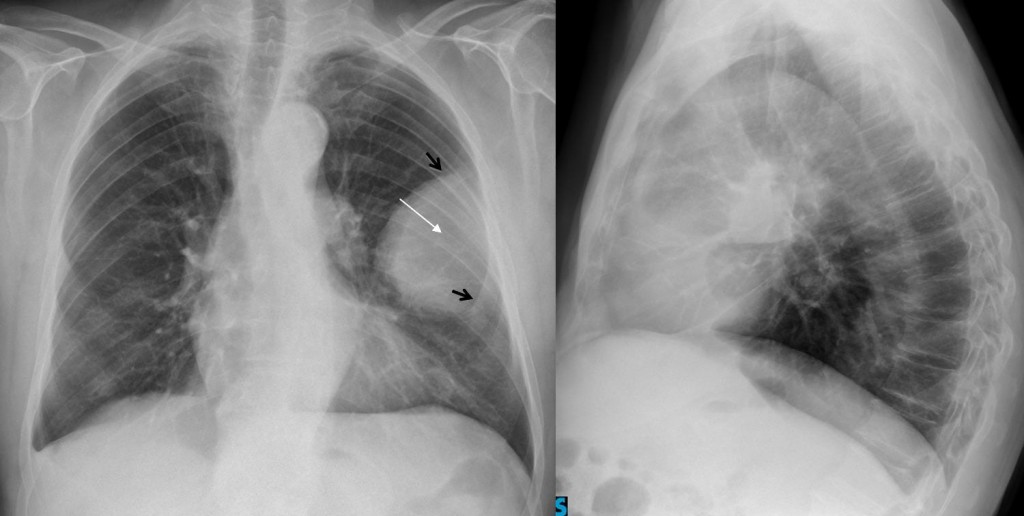
Fig 2
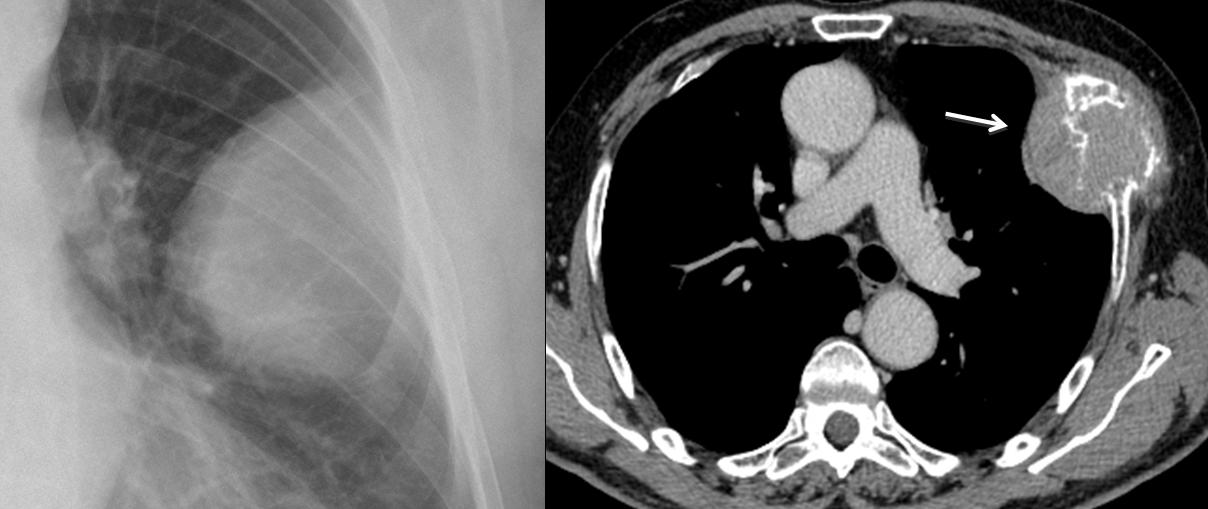
Given that the rib is destroyed, the most likely diagnosis is a malignant costal lesion, either a metastasis or myeloma, neither of which can be distinguished by imaging. CT confirms the rib destruction and the extrapulmonary mass (arrow).
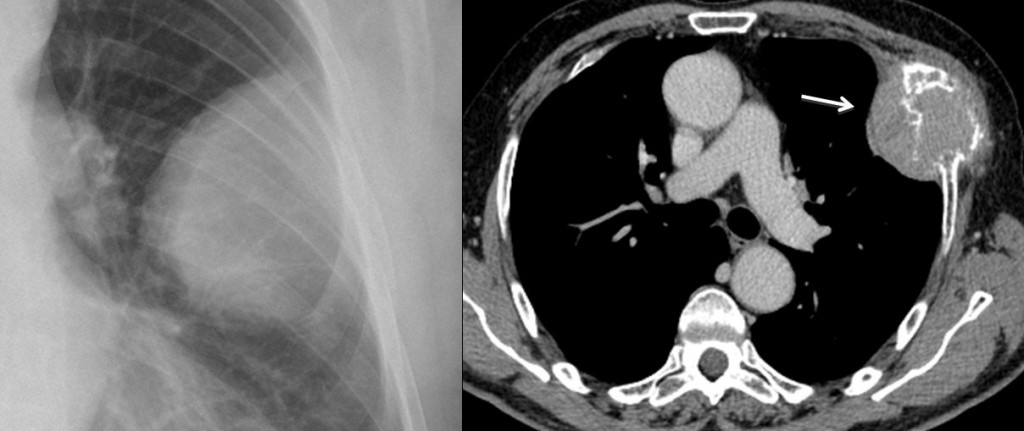
Fig 3
Final diagnosis: metastasis from hepatocarcinoma.
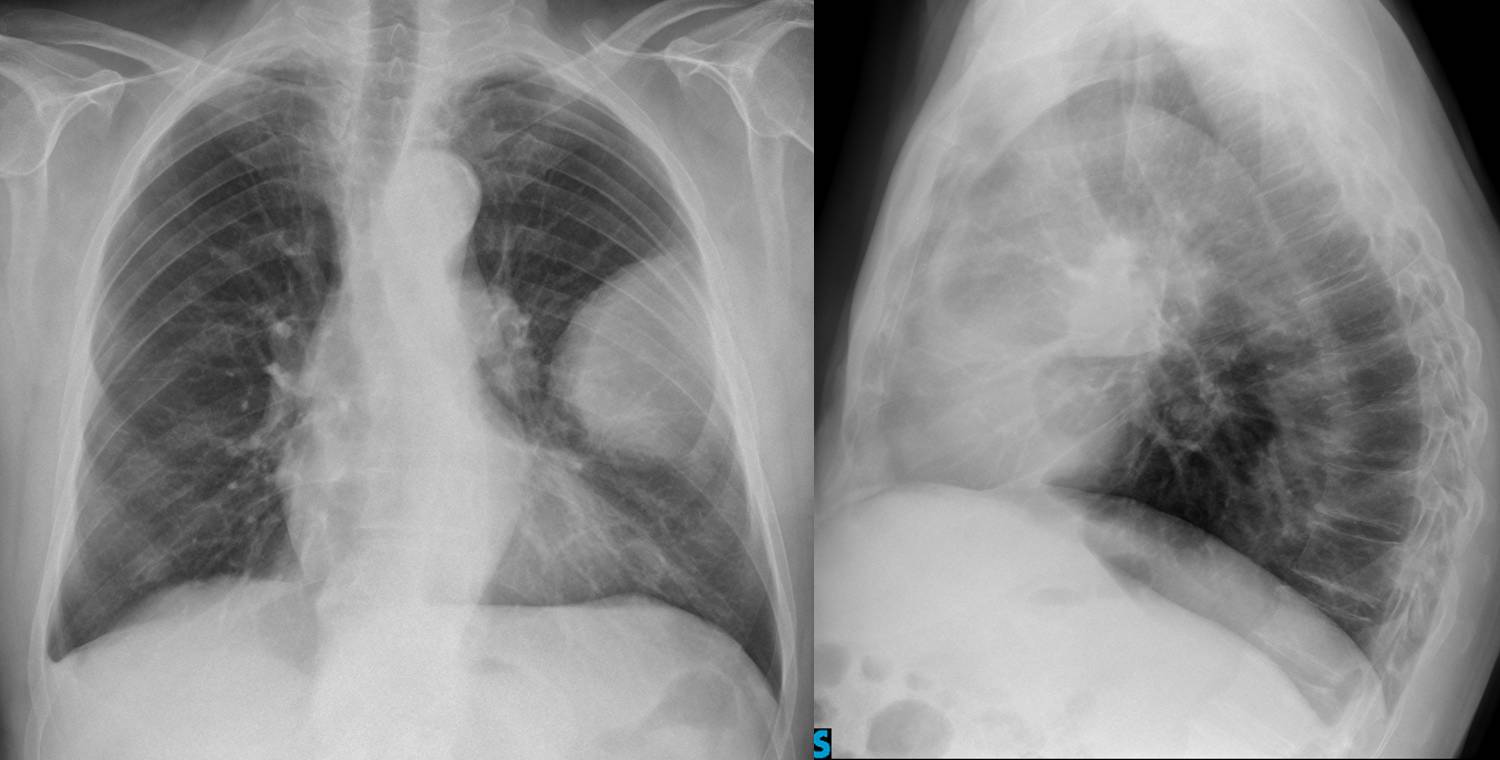
Extrapulmonary masses are easily identified by their typical appearance: location in the periphery of the lung, well-defined outline, and obtuse angles at the corners (pregnancy sign).
The differential diagnosis is simple: they may arise from a rib (metastasis, myeloma), chest wall (extrapleural fat) or pleura (pleural tumour, loculated fluid). Involvement of a rib is usually visible in the chest radiograph and narrows down the diagnosis to a malignant rib lesion. If no rib lesion is visible, the lesion can be of soft tissue density (tumour), water density (loculated fluid) or fat density (extrapleural fat). Differentiation between densities can only be made by CT.
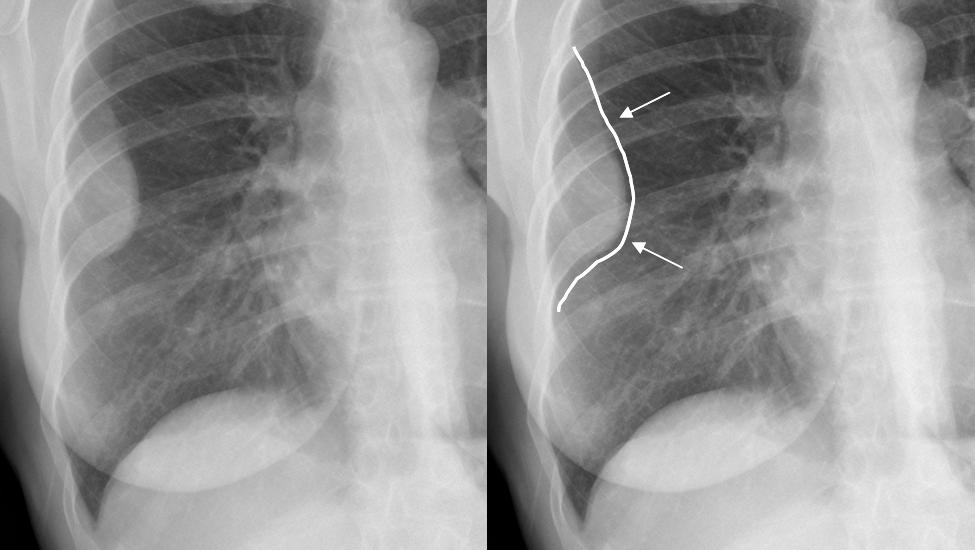
Fig. 4
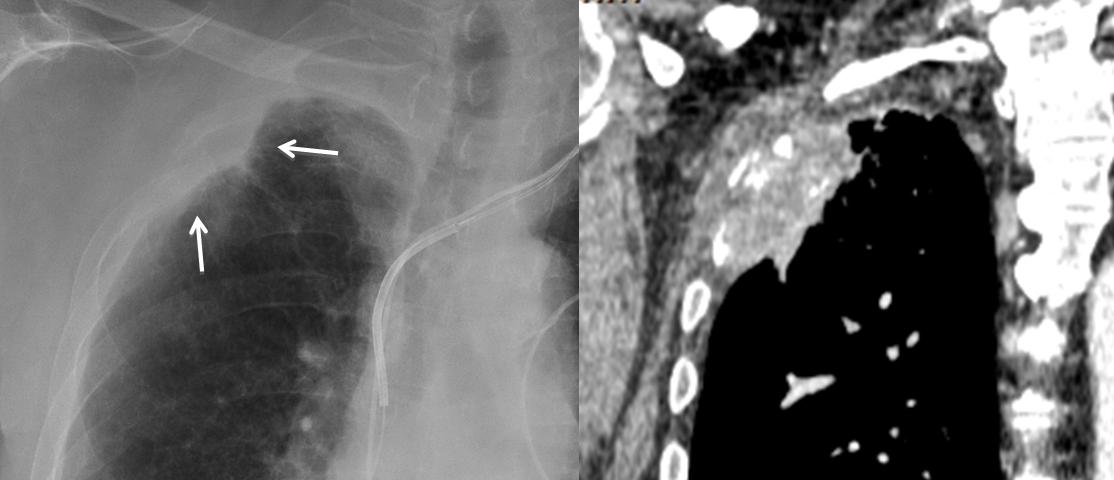
1. Fat Density
In this 57-year-old man we see carcinoma of the lung and left extrapleural lesion (arrow).
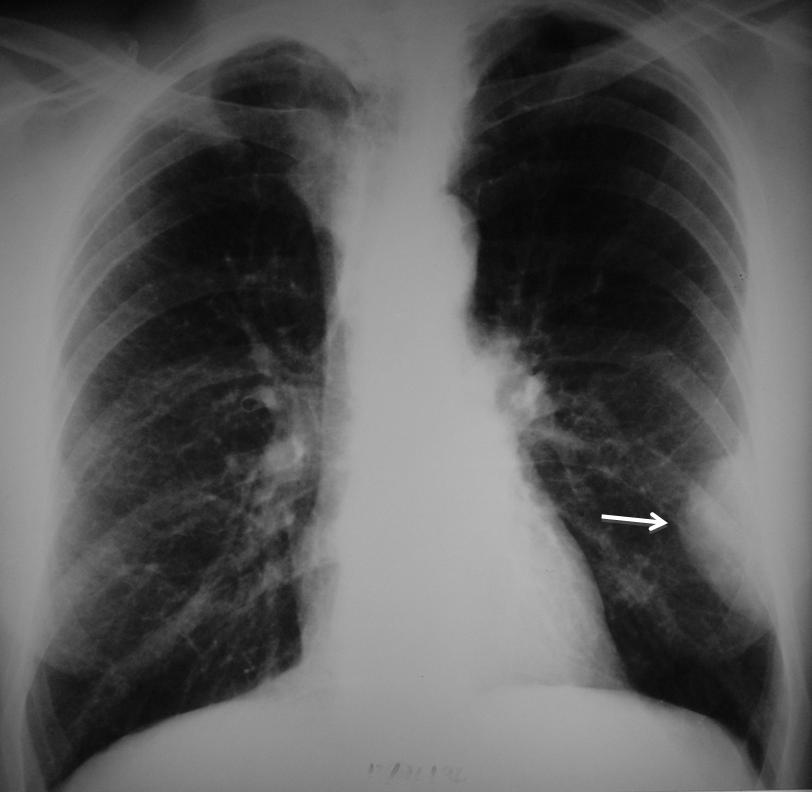
Fig 5
CT demonstrates that the lesion corresponds to extrapleural fat and is, therefore, innocuous.
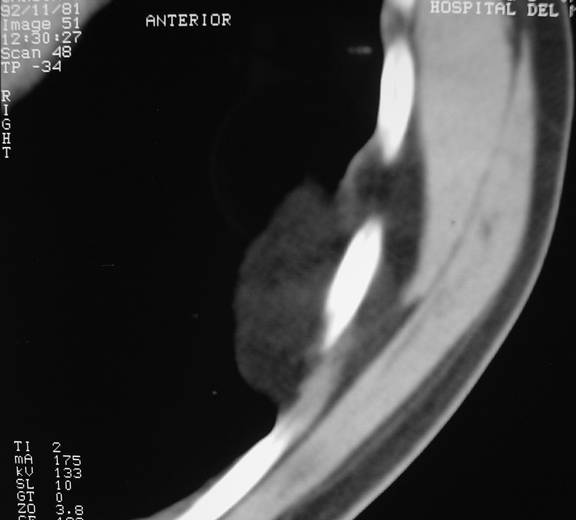
Fig 6
2. Water Density
Two patients with loculated fluid and typical ‘pregnancy sign’ in the chest radiograph.
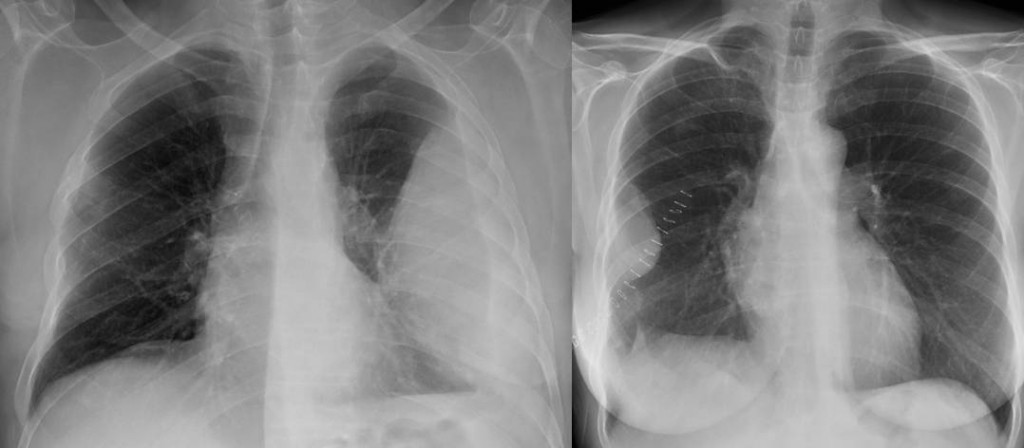
Fig 7
CT in one of them shows that the lesion is of water density, confirming the diagnosis.

Fig 8
Note that both patients show blunting of the costophrenic angle, which always accompanies loculated fluid.
3. Soft Tissue Density
The radiograph shows an extrapulmonary lesion (arrow). CT shows a soft-tissue density, which likely corresponds to a fibrous tumour of pleura. An alternative would be pleural metastasis.

Fig. 9
Pitfalls
A lesion with indistinct borders, like the one below, shouldn’t be mistaken for an extrapleural lesion. The ragged border in this case indicates a peripheral lung carcinoma invading the chest wall or, less commonly, a chest wall lesion invading the lung.
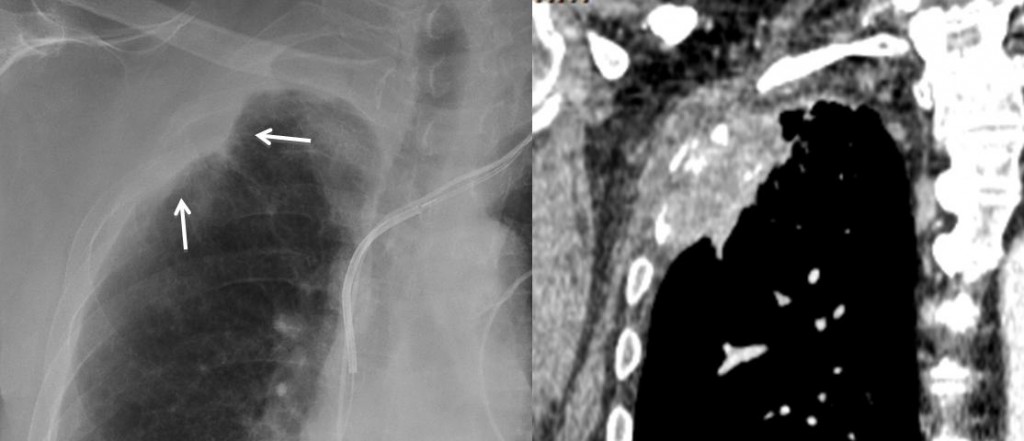
Fig 10
Follow Dr. Pepe’s advice:
- Extrapulmonary lesions are recognised in the chest radiograph by the so-called ‘pregnancy sign’.
- Always look for involvement of the underlying rib (metastases, myeloma).
- All others need a CT.
Suggested reading: chapter in chest wall lesions. JC Reed, Chest radiology. Patterns and differential diagnosis.



2. Fibrous tumour of pleura
Fibrous tumor of the pleura
well defined meduim denisty lesion with obtuse angle with chest wall in one side and acute in the other side and its basee related to the pleural surface confirm its chest wall origin and different shape in both views suggest fibrous tumor of the pleura
The opacity in the projection of the lateral aspect of the midzone of the left lung is definitely extrapulmonary. Since it is forming an obtuse angle with the chest wall, it looks like a pleural based mass.
No associated pleural effusion.
No bony abnormalities of the related ribs are seen – making it not typical of a myeloma met.
It does not look like extrapleural fat (site and appearance not typical).
So my answer is fibrous pleura of pleura.
La massa ha sede extra-pleurica:margini netti e raccordo con angoli ottusi al polomone.In LL essa si sovrappone all’ombra cardiaca, riducendone la opacità per immagini tenuemente rx-trasparenti.Penso allora ad una raccolta adiposa extra-pleurica.
For me it is an extrapulmonary lesions (well-defined soft- tissue masses,with angles obtuse to the chest wall)
I think it is located anteriorly because the anterior clear space is occupied.
I do not clearly see the anterior convexity of the 4th rib in the left hemithorax. So I think it may be a rib lesion
Fibrous tumour of pleura
So far, three people elcted fibrous tumor. Can you distinguish between tumor and extrapleural fat in the plain film?
extrapleural fat is not a localized mass
This is not true. See fig 5 in the answer section
no i cannot distinguish
i think of extraplural fat due the appearnce of seen through the normal lung tissue
All of the above…
I think is a extrapulmonar lesion. The anterior arch of the 4th left rib is missing, suggesting a extraplumonar lesion that is “destroying” the rib. Furthermore it has obtuses angles, which support the extrapulmonar origin. It may be due to a MM, metastases or another primary bone tumor.
Considering that the answer will be posted tomorrow, I have to congratulate you! You made the correct diagnosis, together with Mm.
2. Fibrous tumour of the pleura.
There is semiology about pleural or extrapleural lesions
I can´t see any rib lesion.
Extrapleural fat usually have “water” density on chest radiogrph. Extrapleural fat is usually seen in obese patients or patients with Cushing syndrome. This man doesn´t seem to be it. The “normal” position of extrapleural fat is seen on PA view around 6-7 to 10-11 ribs sometimes in one side some times in both sides. This is a more or less thin lyer. Then if this man had left extrapleural fat it would be “the mother” of extrapleural fats.
Extrapleural lipomas I´ve seen so far now are usually lesser dense than other extrapleural lesions such fibrous tumour of the pleura or neurogenic tumours.
Pain is not very usual in patients with non complicated fibrous tumour of the pleura. I could be a “complicated” pleural fibroma because bleeding, torsion or malignancy.
Fibrous tumour of pleura!
Fibrous tumour of pleura
The anterior Portion of the 4th rib is missing as mentioned above.
Together with pain this strongly suggests a rib lesion (metastasis).
A well defined lesion broad based towards pleura with obtuse angles suggest pleural/extrapleural pathology. There is associated destruction of the left 4th rib anteriorly. No calcification is seen within the lesion.possibilities include-MM/plasmacytoma/mets.Bone destruction is against fibrous tumor of the pleura/extrapleural fat.
i think that i an extrapleural lesion like myelolma muliple, therai’snt any rib destruction an ia the cuae posible , no metastasi no other causes formzs an angle agude in PA in anterio in lateral
Good. Ready to take your Diploma examination
my ansewr is all of the above and more
amazing work. lista de emails lista de emails lista de emails lista de emails lista de emails