Dr. Pepe’s Diploma Casebook: Case 100 – A painless approach to interpretation (Chapter 7) – SOLVED!
Dear Friends,
Today I present the seventh chapter of the Painless Approach to Interpretation, which also happens to be case number 100 of Dr. Pepe’s Diploma Casebook. It makes me very proud to have shared with you one hundred cases and hope they have been useful.
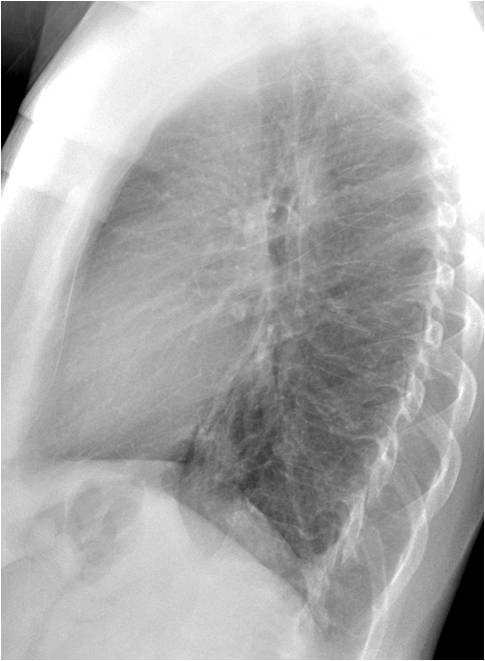
Showing chest radiographs of a 47-year-old woman with mild fever and chest pain.
What do you see? Check the images below, leave me your thoughts in the comments section and come back on Friday for the answer.

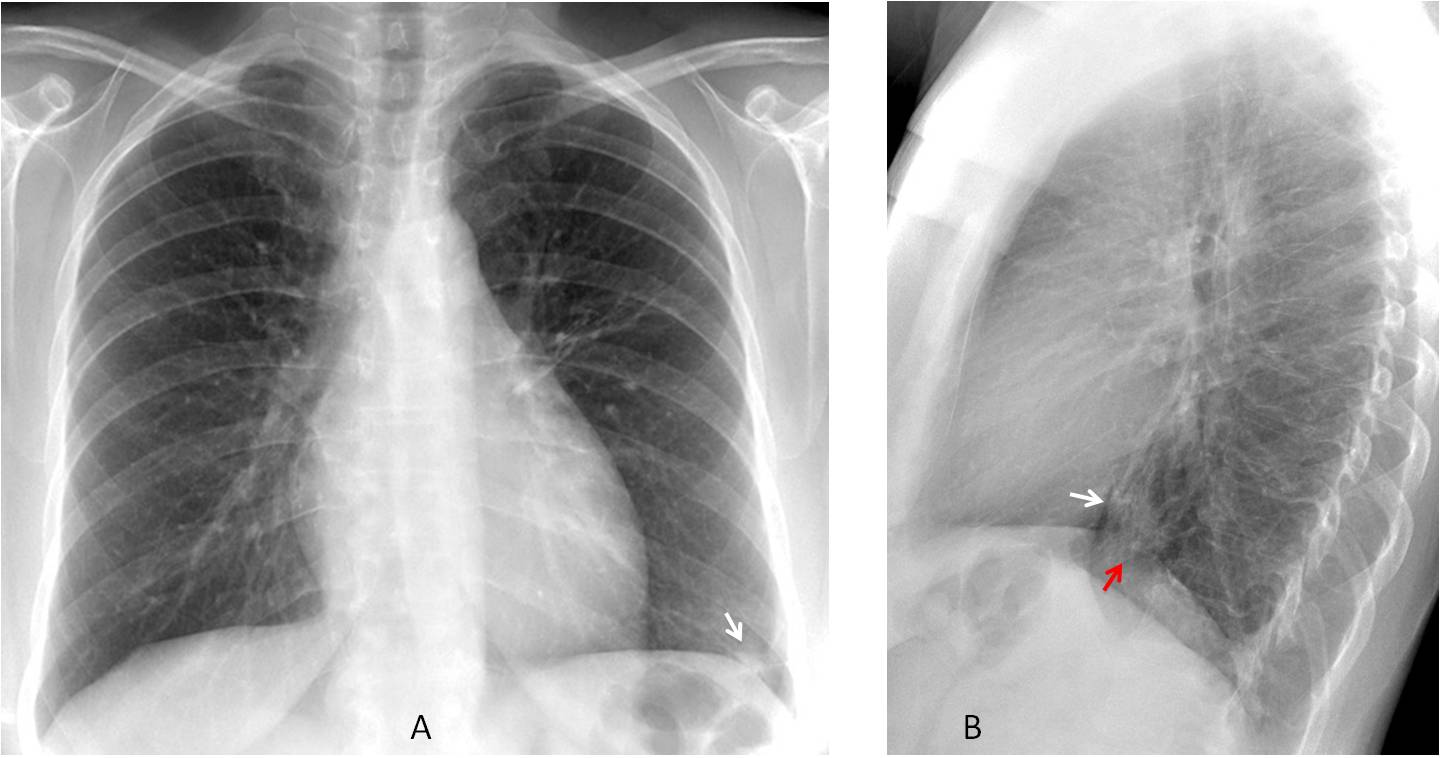
Findings: PA radiograph shows a small infiltrate in the left costophrenic sinus (A, arrow). Lateral view shows an ill-defined opacity with air bronchogram in the retrocardiac space (B, white arrow) with blurring of the dome of the left hemidiaphragm (B, red arrow)
Together with the clinical information, the findings are highly suggestive of an acute inflammatory process, hidden in the PA view. After treatment two weeks later, the follow-up film shows that the findings have disappeared (C and D, circles) .
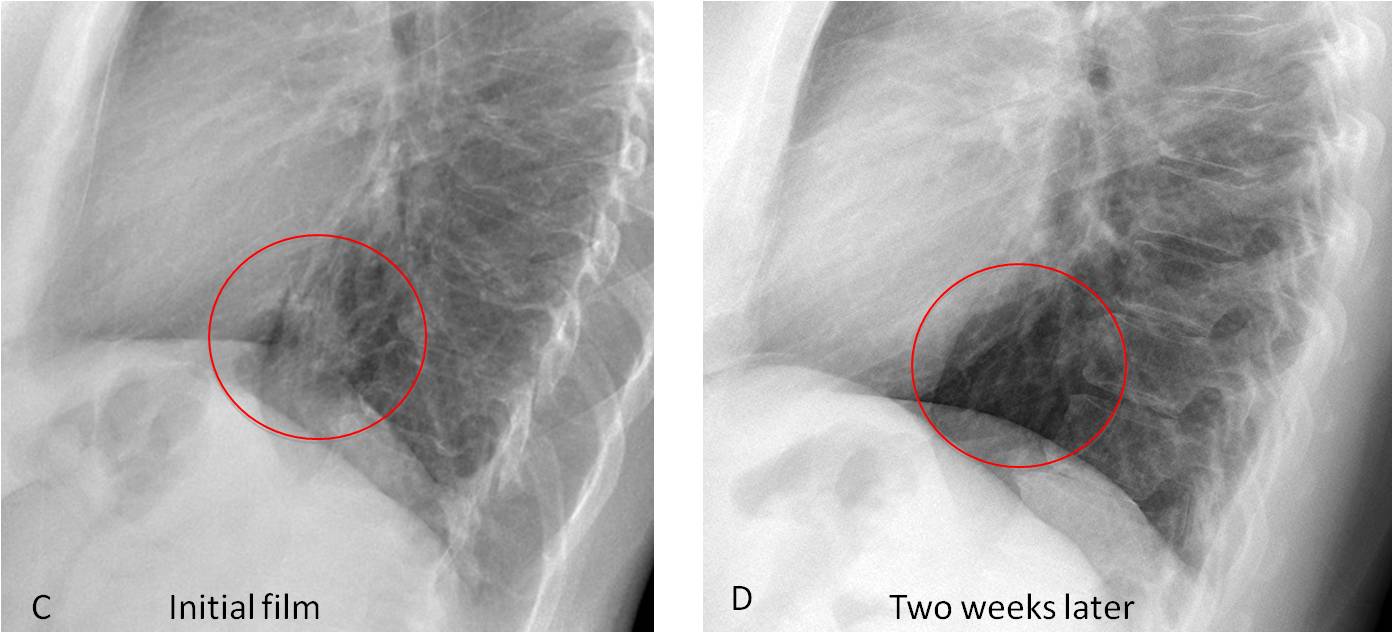
Final diagnosis: retrocardiac pneumonia, discovered in the lateral view.
The purpose of this case is to emphasise the importance of the lateral view in the discovery of chest abnormalities. In the PA radiograph, around 20-25% of the lung surface is hidden by other structures, mainly the mediastinum and diaphragm. The lateral view helps to visualise these occult areas. It also contributes to interpreting abnormalities that may have a confusing appearance in the PA view and are more clearly depicted in the lateral radiograph.
Many physicians and some radiologists are intimidated by the lateral view. In the next two chapters I intend to provide them with a checklist that will facilitate the interpretation.
The initial checklist in the lateral radiograph includes the following areas:
1. Anterior clear space
2. Posterior clear space
3. Retrocardiac space
4. Lung fissures
The anterior clear space corresponds to the dark area behind the sternum in the lateral view. It is limited anteriorly by the sternum and posteriorly by vascular structures (ascending aorta and main pulmonary artery) (Fig. 1).
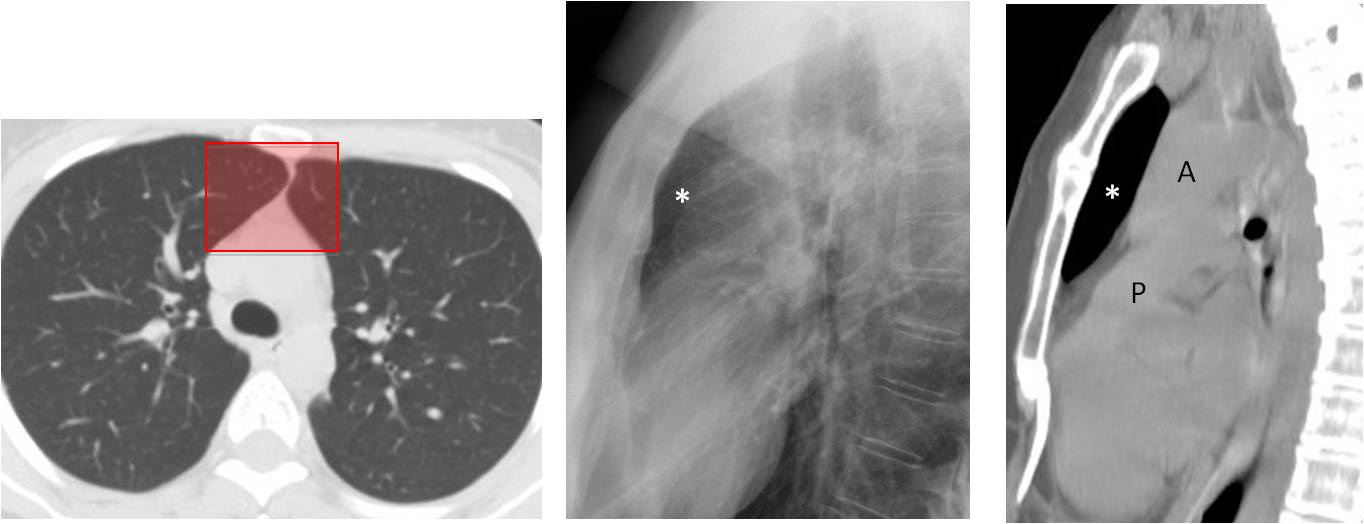
Fig. 1
Fig. 1. Axial CT showing the area of lung hidden in the PA view (A, shaded rectangle), which represents the anterior clear space in the lateral view and the sagittal CT image (B and C, asterisks). A, aorta; P, pulmonary artery
Pathologic conditions in the anterior clear space are hidden in the PA view by superimposition of the sternum and mediastinal structures, but they are clearly visible in the lateral projection. Abnormalities in this specific area usually correspond to masses of the anterior mediastinum (Fig. 2). They may also arise from the pleura/chest wall or lung (Fig. 3).
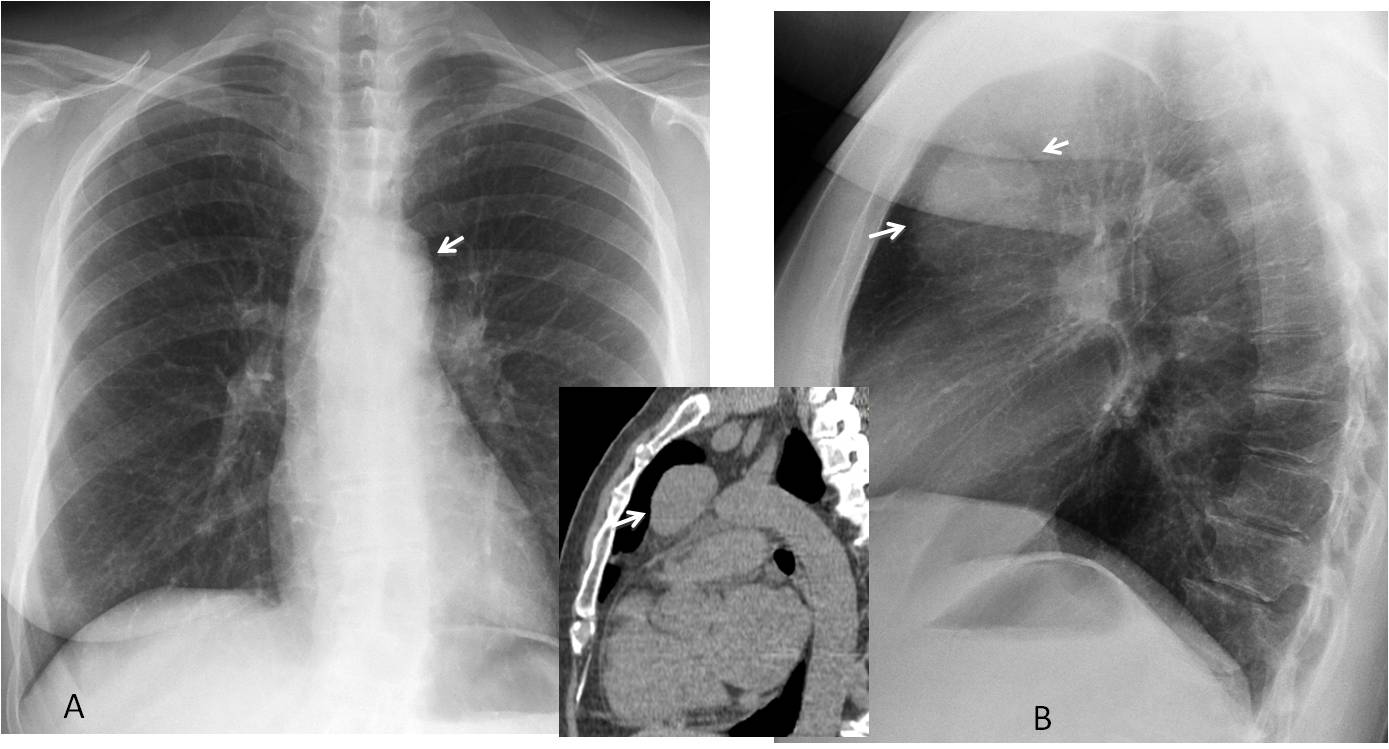
Fig. 2
Fig. 2. 57-year-old woman with myasthenia gravis. PA radiograph shows a barely visible double contour of the aortic knob (A, arrow). In the lateral view, a large round mass is seen in the anterior clear space (B, arrows). Unenhanced sagittal CT confirms the mass (insert, arrow). Diagnosis: thymoma.
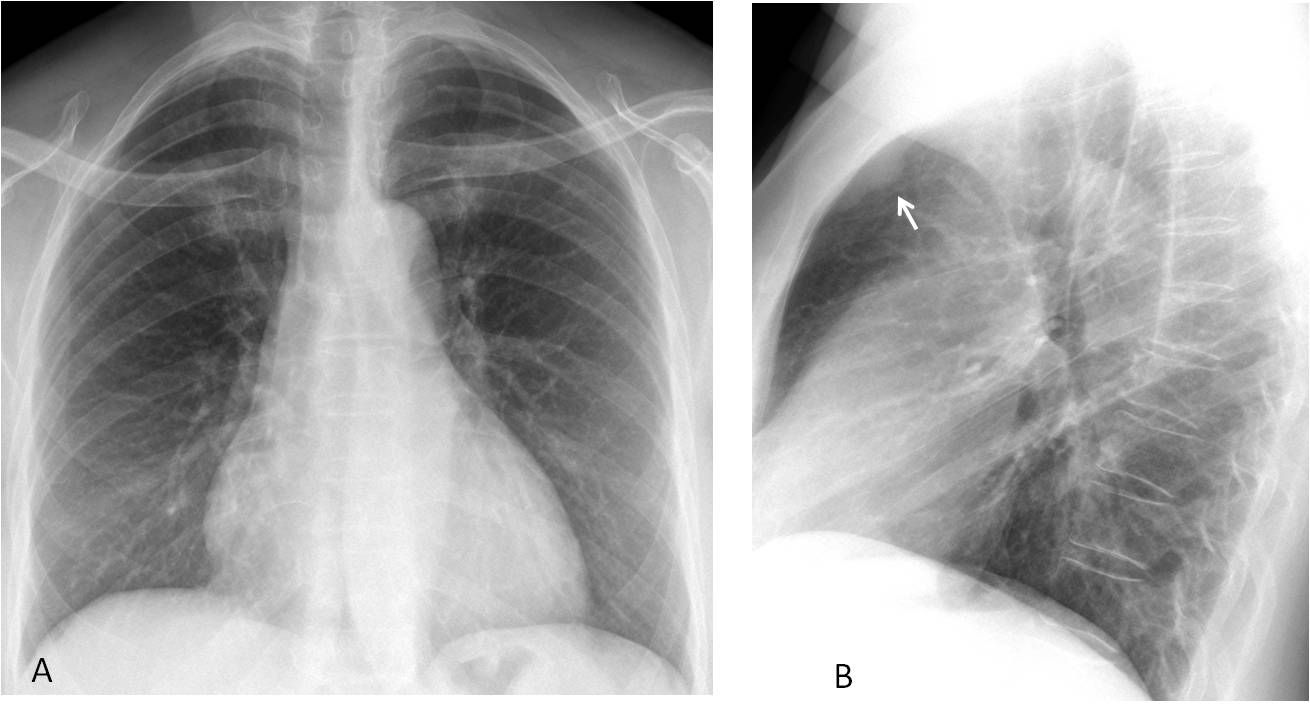
Fig. 3 (a,b)
Fig. 3. Routine follow-up chest films in a 54-year-old woman who had undergone surgery for breast carcinoma. The lateral view shows an extrapulmonary mass in the anterior clear space (B, arrow) that is not visible in the PA radiograph (A).
Comparison with previous radiographs taken a year earlier shows that the mass was present, albeit smaller (C and D, arrows). Sagittal CT confirms the extrapulmonary mass (E, arrow). Surgical diagnosis: metastatic internal mammary lymph nodes.
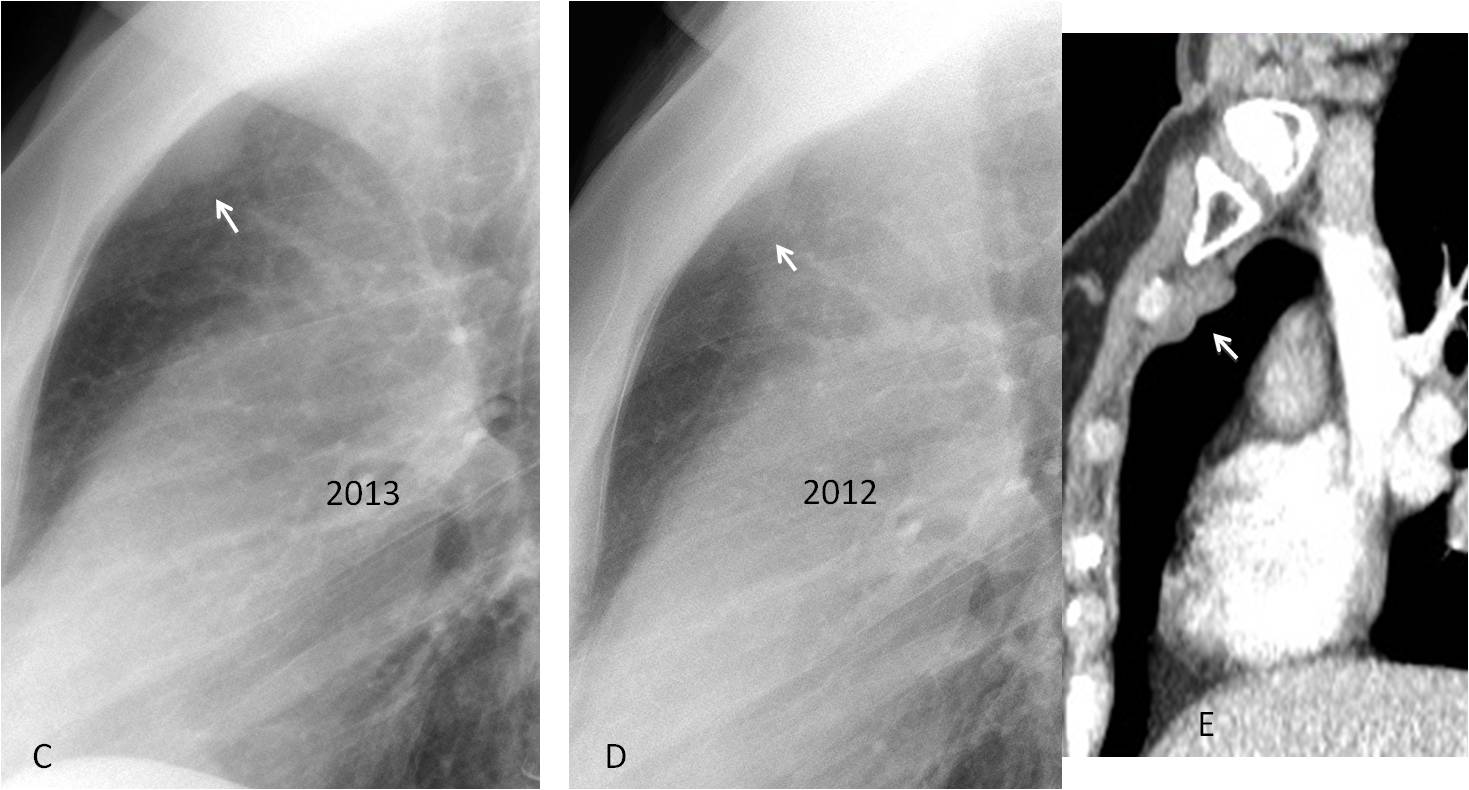
Fig. 3 (c,d,e)
The posterior clear space refers to the area between the oblique posterior diaphragm and the chest wall. This space is hidden in the PA view by the dome of the diaphragm (Fig. 4). Abnormalities in the posterior clear space are easily visible in the lateral view. They may arise from the lung, pleura, or diaphragm. Like the pulmonary apices, the posterior clear space is a narrow region, hence the origin of the abnormality may be difficult to determine. In most cases, CT is needed to confirm the finding and determine the origin.
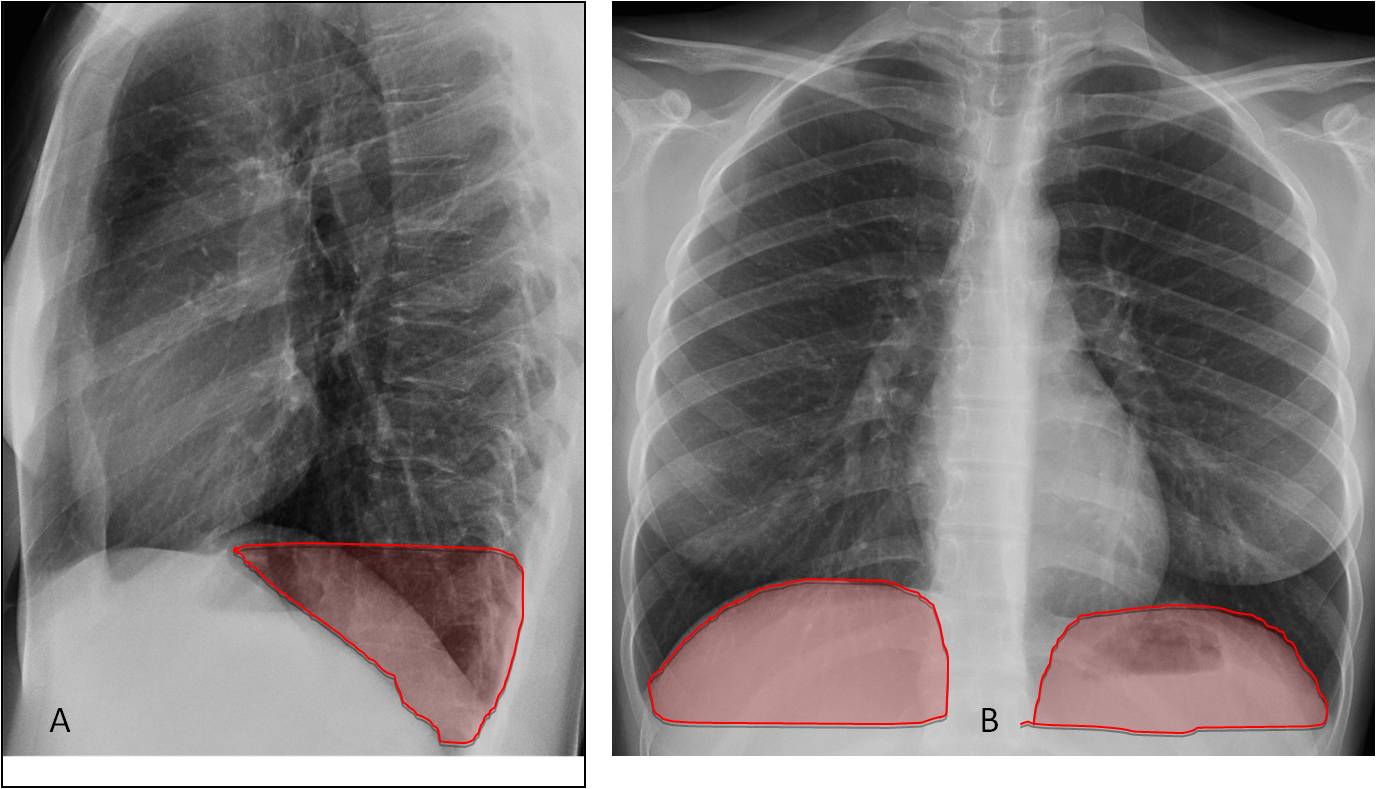
Fig. 4. Lateral view showing the posterior clear space (A, shaded area) located in the PA view behind the diaphragmatic domes (B, shaded areas).
Pleural fluid is the most common finding in the posterior clear space. Small amounts of fluid may be invisible in the PA view, but are easily identified in the posterior costophrenic sinus in the lateral radiograph by the typical concave shape (Fig. 5). Occasionally, pulmonary disease can also locate in this space and be invisible in the PA view (Fig. 6).
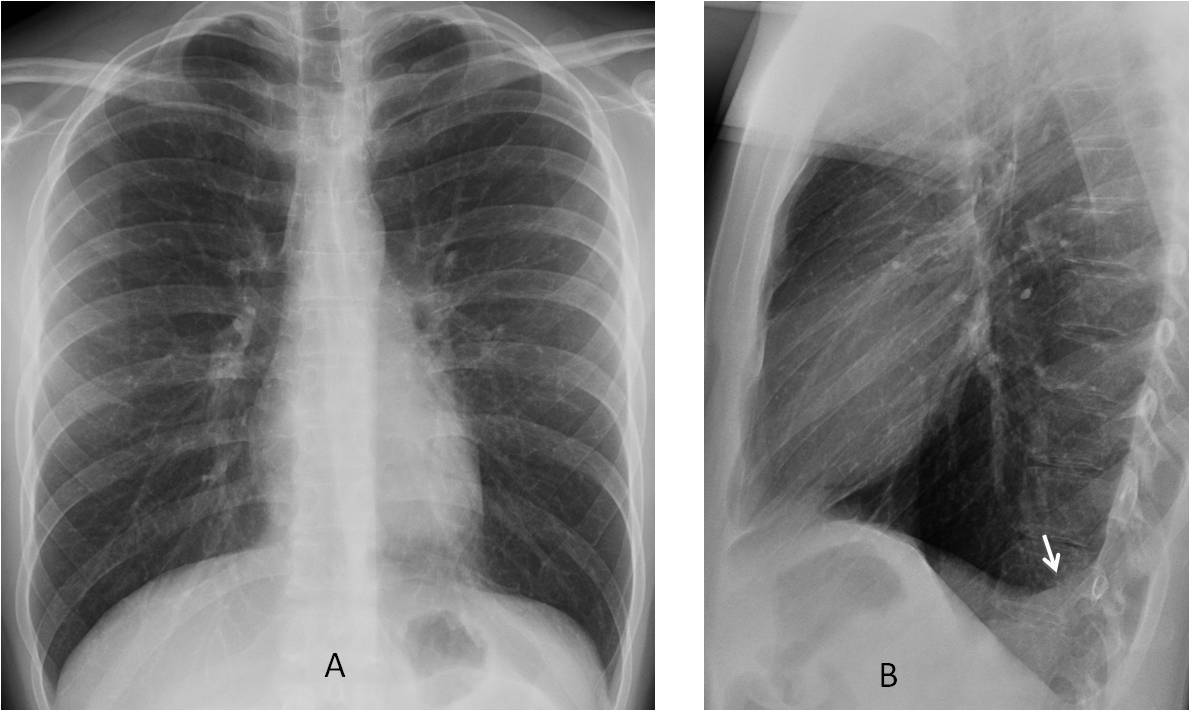
Fig. 5
Fig. 5. 29-year-old man with pleuritic pain. PA view (A) is unremarkable. Lateral view (B) shows the typical appearance of free pleural fluid in the posterior sulcus (arrow).
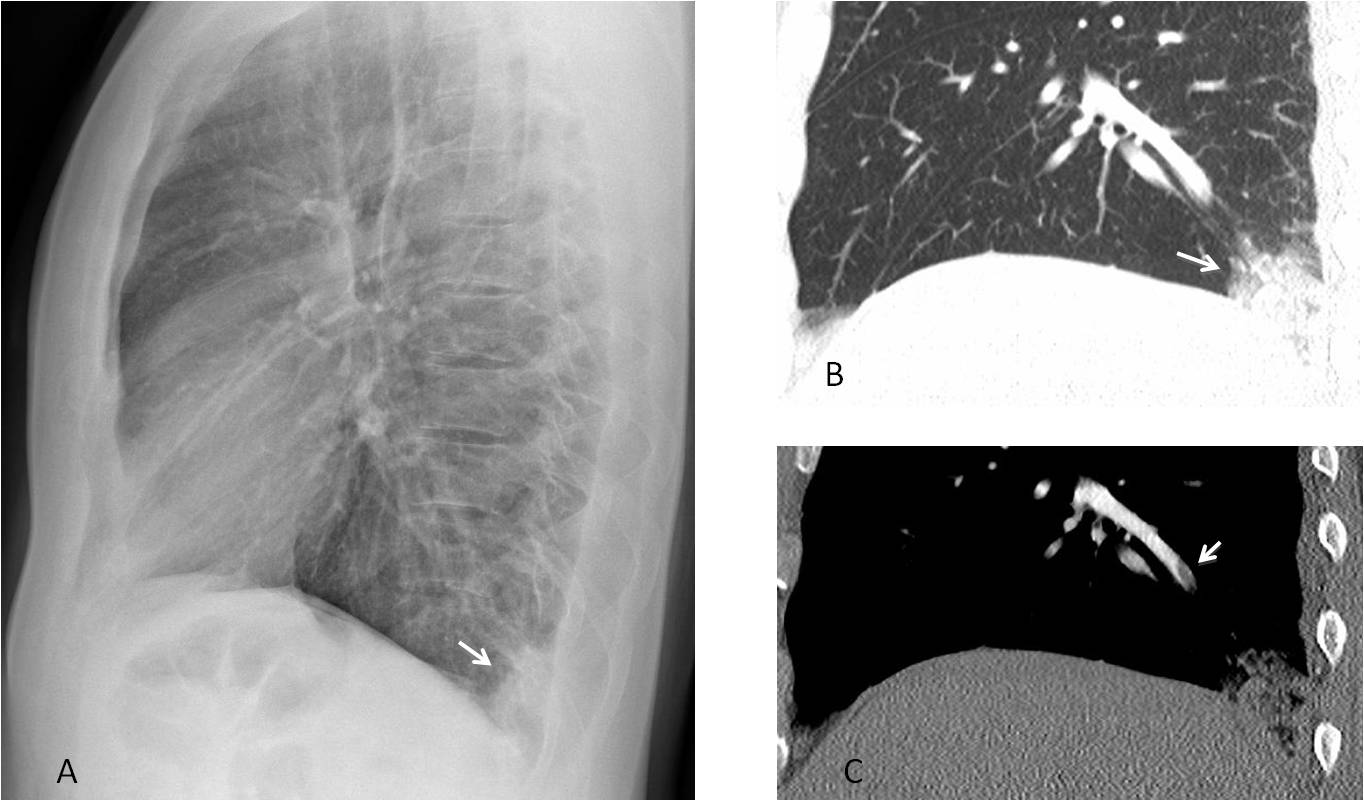
Fig. 6
Fig. 6. 54-year-old man with sudden chest pain. The PA chest film was unremarkable. The lateral view shows a Hampton hump in the posterior costophrenic sulcus (A, arrow). Enhanced sagittal CT confirms the Hampton hump (B, arrow) and depicts an embolus in a segmental artery (C, arrow).
The retrocardiac space is the dark area located behind the heart in the lateral view, limited by the hila, spine and diaphragm (Fig. 7). Lesions in this area are hidden by the cardiac shadow in the PA radiograph, but are cearly visible in the lateral view.
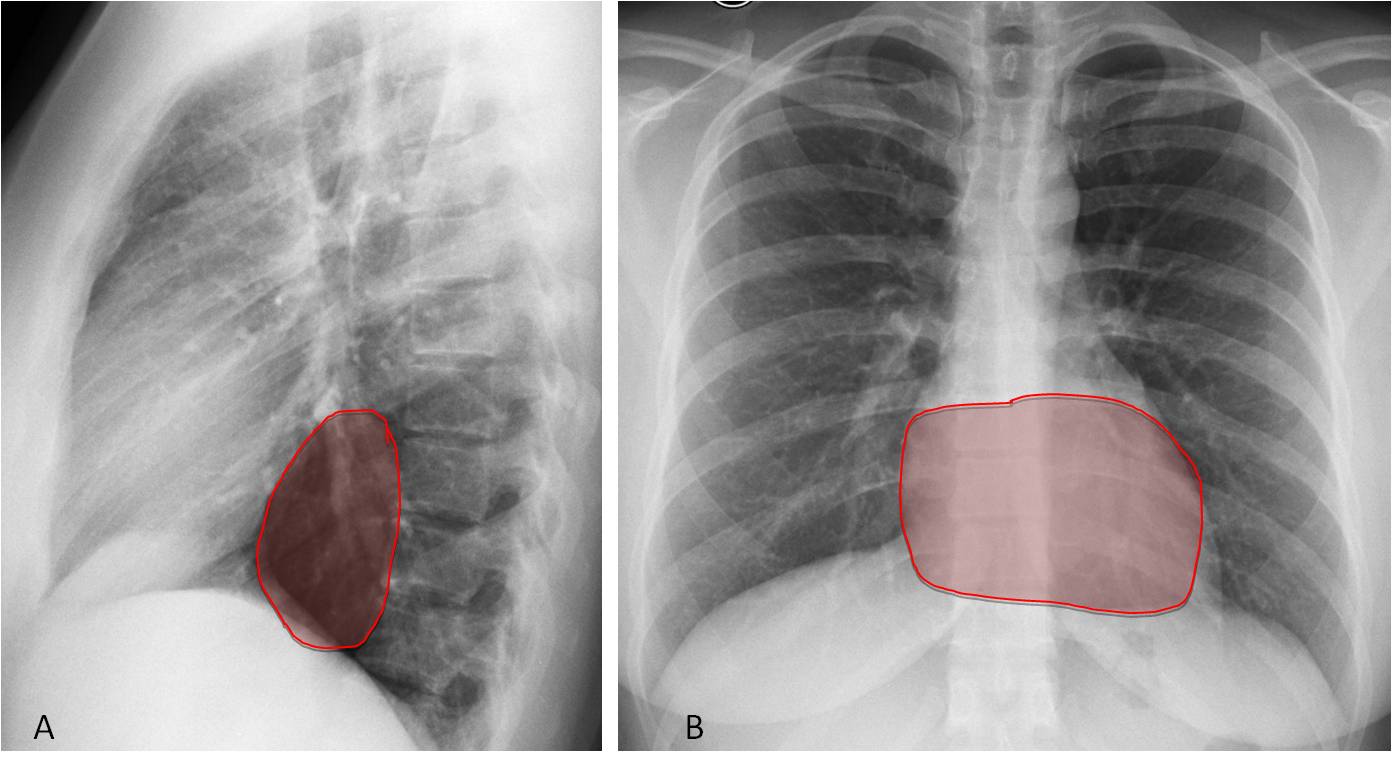
Fig. 7
Fig. 7. Retrocardiac space in the lateral view (A, shaded area), which is obscured in the PA view by the cardiac shadow (B, shaded area).
The most common abnormality in the retrocardiac space is hiatal hernia. It may be airless and should not be confused with a mediastinal mass (Fig. 8). Less often, pulmonary infiltrates can also occur in this area (Fig. 9).
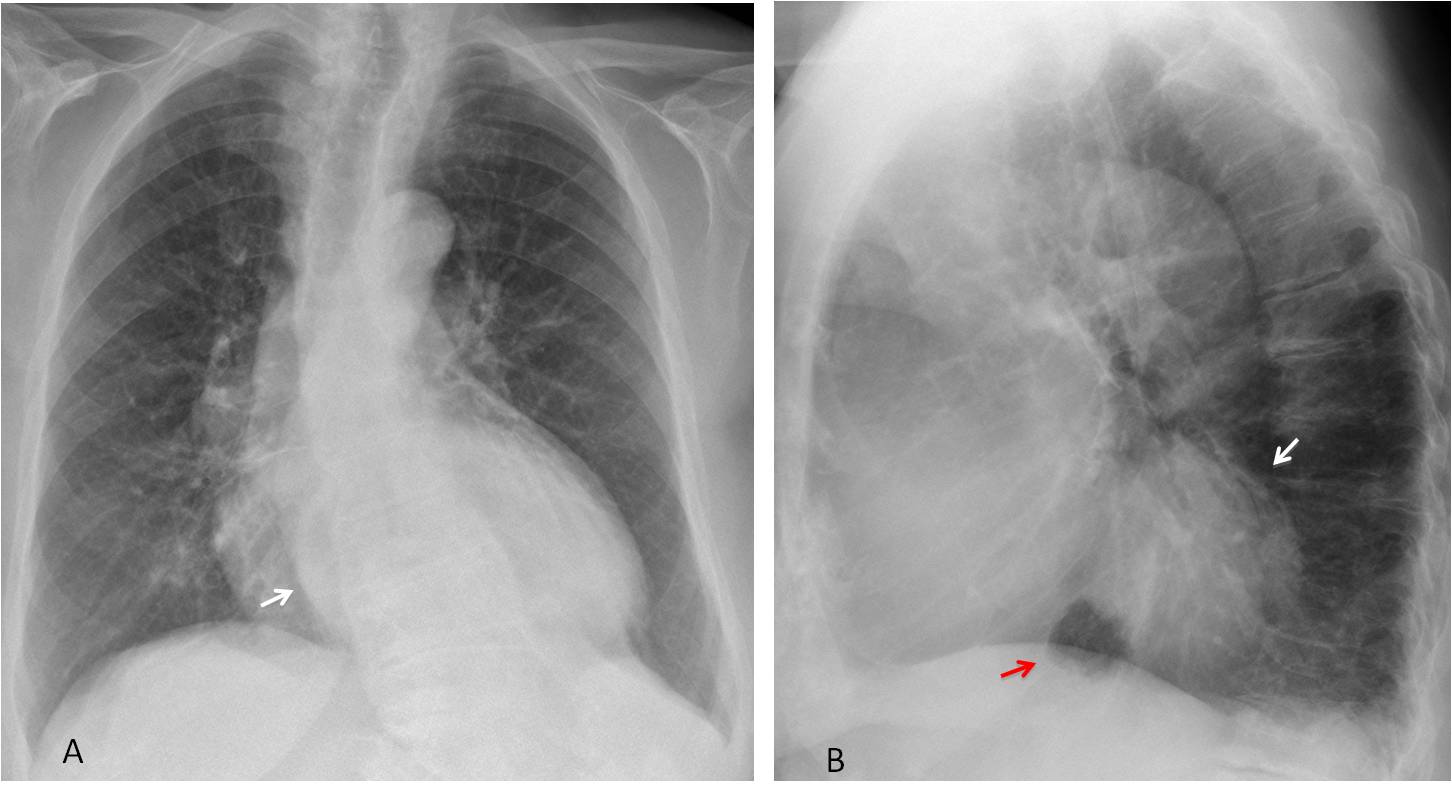
Fig. 8
Fig. 8. Large hiatal hernia, barely visible in the PA view (A, arrow), occupying the retrocardiac space in the lateral radiograph (B, white arrow). Note the small amount of gastric air at the base of the hernia (B, red arrow).
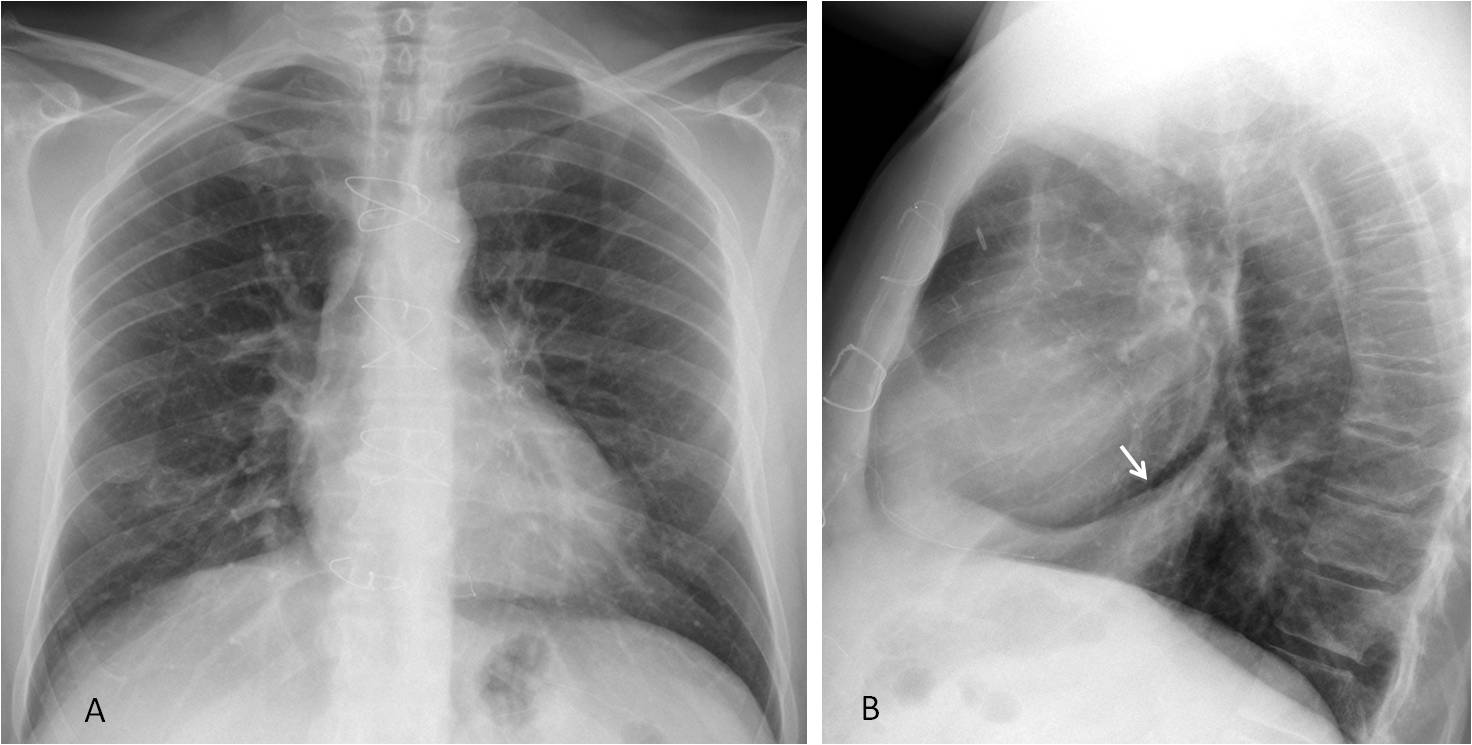
Fig. 9
Fig. 9. Segmental pneumonia in the retrocardiac space, not visible in the PA view (A) and clearly depicted in the lateral radiograph (B, arrow).
The minor and major fissures are visible in a fair number of lateral chest radiographs. They are important landmarks to detect volume loss of the lobes, a common consequence of fibrotic TB (Fig. 10) or bronchogenic carcinoma (Fig. 11).
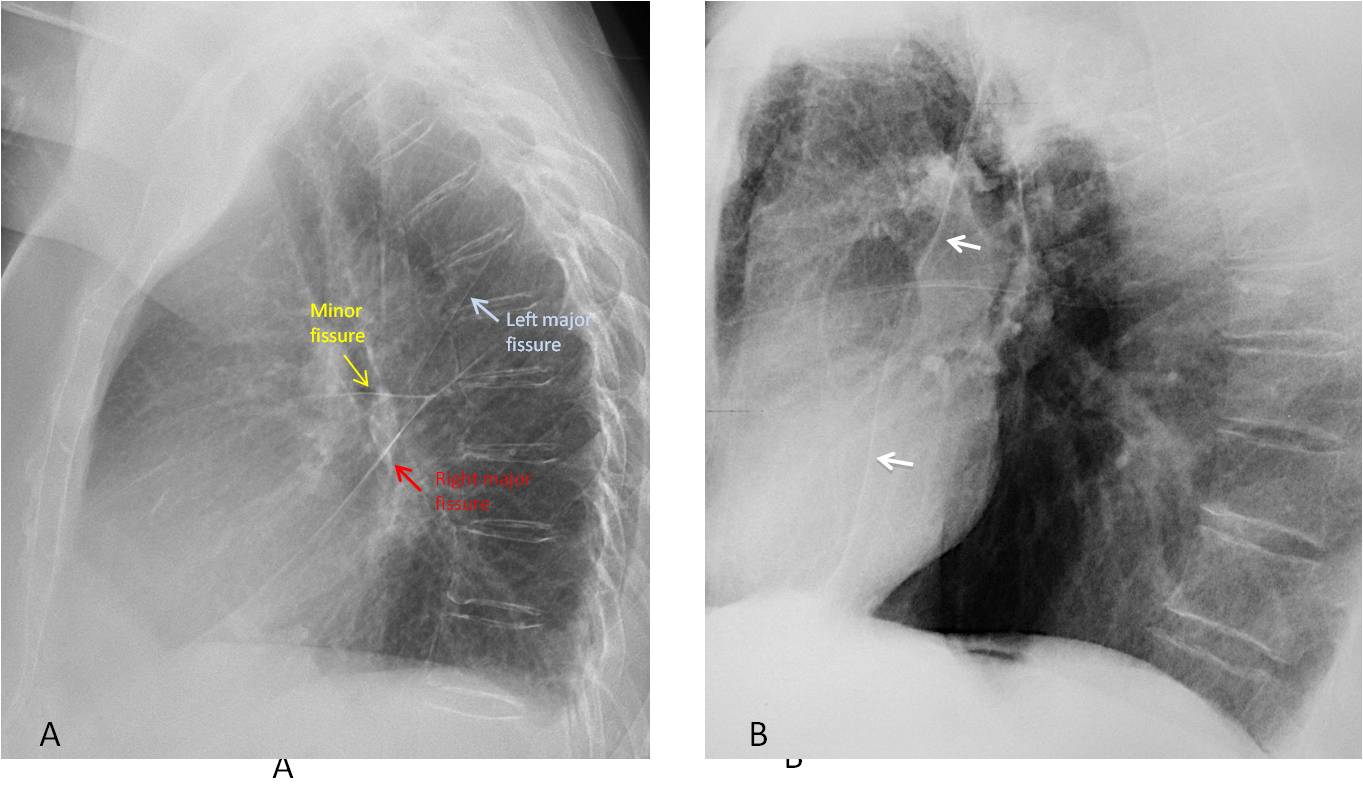
Fig. 10
Fig. 10. A. Normal location of lung fissures in the lateral view. Anterior displacement of the left major fissure (B, arrows) due to LUL volume loss secondary to chronic TB.
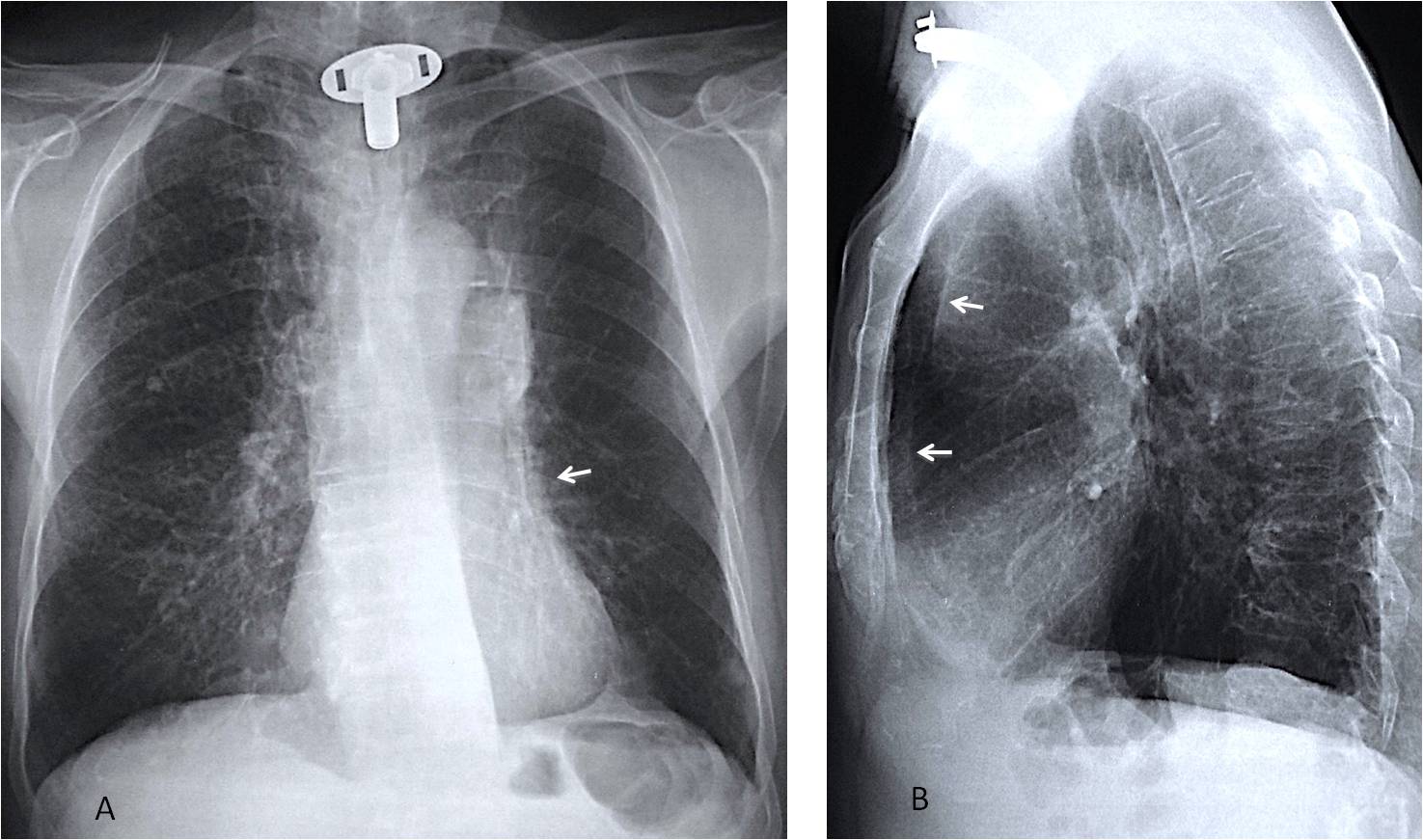
Fig. 11
Fig. 11. Routine control of an 82-year-old man after surgery for carcinoma of the larynx ten years ago. PA view shows abnormal right hilum and blurring of the left cardiac contour (A, arrow). Lateral view shows marked forward displacement of the left major fissure (B, arrows) indicating severe LUL collapse, confirmed to be due to bronchogenic carcinoma.
In conclusion, the following areas should be investigated in the lateral view:
The anterior clear space, to evaluate lesions that are not visible in the PA radiograph, the most common being anterior mediastinal masses.
The posterior clear space; the most frequent abnormality in this area is pleural effusion.
The retrocardiac space; Hiatal hernia is the most common finding.
The lung fissures, to detect displacement that may herald the presence of a central carcinoma.
Next time, I’ll finish with the checklists.

Follow Dr. Pepe’s advice:
In the lateral chest radiograph look for:
Mediastinal mass in the anterior clear space
Opacities in the posterior clear space, mainly pleural fluid
Opacity of the retrocardiac space, most likely hiatal hernia
Displacement of the lung fissures


Where is everybody?
Opacity below the right cardiophrenic angle,opacity in the left costophrenic angle.
Mitral shape of the heart suggests mitral stenosis/insufficiency.
On lateral view slightly inhomogeneous shadow in left lower lobe – ddx: inflammation/hypoventilation left lower lobe
Or probable inflammation of the heart – endocarditis
Can you diagnose endocarditis in the plain film?
Of course, no, but the combination of clinical data and the plain film information make me to think about ddx and further diagnostic algorithm. The laboratory data and heart USD needed
Of course, no. But the combination of clinical data and the plain film information make me to think about the ddx and the next steps of diagnostic algorithm. The laboratory data and heart USD needed
I meant I can not diagnose endocarditis directly on plain film but indirectly
Irregularity and erosions along vertebral endplates of lower thoracic vertebra, may represent discitis
There is also minimal opacity in base of left lung
Pericarditis
I don´t believe pericarditis can be dignosed in the plain film, unless a pericardial fat sign is present (and it is not in this case)
cardiac sillhouete is enlargement
The heart is enlarged, cardiomegaly. I cant delimitate the aorto-pulmonary window. In the lateral view there is an opacity posterior to the left atrium and silhouette sign with the right hemidiaphragm is present.
Increased density at the level of the left principal bronchious.
Alveolar opacity near to the left costophrenic angle.
Cardiac pathology? Endo-pericarditis with alveolar opacities.
Are you sure that the heart is enlarged?
Not really
There is some increased inhomogeneous opacity in the left lower zone adjacent to the left costophrenic sulcus. This may represent a developing focus of consolidation in the context of patient symptoms.
Heart size appears normal.
There are degenerative discovertebral changes seen as osteophytes and lower thoracic facetal hypertrophy particularly at D11 -D12 vertebral level
RV enlarged.
Eso dilated – ?achalasia (narrowing seen in lat)
Focal erosion lt clavicle
Normal paraesopheal line in the PA view goes against achalasia.
Hpt fits erosion and gerd (eso narrowing) but rvh?
right ventricle appears hypertrophic on lateral xray. vasculits needs to be excluded.
now seeing on proper pc becoming more confused!
RVH.
Soft nodule right paratracheal region near apex.
Small wedge opacity left base peripherally.
Erosion inferior border left clavicle.
Not achalasia, but unconvinced GE junction normal
An opacity is noted in the left base. Osteoporotic changes are seen in the vertebra. Pruning of the pulmonary artery noted. On consideration with chest pain,Pulmonary embolism cannot be ruled out.
there is an opacity in the right apex and lobulated mass adjacent to the vertebral column – in posterior mediastinum.
Also the right paraspinal line has abnormal bulge at the level of the right hilum – mass in the paraspinal space?
Below the right hilum there is also opacity but with no siluette sign , it sugests ( together wirh lat. view)pulmonary inflamatory changes or athelectasis in PS7 and 10 due to the posterior mediastinal mass.
There is a thickening/increased linear opacity at the level of the right inferior paravertebral line, and if we compare with the lateral view, perhaps the diaphragm sillhoutte`s sign is because of an atelectasis of the RLL. The carina level is displaced towards the right side.
Alveolar opacity near to the left costophrenic angle.
…Galactico Professore…..vi è una area di disomogeneo addensamento parenchimale in sede paracardiaca basale sx, con velatura del seno costovertebrale, da piccolo versamento pleurico reattivo….il tutto spiega la febbre ed il dolore toracico….ma,ma, ma non vedo il primo arco superiore d della silhouette mediastinica, riferibile all’arco ascendente della ‘aorta…..pertanto due patologie….una riferibile alla patologia attuale e l’altra “incidentale”, di natura vascolare….aspettando la TC un caro saluto da Bari…..
Linear atelectasis left costophrenic angle.
Peribronchial opacity in the left lower lobe with loss of the retro cardiac black space on the lateral in keeping with alveolar opacity secondary to infection.
Note sure about the next bit …. The main pulmonary outflow tract is prominent. The heart is not enlarged so no evidence of a shunt. Consider pulmonary valve stenosis. Given this and the lung opacity consider sub acute bacterial endocarditis involving pulmonary valve.
Why not keep it simple? What is wrong with pneumonia, given the findings and the symptoms?
LLL or RLL?
There is an infiltrate in the anterior segment of LLL in the PA view which also involves the same segment in the lateral view. Pneumonia has to be in the LLL.
Thanks you are right. I’d report it as pneumonia in my day job but thought there must be an added twist? I definitely wouldn’t have suggested pulmonary valve stenosis in my day job!
[…] to complete the checklist for the lateral chest radiograph. In addition to the regions described in Diploma Casebook case 100, we should examine the following areas, most of which are hidden in the PA […]