Dr. Pepe’s Diploma Casebook: Case 101 – A painless approach to interpretation (Chapter 8) – SOLVED!
Dear Friends,
Today I am presenting the last chapter of the Painless Approach to Interpretation. Showing chest radiographs taken during an annual check-up of a 70-year-old man.
What do you see? Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.


Findings: PA radiograph (A) is unremarkable. Lateral view shows a rounded shadow projected over the spine (B, arrow), that was not visible one year before (C).
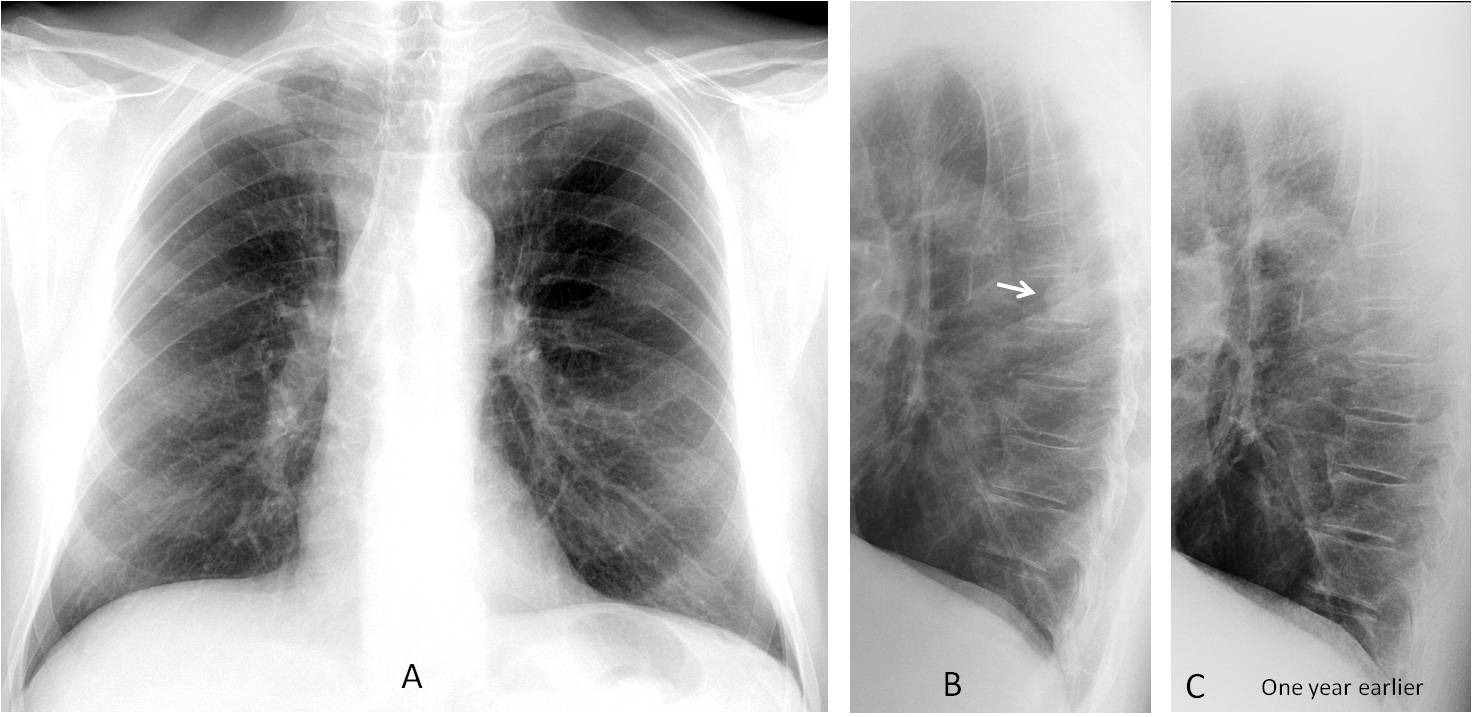
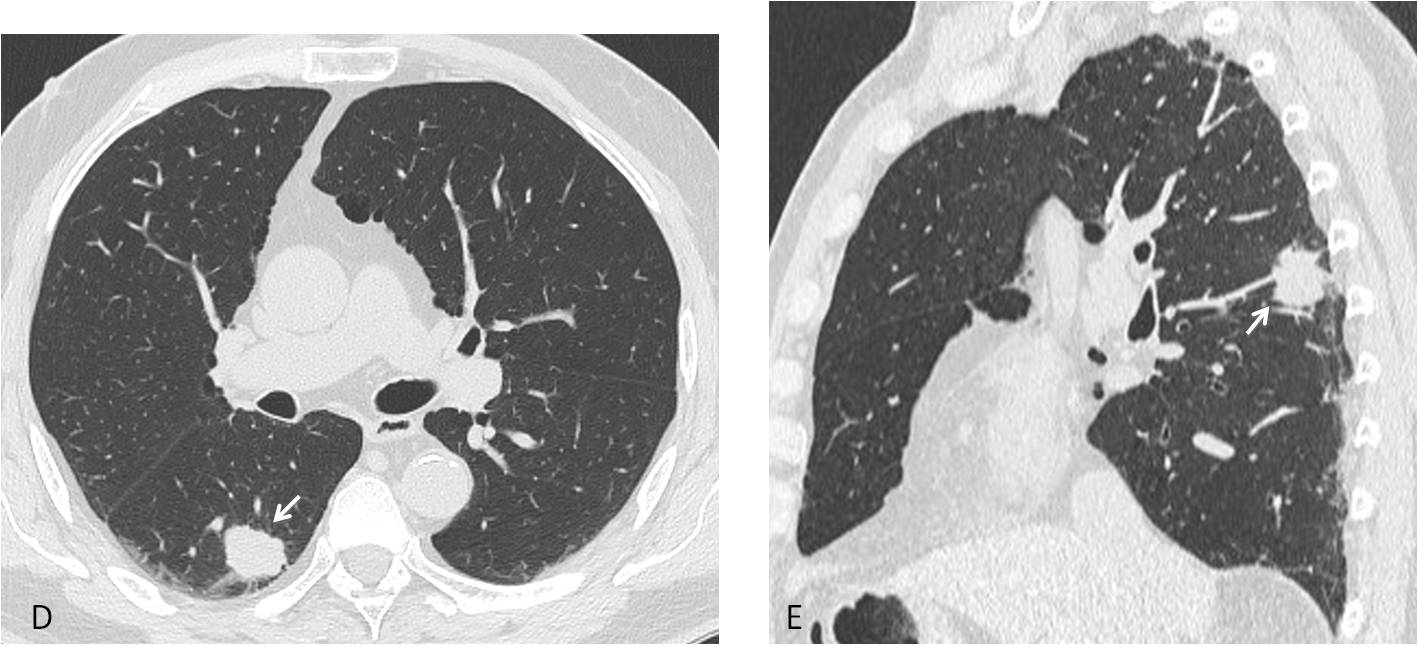
Axial and sagittal CT show an ill-defined nodule in the apical segment of the RLL (D and E, arrows). Needle biopsy confirmed the diagnosis of carcinoma.
Final diagnosis: lung carcinoma, hidden by the right hilum in the PA view.
In this presentation I intend to complete the checklist for the lateral chest radiograph. In addition to the regions described in Diploma Casebook case 100, we should examine the following areas, most of which are hidden in the PA view:
1. Thoracic spine and sternum
2. Middle mediastinum
3. Hila
4. Heart
The thoracic spine is hidden by the mediastinum in the PA view and is clearly depicted in the lateral view. Pathologic conditions may affect the spinal components (vertebral bodies or disk spaces) (Fig. 1) or be projected over the spine, as in the initial case.
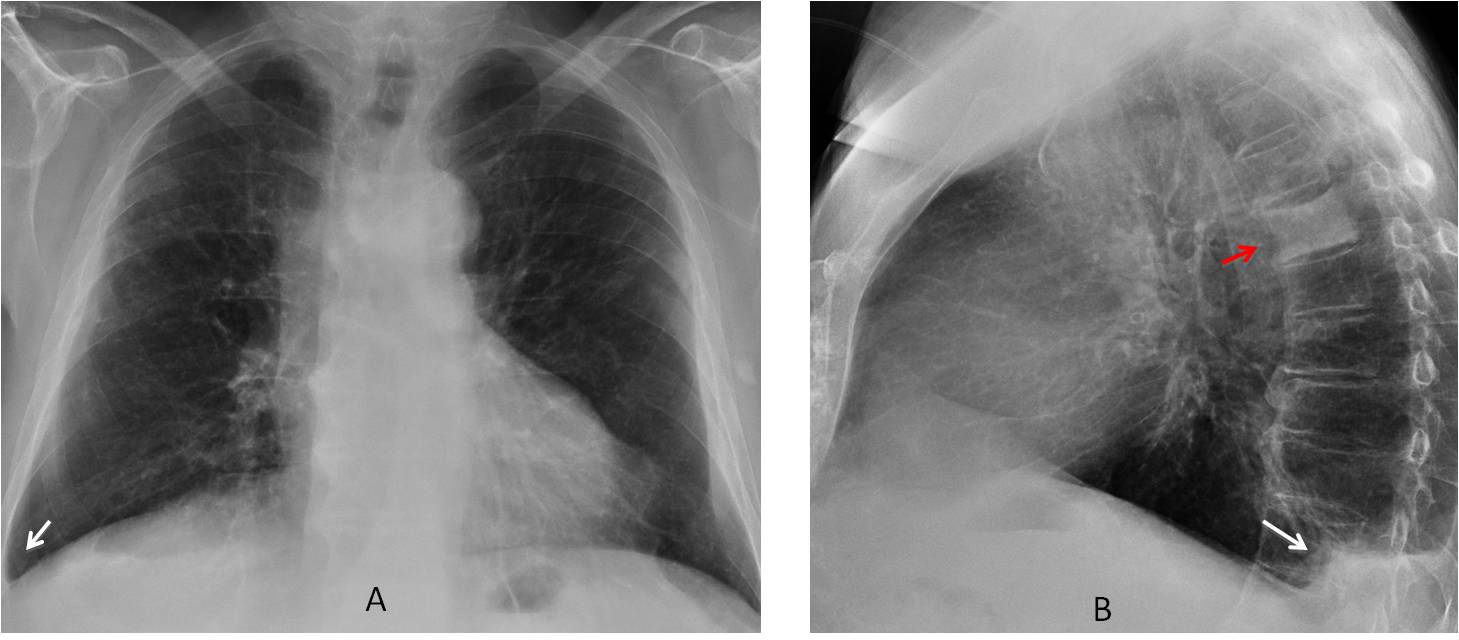
Fig. 1
Fig. 1. 78-year-old man with back pain. PA view shows a small right pleural effusion (A, arrow). Lateral view confirms the effusion (B, white arrow) and shows an ivory vertebra (B, red arrow), unsuspected in the PA view. Diagnosis: metastasis from prostate carcinoma
The sternum is also hidden by the mediastinum in the PA radiograph. Usually it is not well depicted in the lateral view, but it should always be examined because most conditions affecting the sternum are malignant. When sternal disease is suspected, it is imperative to obtain a CT (Fig. 2).
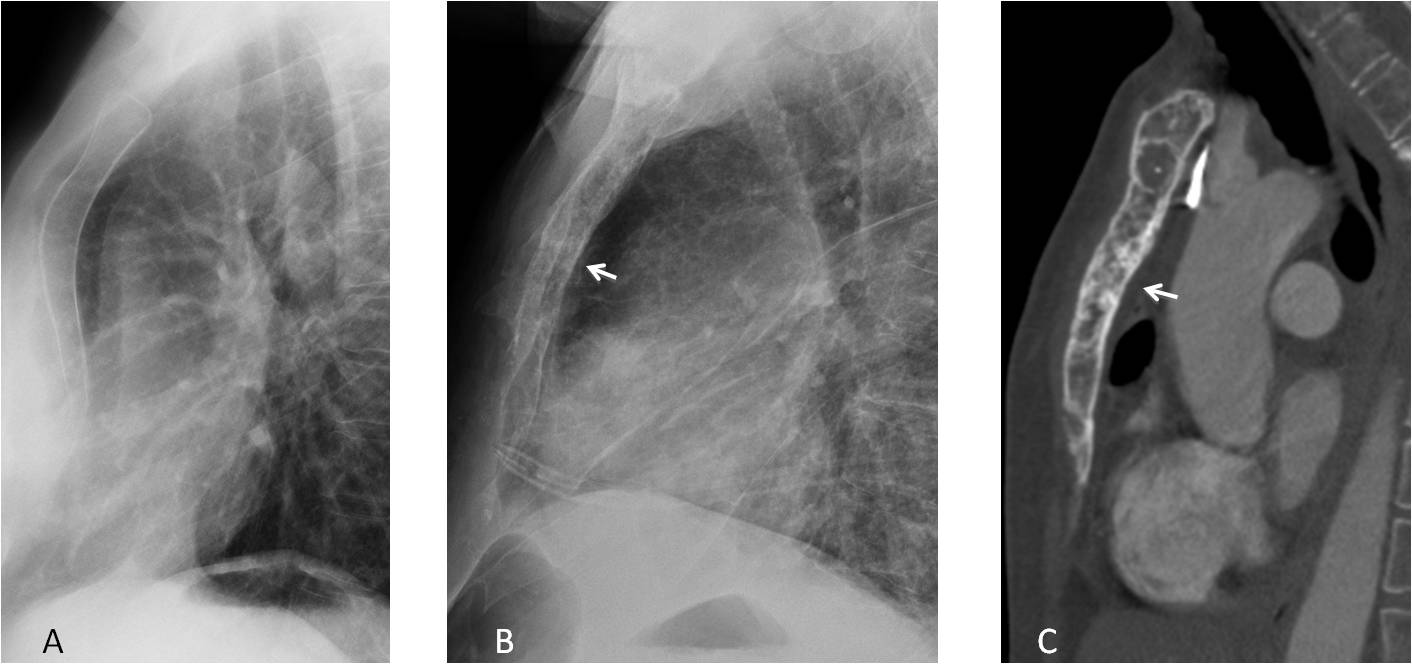
Fig. 2
Fig. 2. A) Lateral view showing a normal sternum. B) In a patient with breast carcinoma, the sternum shows a mottled density (arrow). Mixed metastases are confirmed on the sagittal CT image (C, arrow).
Diseases of the middle mediastinum may only be visible in the lateral view. The following areas should be examined: in the upper region, the trachea and Raider triangle, a radiolucent area that lies between the posterior wall of the trachea, the aortic arch and the spine (Fig. 3A), and in the central mediastinal region, the hilar area (Fig. 3B). The lower region (retrocardiac space) was covered in Diploma case 100.
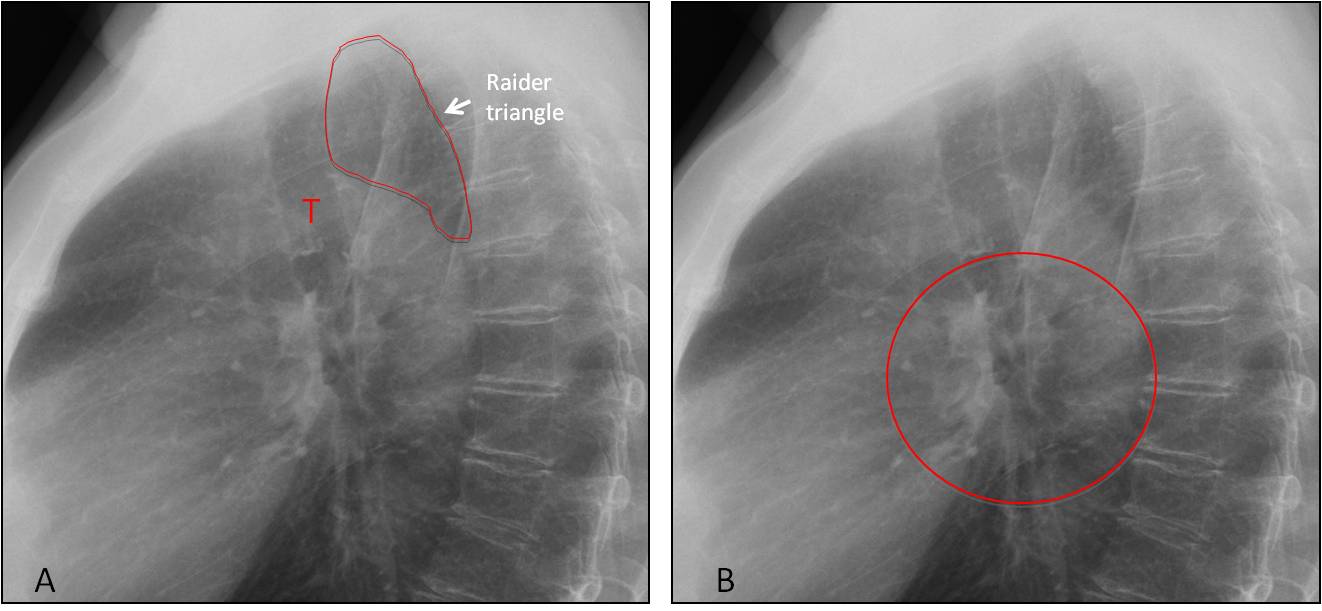
Fig. 3
Fig. 3. A) The trachea (T) is well visualised in most lateral views. The radiolucency of the Raider triangle is similar to that of the anterior clear space. In B, the circle delineates the hilar area in the central middle mediastinum.
Tracheal displacement is an excellent indicator of conditions affecting the upper middle mediastinum. Endothoracic goiter, enlarged lymph nodes and esophageal and vascular diseases are the most common etiologies (Fig. 4)
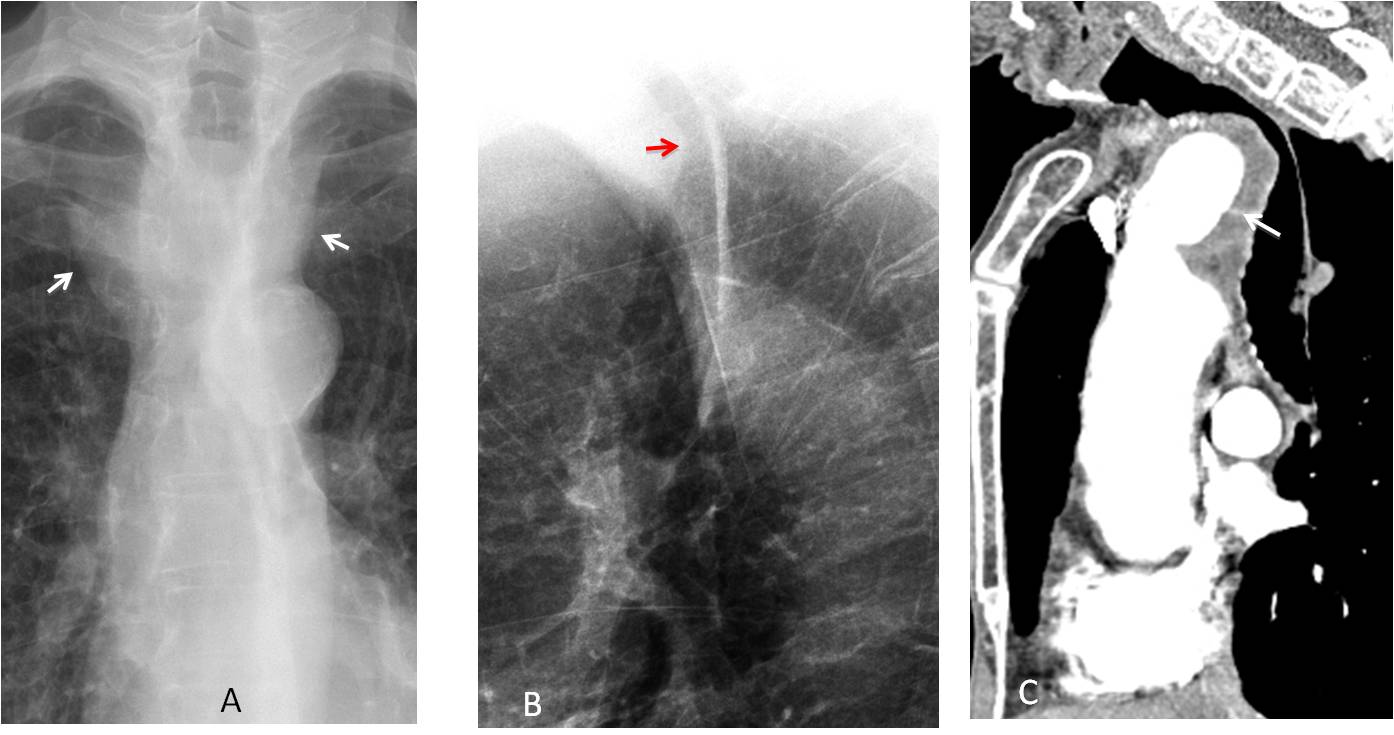
Fig. 4
Fig. 4. 69-year-old man with dyspnoea. PA radiograph shows tortuosity of the supra-aortic vessels (A, arrows). There is marked narrowing of the trachea in the lateral view (B, arrow), suggestive of an anterior mediastinal mass. Sagittal enhanced CT shows an aneurysm of the innominate artery (C, arrow) compressing the trachea.
Opacification of the Raider triangle should always be investigated. The most common cause is esophageal disease (Fig. 5), followed by congenital malformations of the aortic arch.
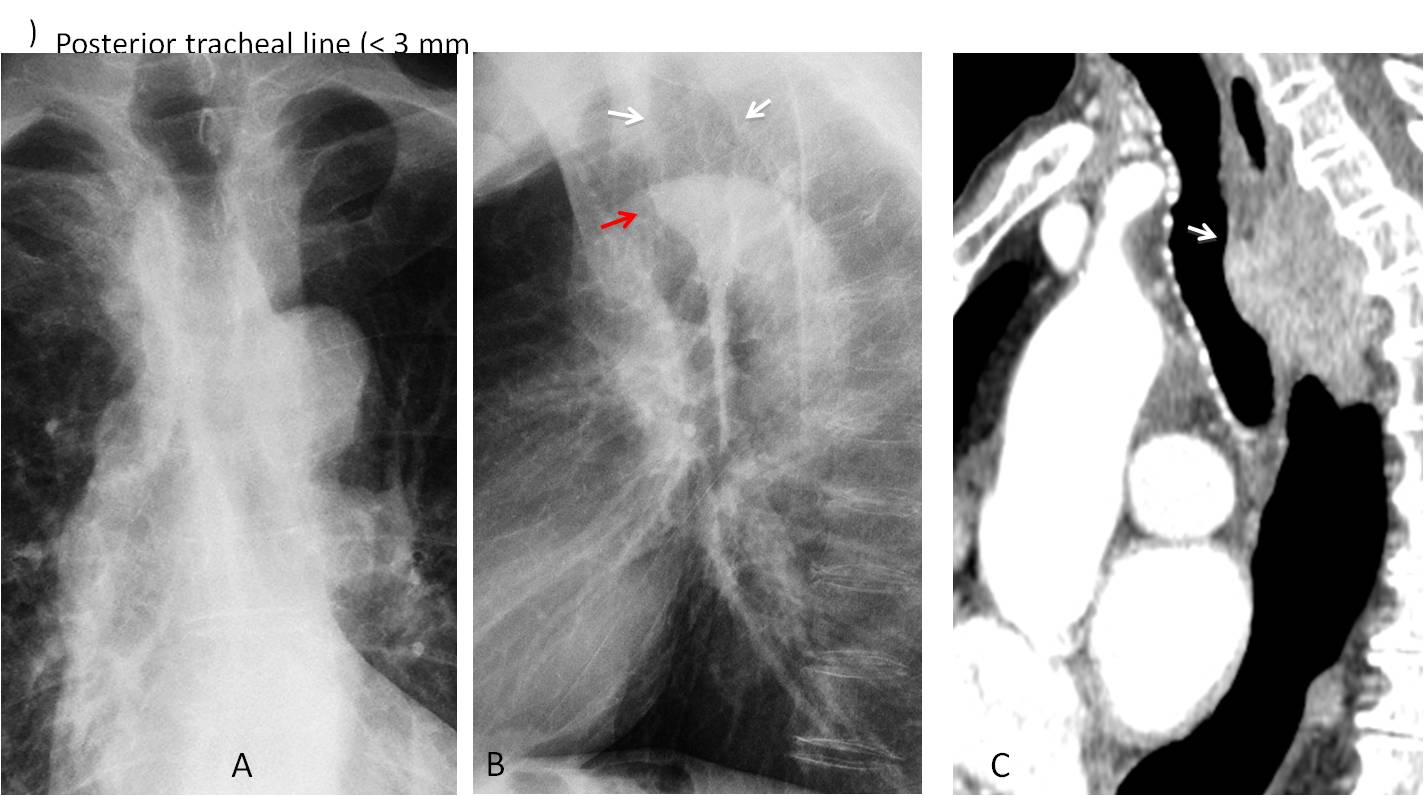
Fig. 5
Fig. 5. 65-year-old man with dysphagia. PA chest film (A) is unremarkable except for a saber-sheath trachea. The lateral film shows that the Raider triangle is opacified (B, white arrows). Note the bulge in the posterior tracheal wall (B, red arrow). Sagittal CT shows a large mass behind the trachea, occupying the Raider triangle (C, arrow). Esophageal carcinoma.
The central areas of the middle mediastinum is occupied by the hila. As we all know, the normal hila correspond to the right and left pulmonary arteries, clearly depicted in front and behind the tracheal plane in most lateral radiographs (Fig. 6).
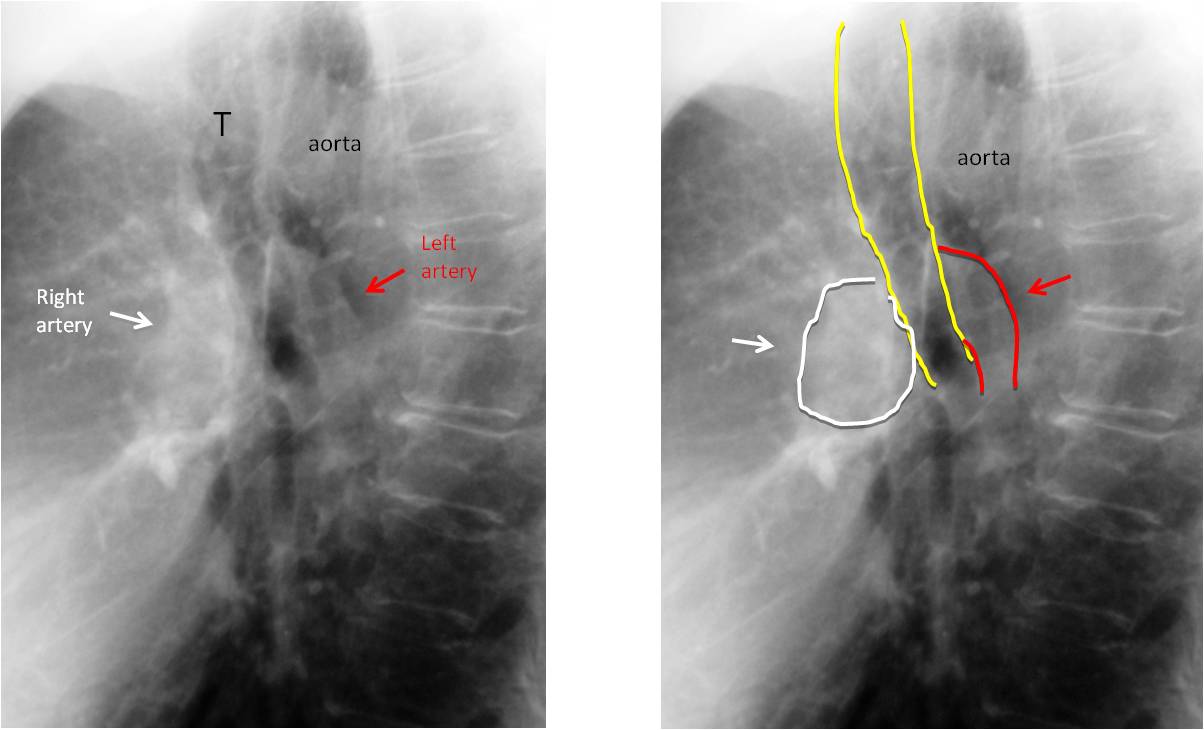
Fig. 6
Fig. 6. Normal anatomy of the hila in the lateral view. The right pulmonary artery is seen as a rounded shadow anterior to the trachea (A and B, white arrows). The left pulmonary artery is behind the trachea and has a comma shape (A and B, red arrows).
The lateral projection is highly useful to determine whether hilar enlargement is due to prominent arteries or enlarged lymph nodes (Fig. 7).
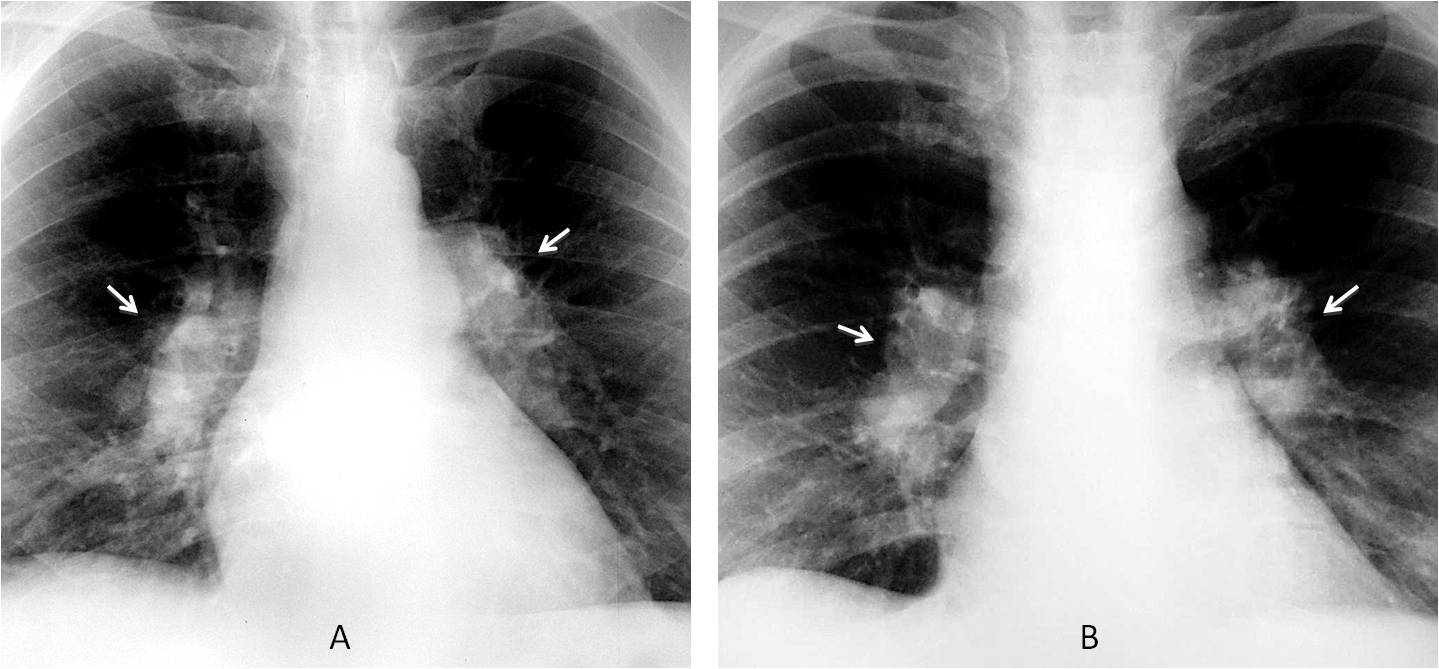
Fig. 7
Fig. 7. Two different patients with prominent hilar shadows in the PA view (A and B, arrows). In this view it is difficult to determine whether or not the cause is secondary to enlarged pulmonary arteries or lymphadenopathy.
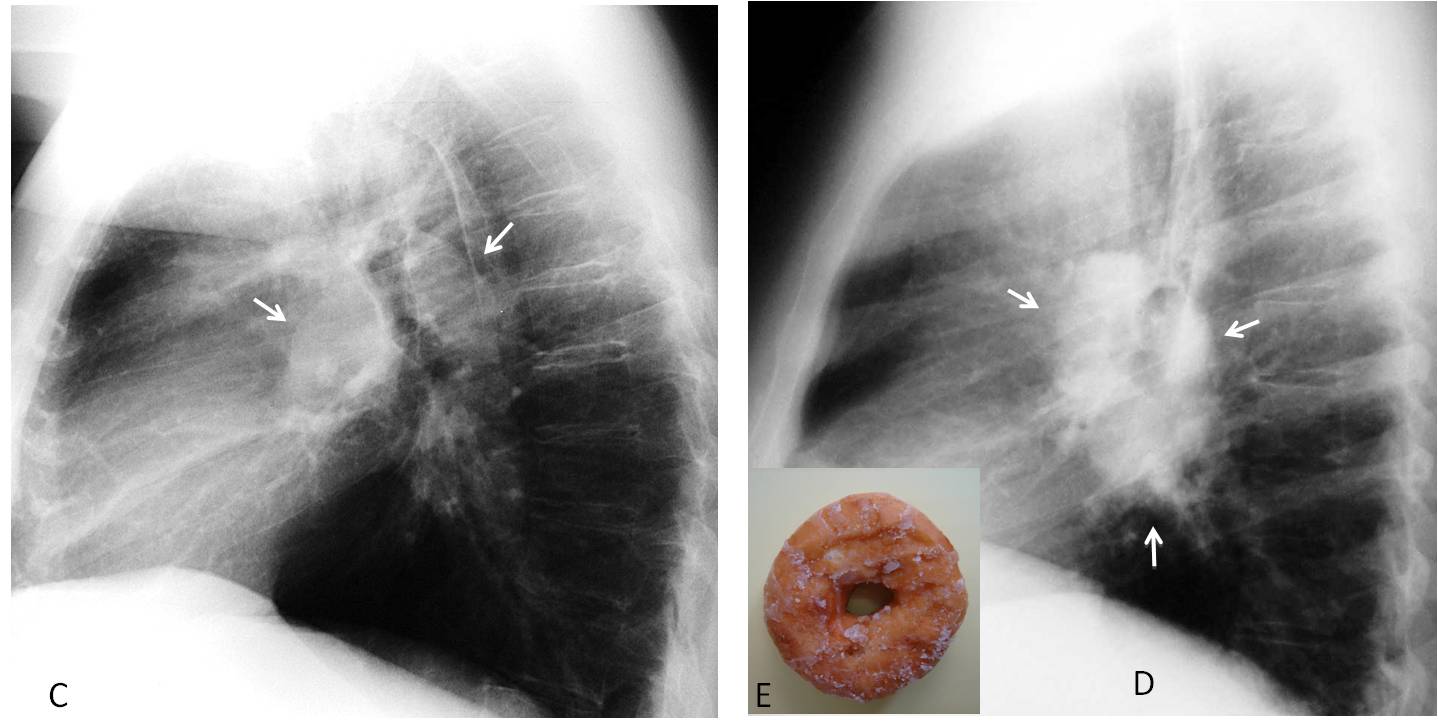
Lateral view of patient A shows enlargement of both pulmonary arteries (C, arrows) secondary to pulmonary hypertension. The lateral view of patient B shows an opacity encircling the upper lobe bronchus (D, arrows), which is known as the donut sign (E, insert) and is characteristic of lymphadenopathy. Diagnosis: lymphoma
Congenital duplication cyst is a common condition in the central region of the middle mediastinum. The PA view is often unremarkable (Fig. 8).
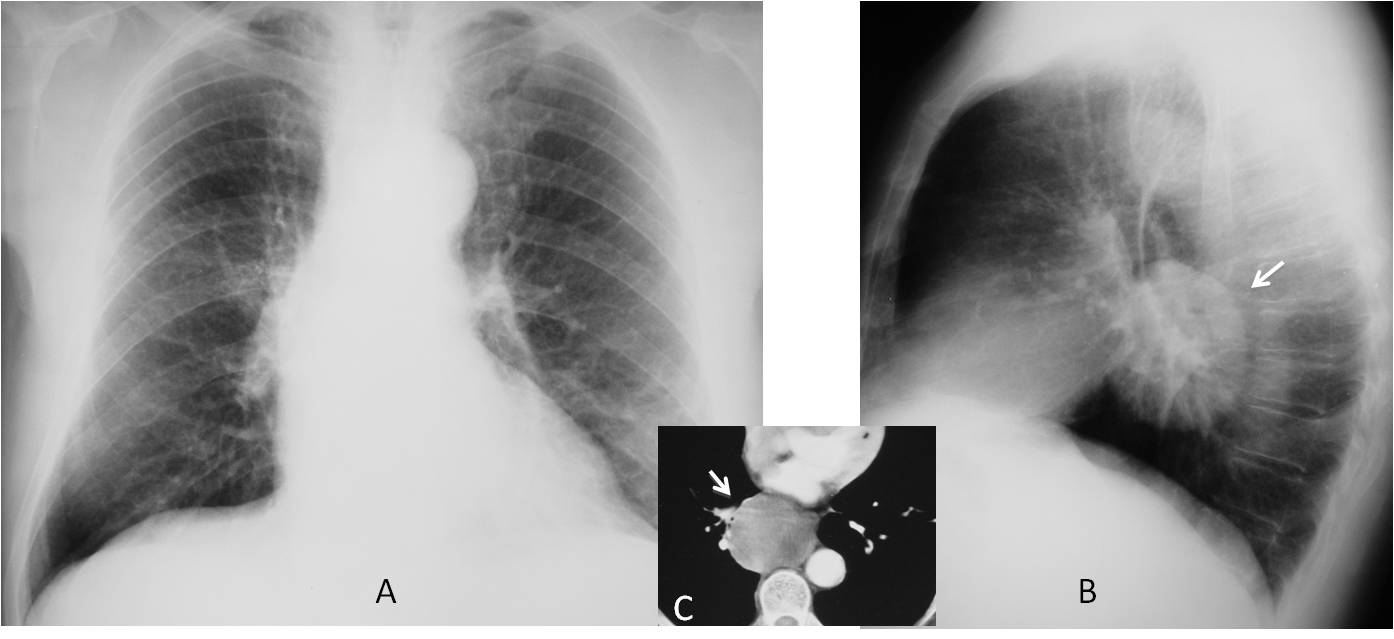
Fig. 8
Fig. 8. 56-year-old man with cough. PA radiograph (A) is unremarkable. Lateral view shows a well-defined rounded mass in the central area of the middle mediastinum (B, arrow). Axial CT shows a non-enhancing mass (C, arrow), confirmed to be a duplication cyst.
To finalise the checklist, we have to examine the cardiac shadow, particularly seeking cardiac or pericardial calcifications that are not seen in the PA view (Figs. 9 and 10) and pericardial effusion (Fig. 11).
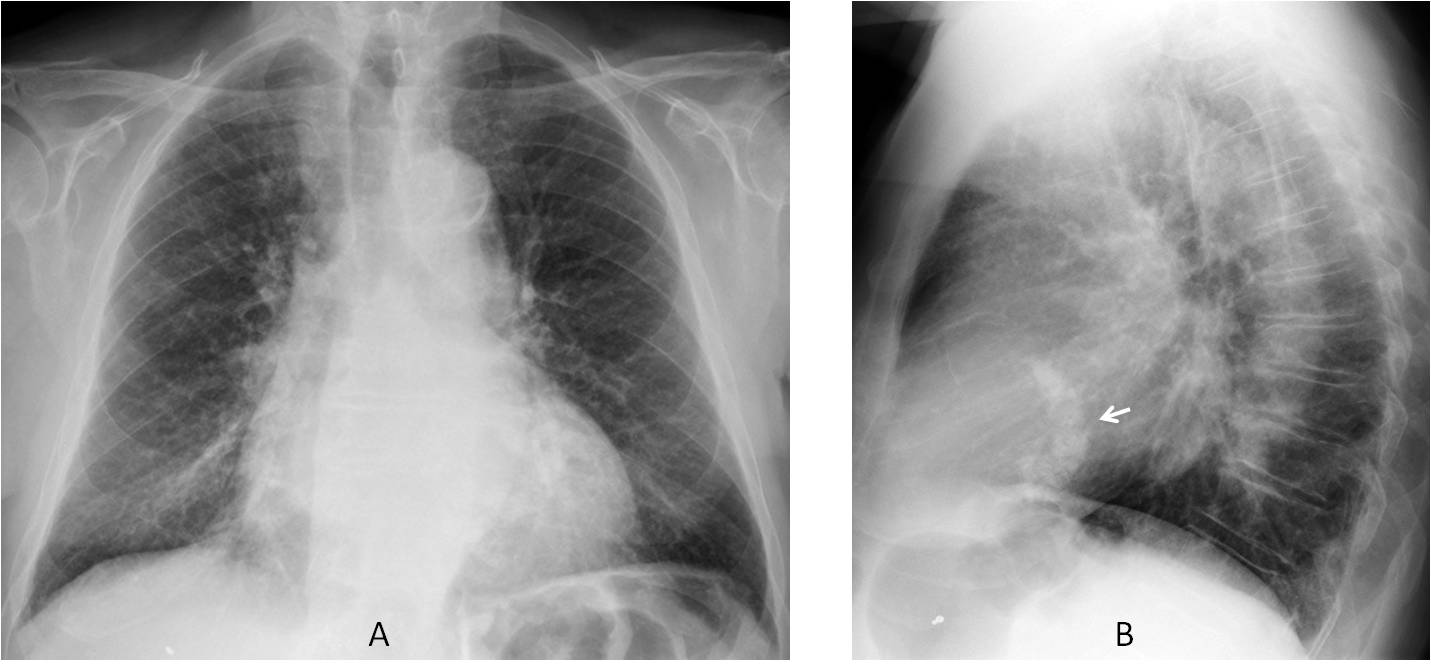
Fig. 9
Fig. 9. 72-year-old man with dyspnoea. PA radiograph (A) shows discrete cardiac enlargement. Lateral view dipicts a typical reversed C-shaped calcification of the mitral annulus (B, arrow). This is not uncommon in the elderly population and is usually symptomless.
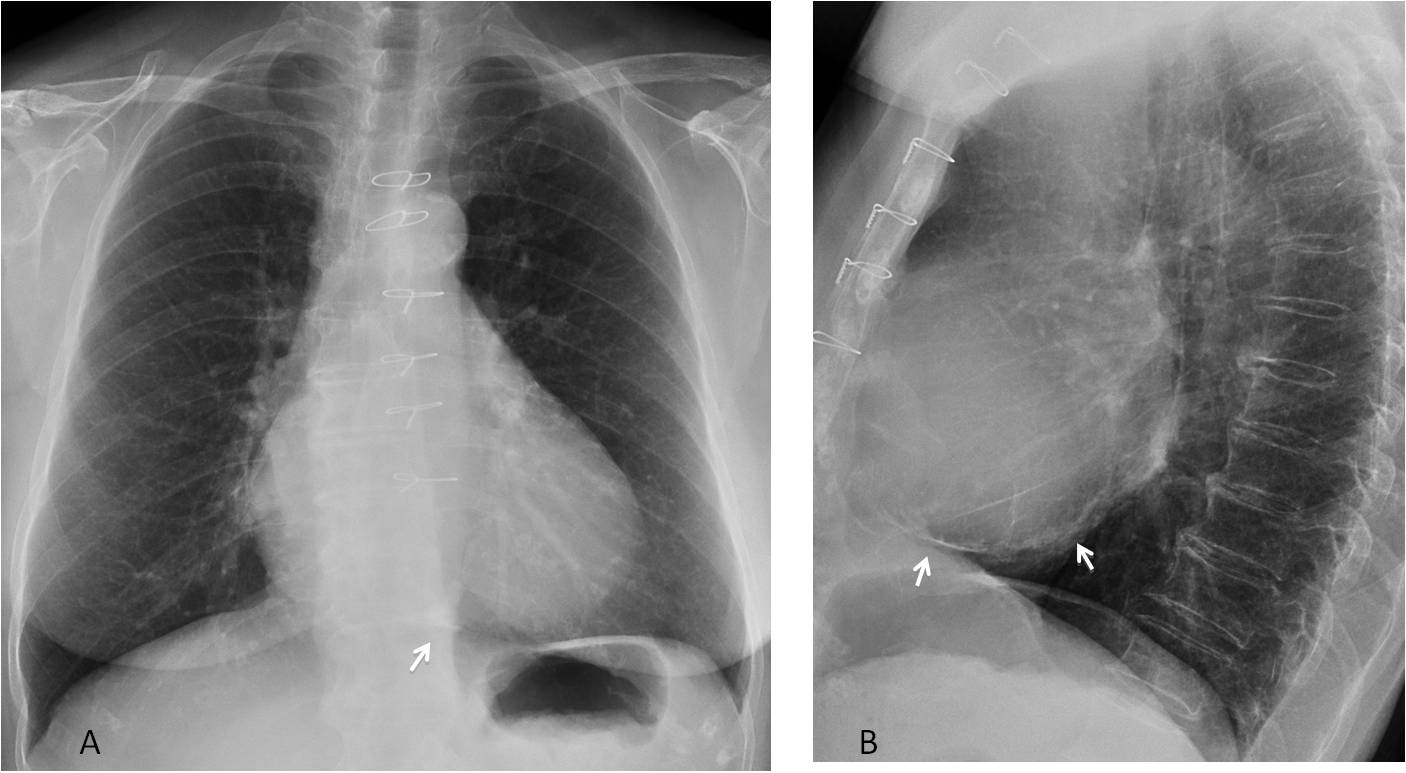
Fig. 10
Fig. 10. 58-year-old woman with a pericardial calcification after cardiac surgery. The calcium is barely visible in the PA view (A, arrow), but is obvious in the lateral projection (B, arrows).
In patients with an enlarged cardiac silhouette in the PA radiograph, we should always look at the anterior area of the heart shadow in the lateral view. In my experience, detection of displacement of the epicardial fat (pericardial fat stripe sign) is a reliable indicator to suspect pericardial effusion/thickening, which should be confirmed by echocardiography (Fig. 11).
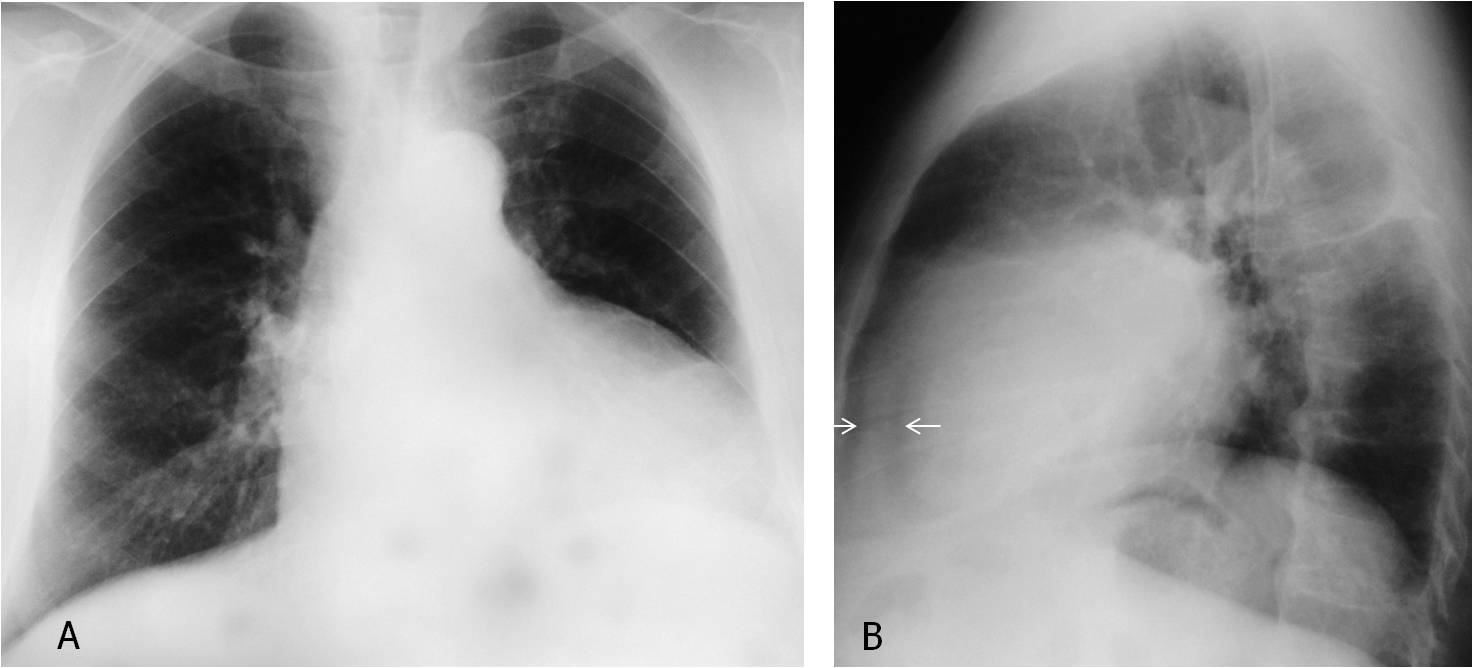
Fig. 11
Fig. 11. 53-year-old man with pericardial effusion simulating cardiomegaly in the PA view (A). The diagnosis is suspected in the lateral view because of the thickened pericardial stripe between the epicardial and mediastinal fat (B, arrows).
Cone-down lateral view taken three months earlier shows a normal pericardial stripe (C, arrows). Compare with the present film (D, arrows). Sagittal CT confirms the presence of a large pericardial effusion (E, arrows).
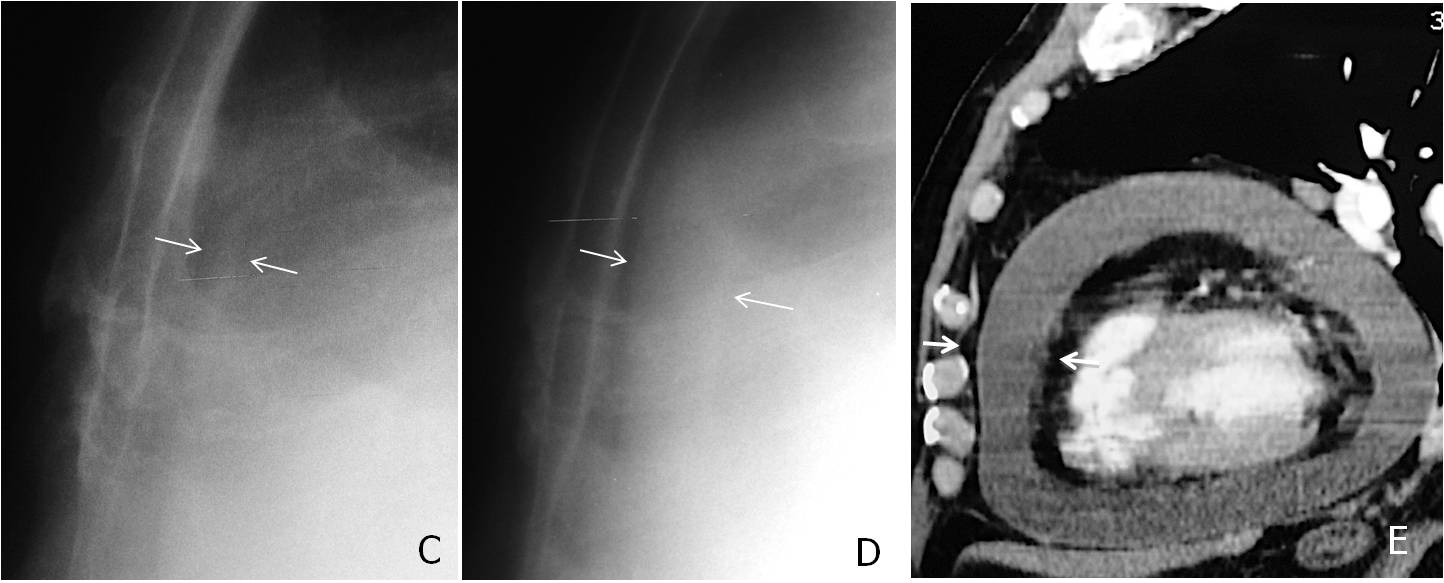
Fig. 11
In conclusion, the following areas should be investigated in the lateral view:
The spine and sternum, to detect conditions that are not visible in the PA radiograph
The upper middle mediastinum, to discover tracheal displacement or Raider triangle opacification
The hila, to confirm disease and to differentiate between enlarged arteries and lymphadenopathy
The heart shadow, to detect cardiac and pericardial calcifications and an enlarged pericardial stripe

Follow Dr. Pepe’s advice:
In the lateral chest radiograph look for:
1. Disease of the spine or sternum
2. Tracheal displacement
3. Opacity of the Raider triangle
4. Donut sign
5. Cardiac/pericardial calcifications and thickened pericardial stripe


The lateral view shows a high density lesion proyected over the vertebral body with an anterior well defined margin (posterior mediastinum). I cant find it in the PA view. I think it correspond to a vertebral lesion.
In the PA view the trachea is slighly displaced to the right side.
In older persons it is normal to have the trachea displaced to the right by the elongated aorta
The PA view shows an tubular infracarinal lucency which communicates with the carina,displacing the left main bronchus.this can also be seen on the lateral view, reaching the heart contour. Probably a subcarinal air cyst communicating with the carina.
Sclerotic lesion of Th vertebral body, prostatic Ca meta?
Widening of the right upper mediastinum- right paratracheal, lymphadenopathy? Vascular structures? Retrosternal mass?
Sclerotic vertebra – given age concerning for metastasis most likely prostate (I would compare to old films and make sure not old and benign). The left main bronchus has a slightly vertical orientation and the left upper zone looks a more lucent compared to the right but I cannot see features of left lower lobe collapse so I’d ignore this and just call vertebral lesion and suggest bone scan / PSA level.
….il polmone di sx è iperlucente, , da patologia del bronco lobare che appare improntato anteriormente e leggermente dislocato posteriormente( ?)…l’ilo vascolare mi sembra ipoplasico….anomalia vascolare ? Comunque vada è bello sfidarti !
Lateral view shows rounded opacity projected over a mid thoracic vertebra
Likely represents pleural bases posterior pulmonary mass.
It’s not clearly seen on PA view
In lateral and AP view in the left lung there is density lesion.
Thank You Dr.Pepe