Dr. Pepe’s Diploma Casebook: Case 25 – SOLVED!
Dear Friends,
This week I’m presenting the case of a 9-year-old child with pain in the leg after trauma.
Diagnosis:
1. Aneurysmal bone cyst
2. Simple bone cyst
3. Giant-cell tumour
4. Osteosarcoma

9-year-old child with pain in the leg after trauma
Findings: well-delimited, expansive intraosseous lytic lesion at the proximal peroneal diaphysis. Thinning of the periosteum and multiple internal septations (black arrows). Periosteal reaction at the distal end (white arrows).

Fig. 1
Magnetic resonance shows the expansive intraosseous lesion with multiple small cavities (Fig. 2, black arrows). There is a larger cavity (Fig. 2, asterisk) with a fluid-fluid level (Fig. 3&4 red arrows), cortical thinning, and periosteal reaction (Fig. 4, yellow arrows). No soft tissue lesions are seen.
Diagnosis: Aneurysmal bone cyst.
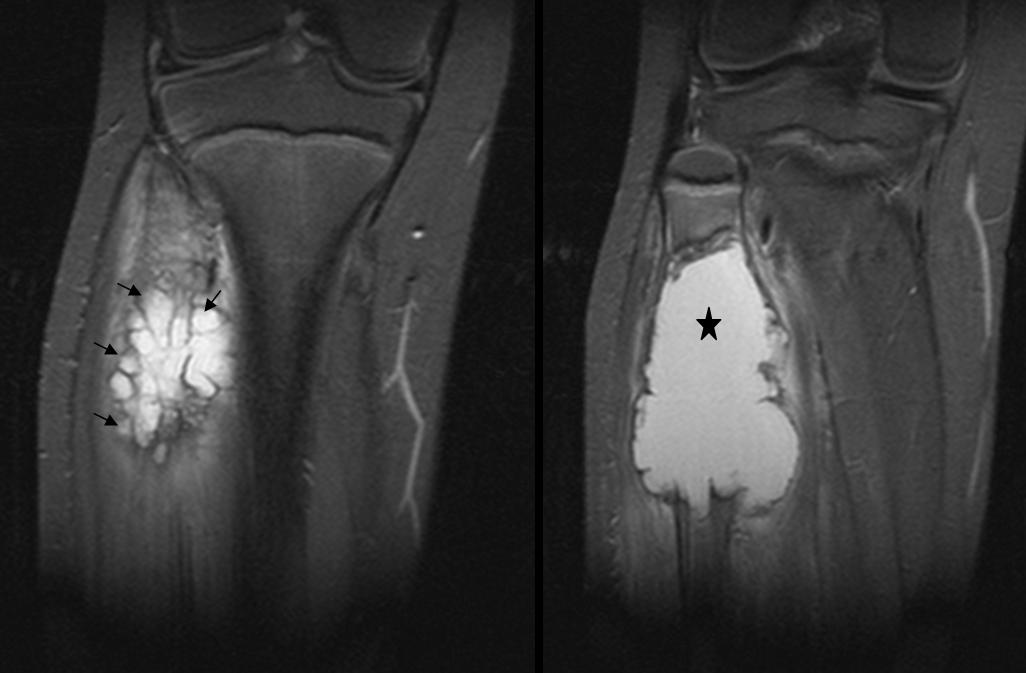
Fig. 2
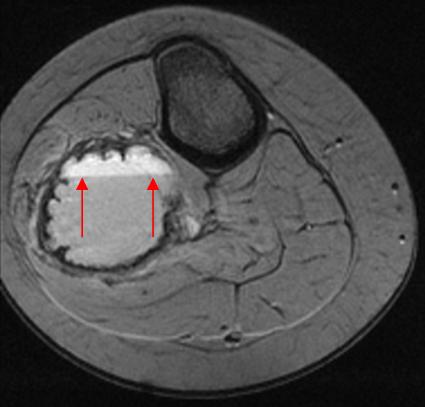
Fig. 3
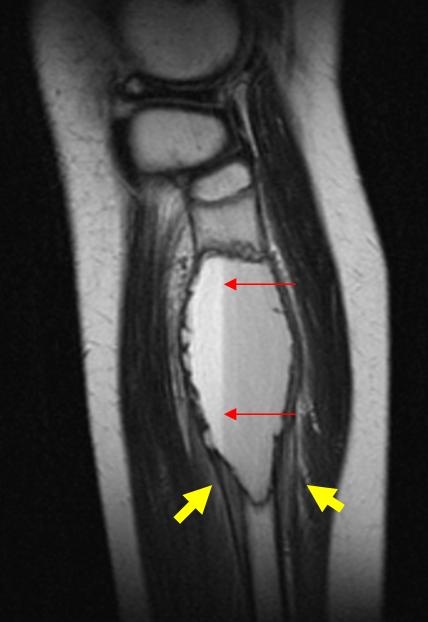
Fig. 4
Aneurysmal bone cyst, a common condition in children and adolescents, is characterised by the presence of large cavities filled with haematic material. It is usually identified incidentally following a trauma, or in studies investigating pain or increased bone volume. Aneurysmal bone cyst usually occurs in the long bones, although any bone of the organism can be affected. The most commonly affected flat bone is the pelvis. The size of the mass varies considerably from 2 to 20cm.
The radiologic appearance of long bone involvement is characteristic: well-delimited lytic area in the metaphysis with fine internal septations, cortical thinning, and bone expansion. There may be periosteal reaction and cortical rupture (pathologic fracture). The margin of the lesion is usually sharp and sclerotic. The radiologic features in flat bone involvement can simulate aggressive disease. On CT and MRI, fluid-fluid levels are often seen in the cavities. The soft tissues are seldom affected. In cases of pathologic fracture, there may be oedema of the soft tissues.
The etiopathogenesis of aneurysmal bone cyst is unknown. There is some debate regarding whether it is a radiologic and pathologic entity or the result of changes induced by a pre-existing lesion.
Simple bone cyst is a tumour-like lesion of unknown etiology, usually presenting as a well-defined, central lytic lesion of the metaphysis located adjacent to the epiphysis (Fig. 5, arrows). Any bone can be affected, but it most commonly occurs in the long bones, with 60% to 80% of cases involving the femur and humerus. The size of the cyst ranges from 2 to 15cm. The lesion may increase in length as the patient grows, but it never extends toward the adjacent epiphysis; hence, the growth cartilage remains intact. Pathologic fractures are common and when they occur, pain ensues. If there is no associated fracture, these lesions are usually asymptomatic.
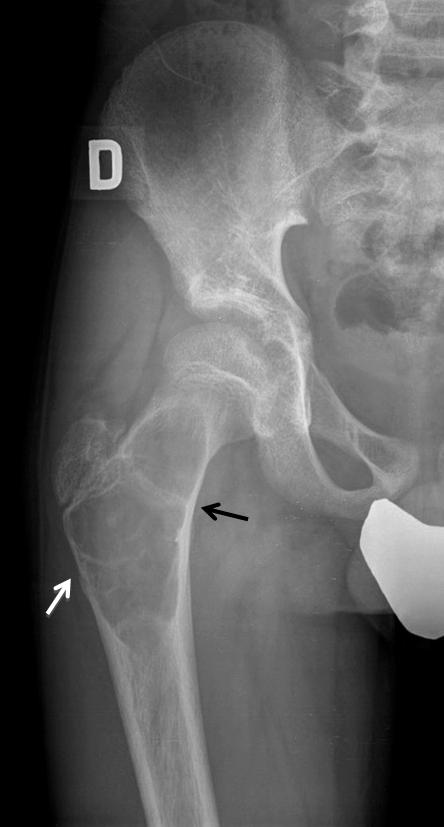
Fig. 5
Giant cell tumour is an epiphyseal bone tumour that affects patients when the growth cartilage has already fused. Most cases occur between the ages of 20 and 50 years; they are rare in children. The lesion mainly affects the long bones of the extremities (70-90% of cases), as well as the spine and pelvis. Giant cell tumour is usually a single lesion, 2 to 20cm in size. On radiographic study, it is seen as an expansive, lytic, epiphyseal lesion that extends to the subchondral bone, with well-defined borders, but no sclerosis (Fig. 6, arrows).

Fig. 6
The differential diagnosis with aneurysmal bone cyst is based on the age at presentation and the location of the tumour within the bone. Aneurysmal bone cyst rarely affects the epiphysis and occurs when the growth cartilage still persists. Giant cell tumour affects the epiphyses of mature skeletons.
Conventional osteosarcoma is usually an extensive lesion with an aggressive radiologic appearance, including bone destruction, poorly defined margins, cortical rupture, and soft tissue invasion. One variant of this tumour, telangiectatic osteosarcoma (less than 5% of osteosarcomas) presents cystic areas of necrotic or haemorrhagic nature. On MRI, the lesion may show blood-filled cavities with an internal fluid-fluid level that can mimic aneurysmal bone cyst. The presence of periosteal reaction and soft tissue invasion (Fig. 7, arrows) helps to differentiate between these conditions.

Fig. 7

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Aneurysmal bone cyst appears as an expansive, lytic metaphyseal lesion in children.
- The characteristic MR findings are expansive lesion with cavities and internal fluid-fluid levels.
- Consider other conditions if the epiphyses have already fused or there is invasion of the soft tissues.
Suggested reading:
- Aneurysmal bone cyst: Value of MR imaging and conventional radiography. Eur Radiol 13:1118-24,2003.
- Imaging features of subperiosteal aneurysmal bone cyst. Acta Radiol 43:336-9, 2002.


aneurysmal bone cyst
aneurysmal bone cyst or telagiectatic osteosarcoma
Lytic insuflating multiseptated epi-metaphyseal lesion in a 9y.o child. My initial though would be an aneurismal bone cyst (primary or secondary to a Giant Cell Tumor or even a Chondroblastoma). The fact that the metaphysis is still open makes GCT of bone very unlikely; although chondroblastoma could associate aneursimal bone component, it is quite rare and there is no evidence of chondroid matrix. The appearance does not go with Simple Bone Cyst. Two other diagnoses I think we should contemplate because of the age of the patient are the Brodie Abscess and the Eosinophilic Granuloma, the image does not favor any one of them. Other possibilities we can think of are the Fibrous Dysplasia, non-ossifying fibroma and more rare tumors like chondromyxoid fibroma; the appearance and location does not reminds me anyone of them.
Finally, there are two images features that makes me worry and go against the initial diagnostic of Aneurysmal Bone Cyst. It seems to be soft-tissue component and evidence of cortical reaction in the lower pole of the lesion.
With these two last features, I think you cannot stablish the benign diagnosis of an ABC and you should complete the study with an MRI with the suspicion of TELANGIECTATIC OSTEOSARCOMA.
Expansive lytic image with no break in the cortical proximal third of the fibula. Presents narrow transition zone and no periosteal reaction.
The findings on plain radiographs and age are suggestive of aneurysmal bone cyst
aneurysmal bone cyst
proximal fibular, lytic, expansile, bubbly meta-diaphyseal lesion, lucent matrix, in an unfused skeleton ; but the periosteal elevation and spiculated bony densities at the lower edge of the lesion are highly suspicious for a much more aggressive lesion than an ABC –
final diagnosis telengiectatic osteosarcoma.
Lesione litica che “espande” l’osso: si esclude pertanto il TGC che è litico puro, senza “insufflazione dell’osso. La cisti semplice la si esclude perchè si vedono “spiculature” distali segni di pattern di tipo infiltrativo.Una cisti aneurismatica dovrebbe avere setti interni ossei e dovrebbe avere margini lisci.Rimane una “varietà dell’osteosarcoma, in passato definito aneurisma “maligno” dell’osso che è l’OS emorragico o teleangectasico:La rm fa diagnosi mostrando il segnale paramagnetico tipico del sangue ed emosiderina.
Giant cell tumor
Although giant cel tumor may occur in children, should not be your first choice if epiphysis are open.
an expansile lytic bone lesion at the proximal end of the fibula (meta-diaphyseal)with no cortical distruction and narrow zone of transition.not extentending to the articular surface, with evidence of internal septation, picture suggestive of aneurysmal bone cyst
Giant cell tumour