Dr. Pepe’s Diploma Casebook: Case 36 – SOLVED!
Dear friends,
Presenting liver MR images of a 63-year-old diabetic woman with mild pain in the RUQ over the last few weeks.
Possible diagnoses:
1. Hepatocellular carcinoma
2. Hepatocellular adenoma
3. Liver angiomyolipoma
4. Liver metastases
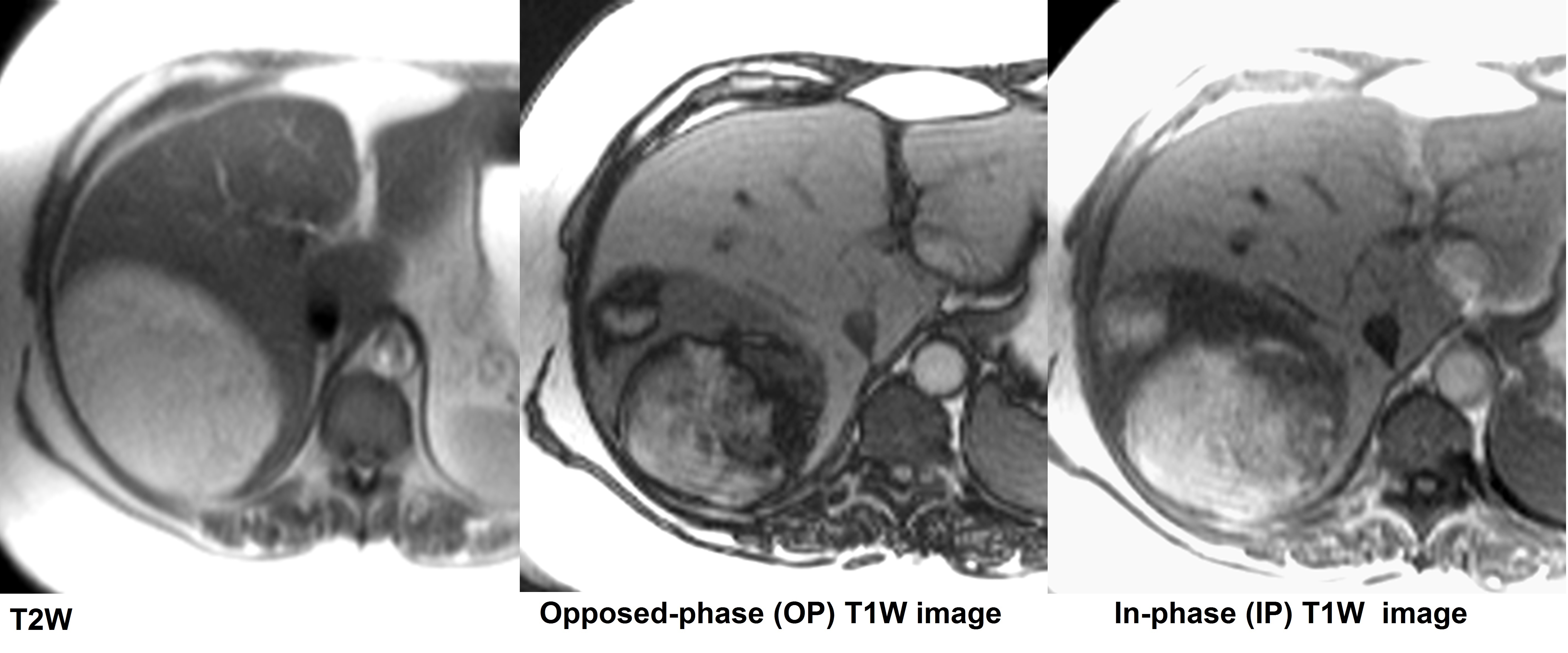
A 63 -year-old diabetic woman with mild abdominal pain in the right upper quadrant over the last few weeks
Click here for the answer to case #36
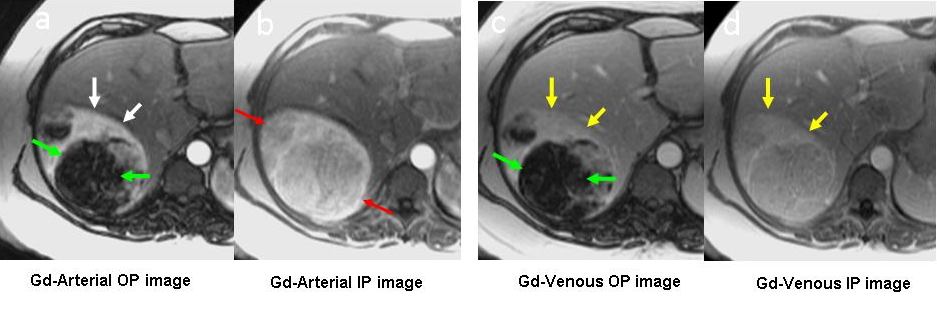
Imaging findings: (a-d) Enhanced arterial and venous chemical shift (OP-IP) images. The two parts of the tumour show different degrees of enhancement: the anterior part is highly hypervascular (black arrows), whereas the posterior fatty portion shows a paradoxical signal loss on the OP image relative to the unenhanced OP image (b in Figure 2) (green arrows). On IP imaging, the signal intensity of the soft tissue and fatty area are very similar (red arrows). (c,d) Note that the mass lacks a peripheral capsule (yellow arrows).
Hepatic angiomyolipoma (AML) is a rare, benign, unencapsulated mesenchymal tumour composed of a variable amount of mature adipose tissue, smooth muscle, and blood vessels. The imaging findings depend on the relative proportions of tissue components within the tumour.
One of the most characteristic findings of AML is the presence of a fatty component. Liver AML should be differentiated from other fat-containing tumours, including hepatocellular carcinoma (HCC) and liver adenoma (LA). It is important to know that the fatty tissue of AML corresponds to adipose tissue or mature fat, whereas in HCC and LA, it represents fat within the tumour cells, and therefore, is mixed with cytoplasmic water.
On MR studies, the fat in AML can be accurately demonstrated using chemical shift MR imaging (OP and IP images). This technique depicts the dark cancellation line between the fatty component of the tumour and the soft tissue of the liver parenchyma or adjacent soft tissue tumor. In tumours in which the fatty component is a mixture of fat and water, there is a signal intensity loss on OP images as compared to IP images, but no dark cancellation line is seen.
Another morphologic characteristic of AML is the lack of a tumour capsule, as in the present case. HCC and LA often show a peritumour capsule.
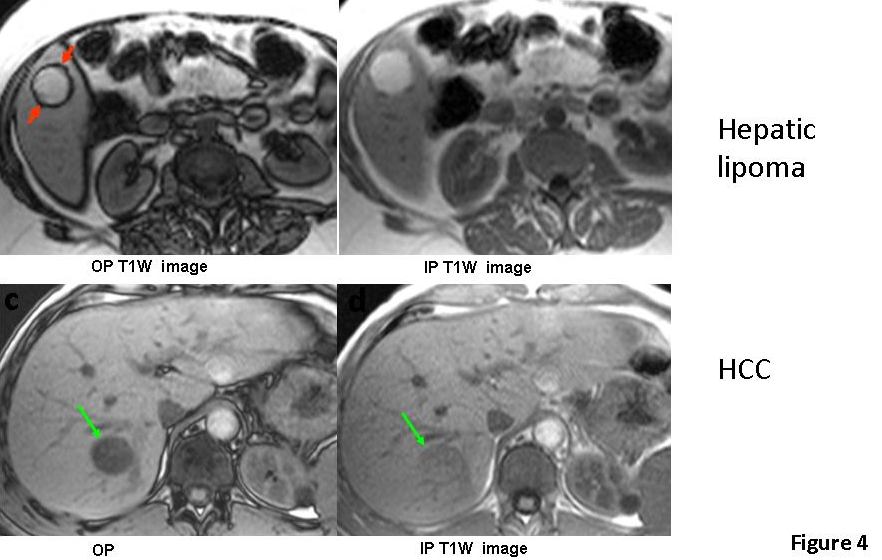
Differences in chemical shift MR (OP and IP) images between a tumor with mature fat, such as hepatic lipoma (a,b) and HCC with fatty metamorphosis (c,d). In the case of lipoma, signal intensity is similar on both OP and IP images, and a dark cancellation line between the tumor and liver is only seen on the OP image (red arrows in a). In HCC with fatty metamorphosis, a signal loss is seen on the OP image relative to the IP image, but there is no dark cancellation line (green arrows in c,d)
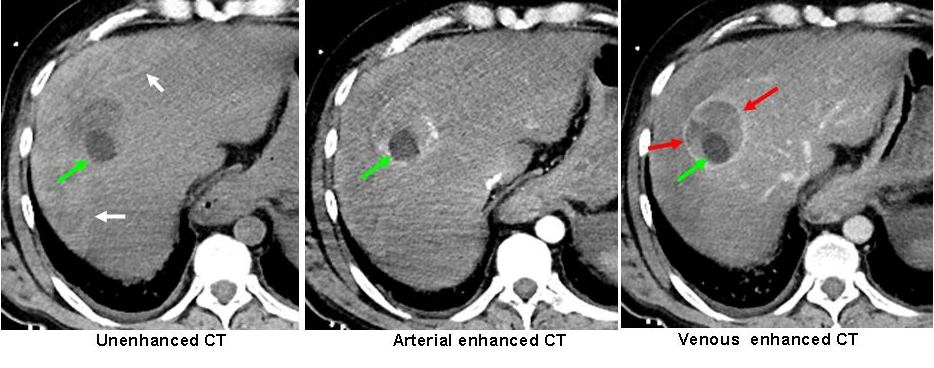
HCC with fatty metamorphosis and a complete peripheral capsule. (a-c) Unenhanced and enhanced CT show a liver tumour with a posterior rounded, fatty, nodular component (CT value, 23 HU) (green arrows) and a complete peripheral capsule, especially well-depicted in venous phase imaging (red arrows). In this patient, spontaneous rupture of the HCC occurred, with perihepatic bleeding (a, black arrows)
Follow Dr. Pepe’s advice:

MRI imaging techniques help differentiate AML of liver from other fat-containing hepatic tumours, such as HCC with fatty metamorphosis and liver adenoma.
On MRI, the pure fat of AML can be accurately confirmed with chemical-shift MR imaging (OP and IP), which shows a dark cancellation line between the tumour fat and tumour soft tissues or liver parenchyma, whereas the fatty component of HCC and LA is manifested by a signal intensity loss on OP images relative to IP images.
Liver AML lacks a tumour capsule. Other fatty tumours such as HCC with fatty metamorphosis and liver adenoma usually have one.
Kamimura K, Nomoto M et al. Hepatic Angiomyolipoma: Diagnostic Findings and management. Int J Hepatol. 2012;2012:410781
Prasad S, Wang H, Rosas H, et al. Fat-containing Lesions of the Liver: Radiologic-Pathologic Correlation. Radographics 2005;25:321-331
Case presented by Julio Martin, MD


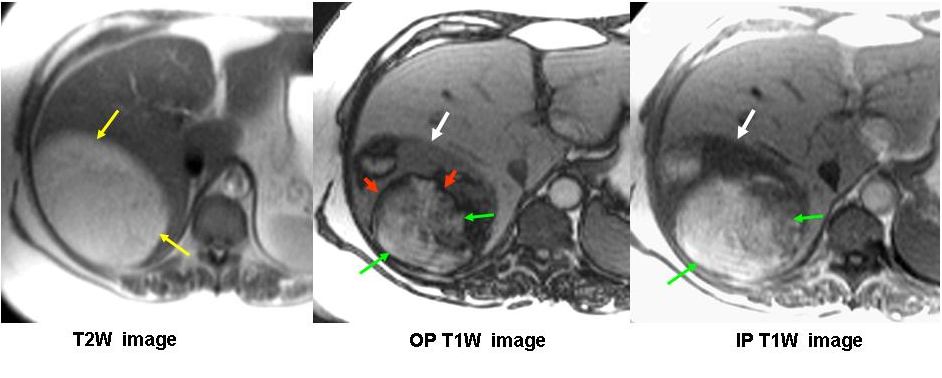
A large oval shape well defined outline focal lesion is seen at segment VII of the liver. It has high signal intensity at T1WI.
It posterior compartment shows different signal intensity between IP and OP; denoting fatty component.
with available MRI sequences ANGIOMYOLIPOMA is suggested.
However post Gd enhanced studies in arterial phase and subtraction IP-OP sequence is recommended to exclude malignancy.
Angiomiolipoma: Formazione spazio-occupante, a margini netti, senza capsula di delimitazione, disomogenea, per le diverse componenti tessutali, in OP ed IP.
Angiomyolipoma. It consists of macroscopic fat which does not show low signal on opposed phase image!
Loss of signal within the segment VI lesion on the out of phase T1WI suggests intracellular lipid, this is against hepatic angiomyolipoma. In a non-cirrhotic patient I would favor a hepatic adenoma, however a lipid containing HCC remains a possibility. Correlation with fat suppressed pre and post contrast imaging is needed to exclude macroscopic fat as a cause for the intrinsic T1 high signal, in which case an angiomyolipoma would be possible, although rare in the absence of tuberous sclerosis. In the presence of pain haemorrhage could also explain the intrinsic high T1 signal.
Hemangioma is a possibility. Simply because it contains fat and has high signal on T2.
A very, very remote possibility
Liver angiomyolipoma
….scusa dr Pepe ma al 2° segmento epatico è visibile un’altra immagine nodulare, iperintensa in IP:questo cambia tutta la diagnosi!!!!
Checked with Dr J Martin, who prepared the case. He congratulates you for your perception, but what seems a nodule is an artifact created by the aortic pulsation.
Well done!
The lesion contains macroscopic far and has heterogenous T1
Signal. This may represents an adenoma or angiomyolipoma.. Need intravenous contrast