Dr. Pepe’s Diploma Casebook: Case 48 – SOLVED!
Dear Friends,
This week I am presenting images of a 49-year-old woman with abdominal pain and moderate distension. Examine the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
What would be your diagnosis?
1. Hepatomegaly
2. Subpulmonary fluid
3. Diaphragmatic eventration
4. None of the above
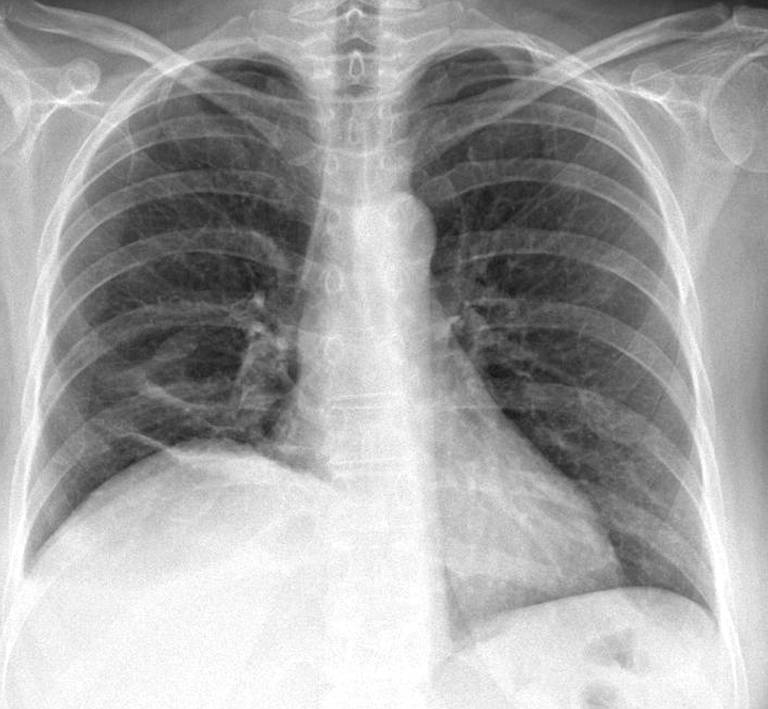
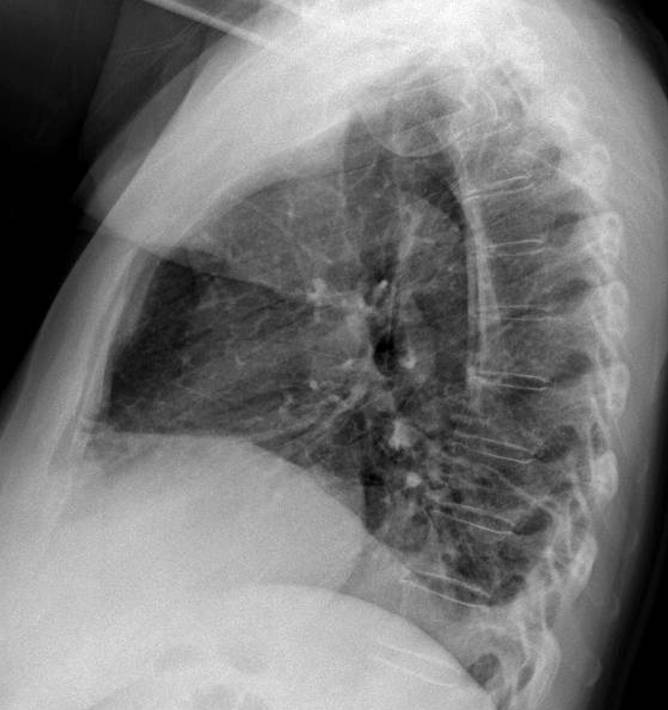
Findings: chest radiographs show an obvious elevation of the right hemidiaphragm, with blunting of the posterior costophrenic angle (B, arrow). There is also a small ovoid opacity in the right lower lung (A, arrow) and laminar atelectasis at the right lung base.
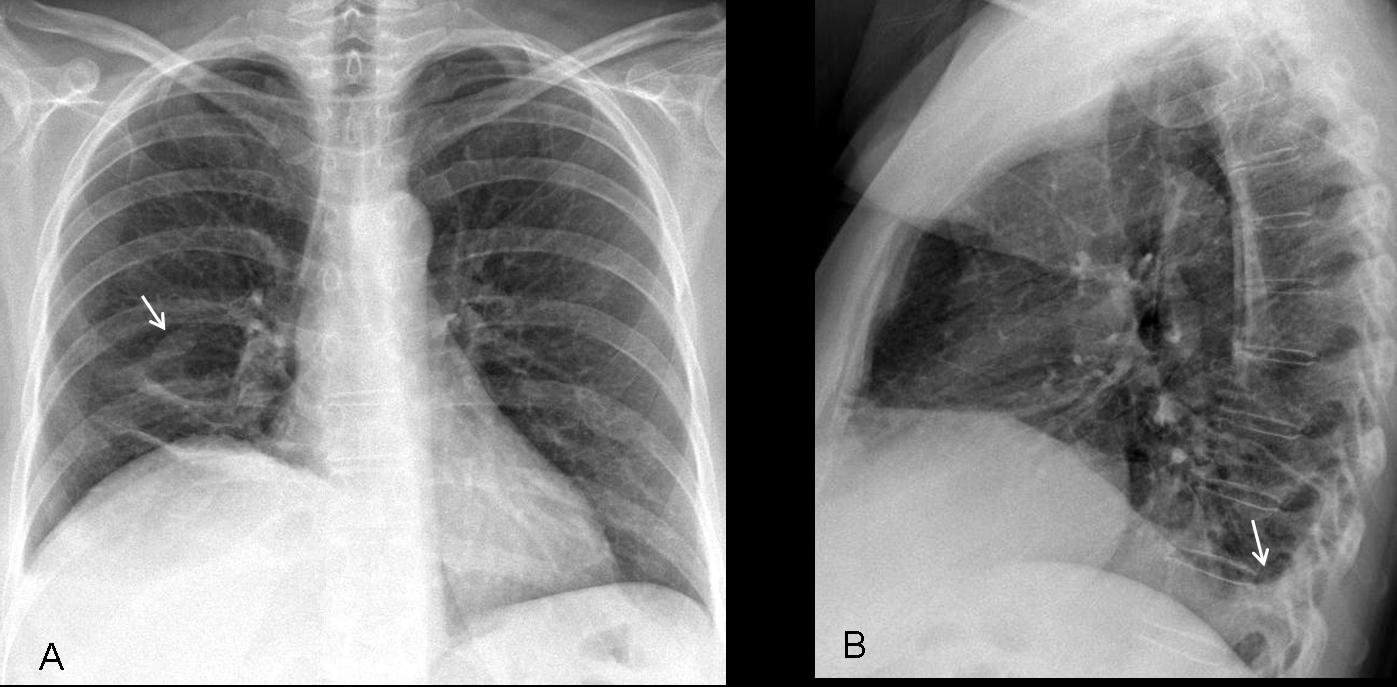
Fig. 1
Abdominal CT shows widespread ascitis, which is mass-like in the right subphrenic space (A, arrows). There is a small pleural effusion. The density of the ovoid lung lesion (B,C arrows) is similar to that of the masses in the subphrenic space.
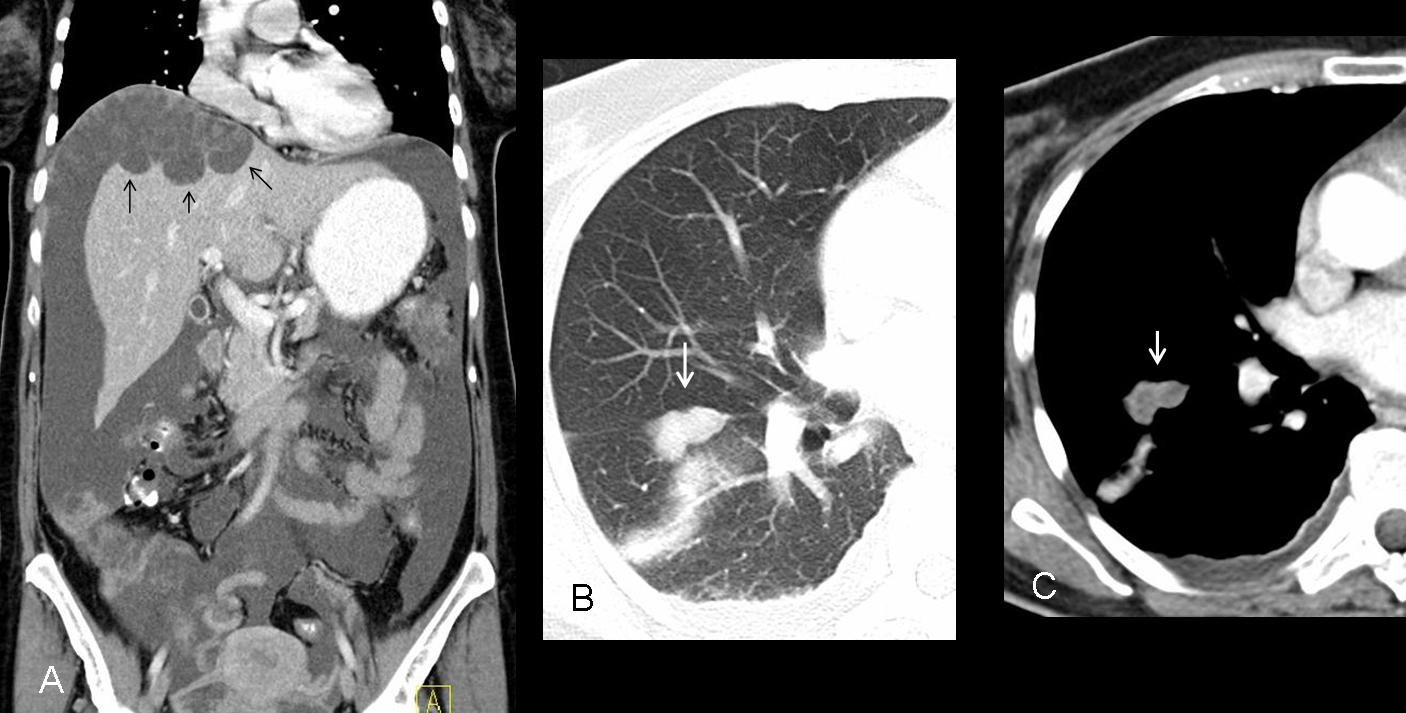
Fig. 2
Final diagnosis: ovarian carcinoma with pseudomyxoma peritonei and pulmonary metastases.
This case is presented to discuss the causes of elevated hemidiaphragm. Unilateral diaphragmatic elevation is not an uncommon finding, but in most cases, it is not clinically relevant. Nonetheless, it is sometimes a sign of a serious condition, as in the case shown.
In healthy individuals, the right hemidiaphragm is about 2cm higher than the left. Small differences in height should not cause concern, but obvious asymmetry deserves investigation.
The main causes of unilateral diaphragmatic elevation are:
1. Diseases of neighboring organs (chest and abdomen)
2. Diaphragmatic pathology (paralysis and eventration)
3. False elevations (subpulmonic fluid and hernias)
A common cause of diaphragmatic elevation is disease in neighboring organs.
The diaphragm is a frontier organ between the chest and the abdomen, and diseases in these anatomic areas may affect the position of the diaphragm. Any upper abdominal process (abscess, visceromegaly) may elevate the corresponding hemidiaphragm (Fig. 3). Similarly, any process causing a loss of lung volume (atelectasis, surgery), may pull the hemidiaphragm upward (Fig. 4).
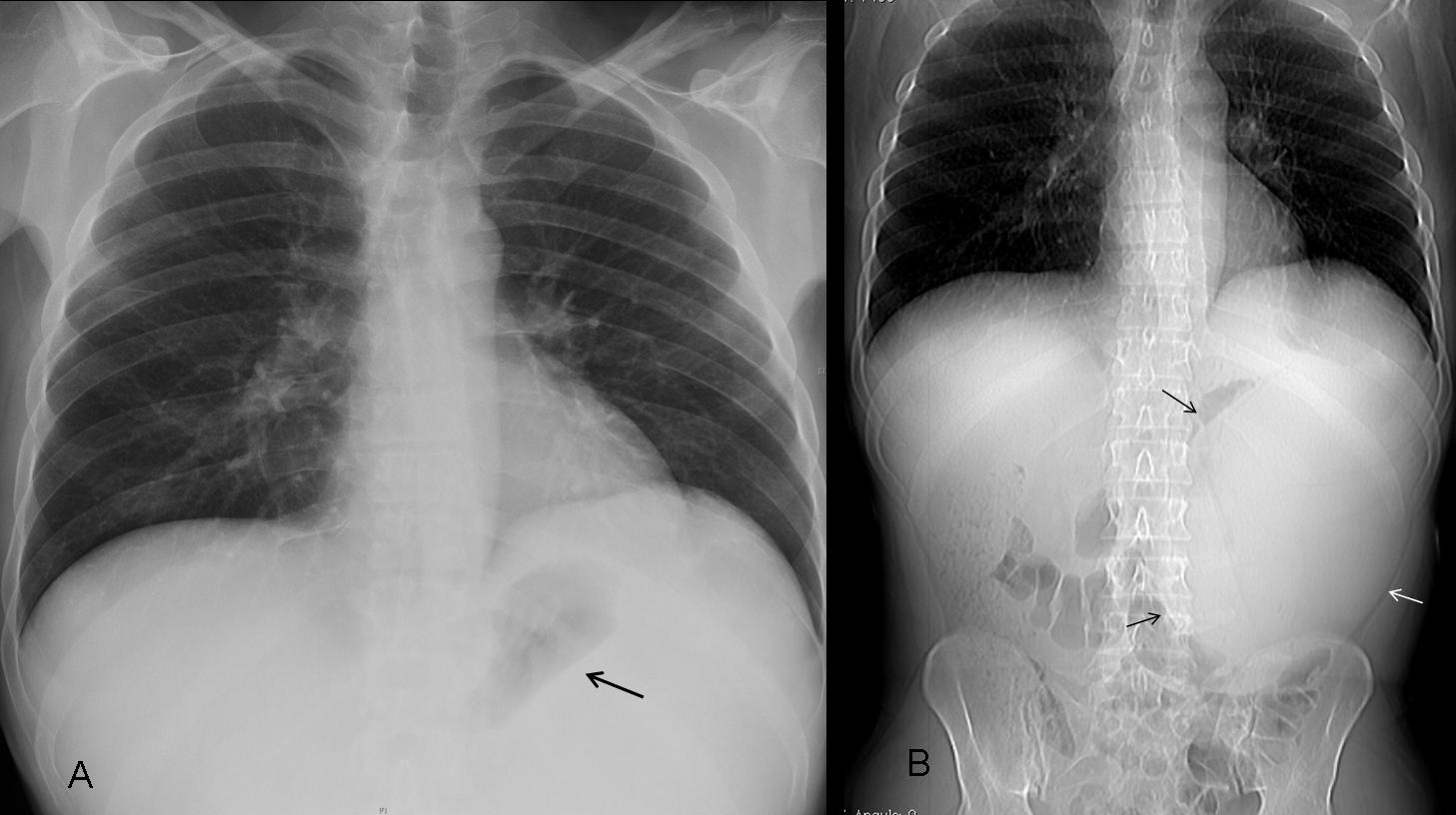
Fig. 3
Fig. 3 (aboove): elevated left hemidiaphragm secondary to marked splenomegaly. Notice the medial displacement of the gastric fornix (A, arrow) and the uniform opacity of the left upper quadrant. Abdominal film confirms the splenomegaly (B, arrows). Diagnosis: lymphoma.
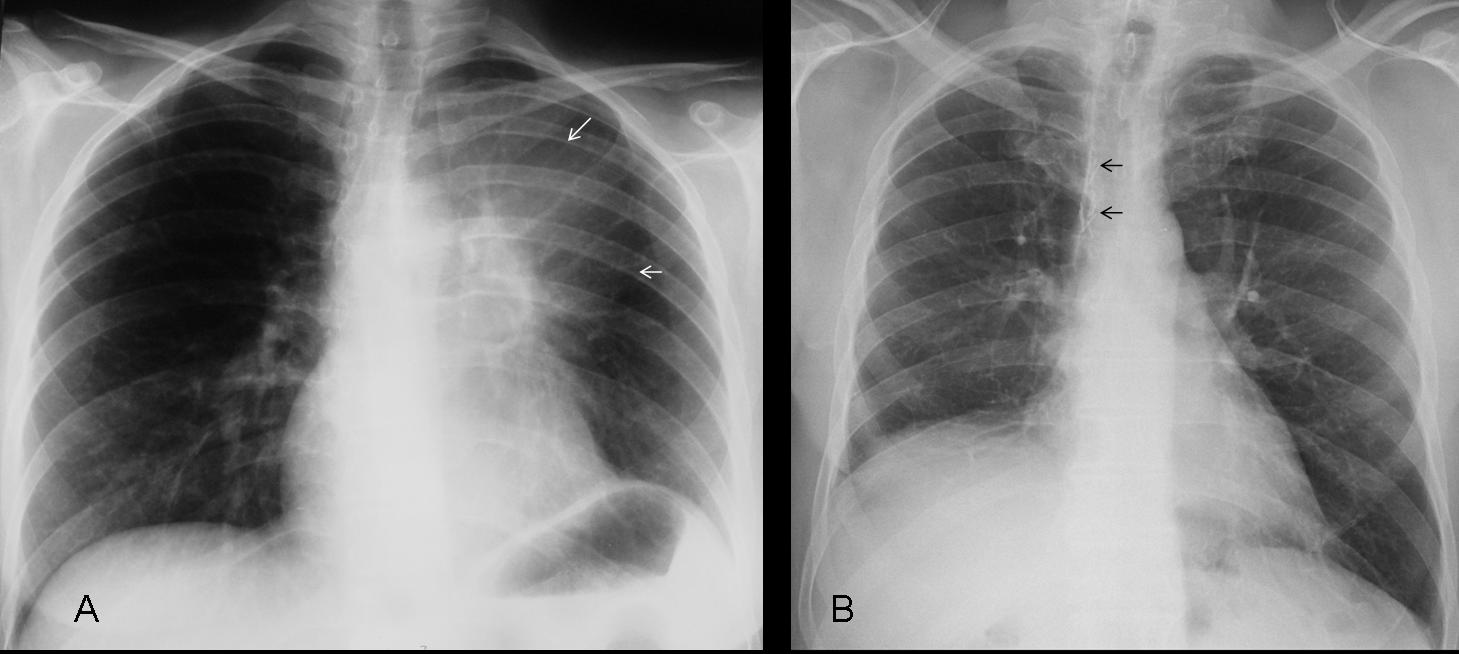
Fig. 4
Fig. 4 (above): elevation of hemidiaphragm due to loss of lung volume. Case A shows signs of LUL collapse (A, arrows). Case B corresponds to a RUL lobectomy. Post-surgical metallic sutures (B, arrows) may be overlooked if they are not carefully sought out.
Time for a test. Pre-op radiographs of a 27-year-old male undergoing urethral surgery. What would your diagnosis be?
1. Subpulmonic fluid
2. Diaphragmatic hernia
3. Diaphragmatic paralysis
4. None of the above
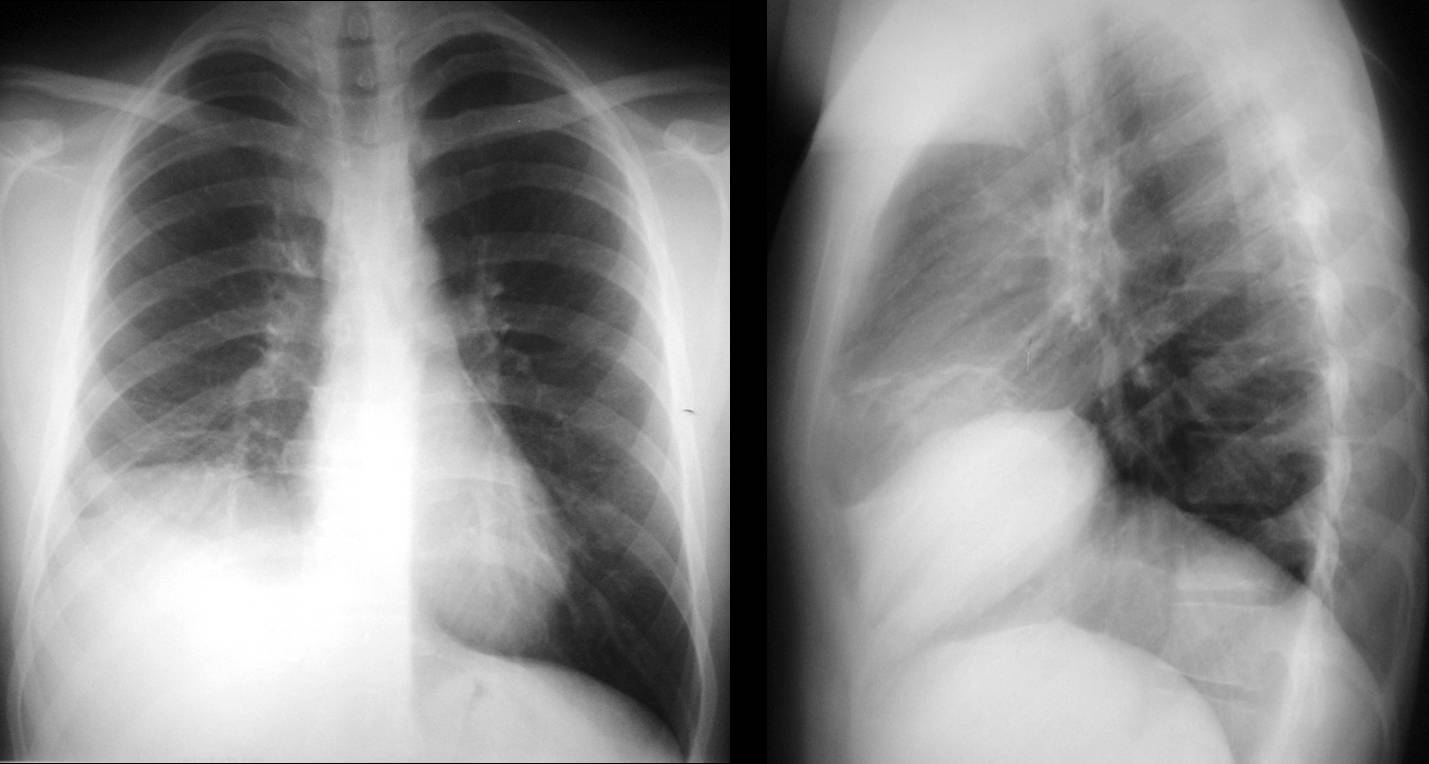
Fig. 5
Findings: Chest radiographs show an irregular elevated right hemidiaphragm, with obliteration of the costophrenic angle. Patient had ruptured his urethra in a motorcycle accident and additionally had a torn diaphragm with herniation of the liver, which was overlooked in this film.
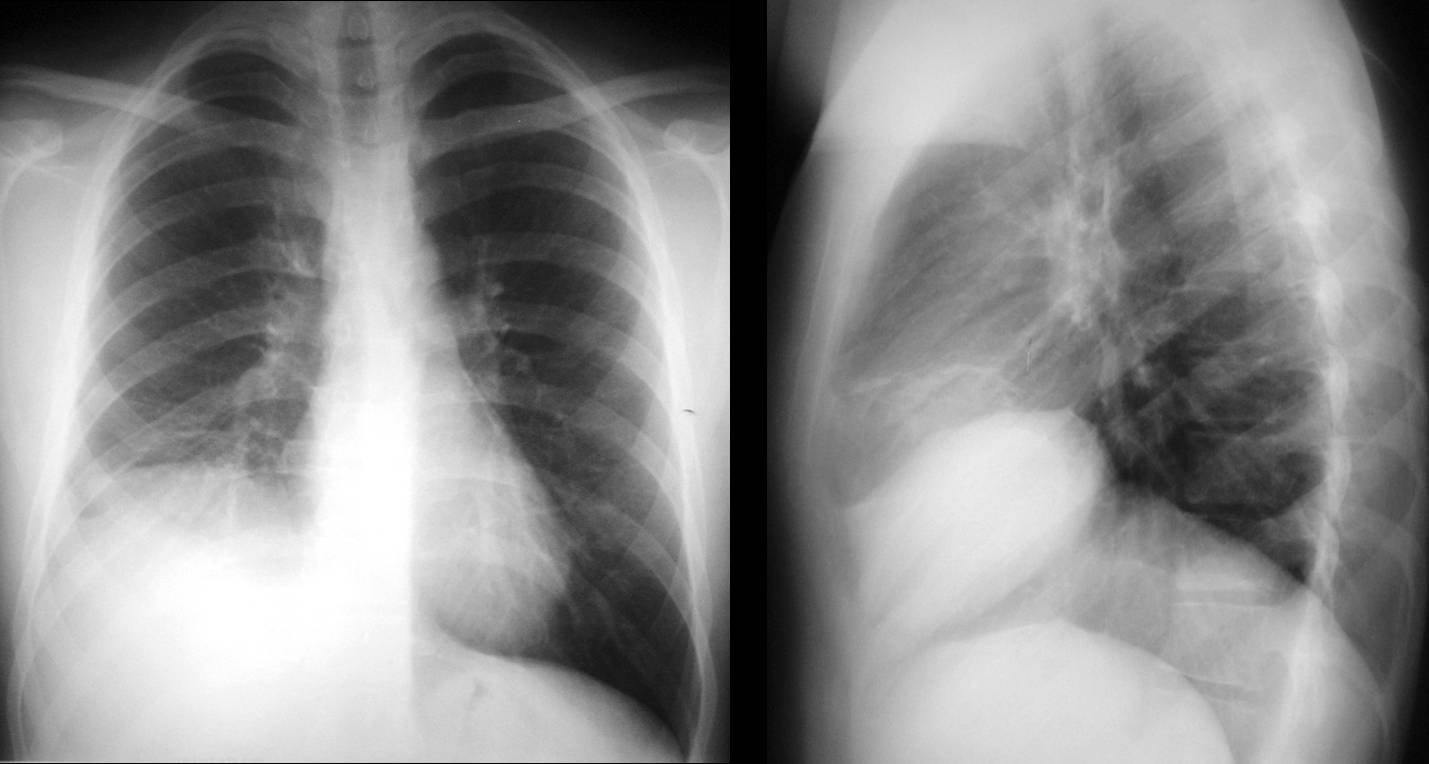
Fig. 6
Patient remained asymptomatic, and three years later the hernia is more obvious. Note the hepatic flexure of colon (A, arrow) marking the inferior border of the liver. Unenhanced CT at that time shows a large rent in the diaphragm (B, arrows), with most of the liver herniated into the chest.
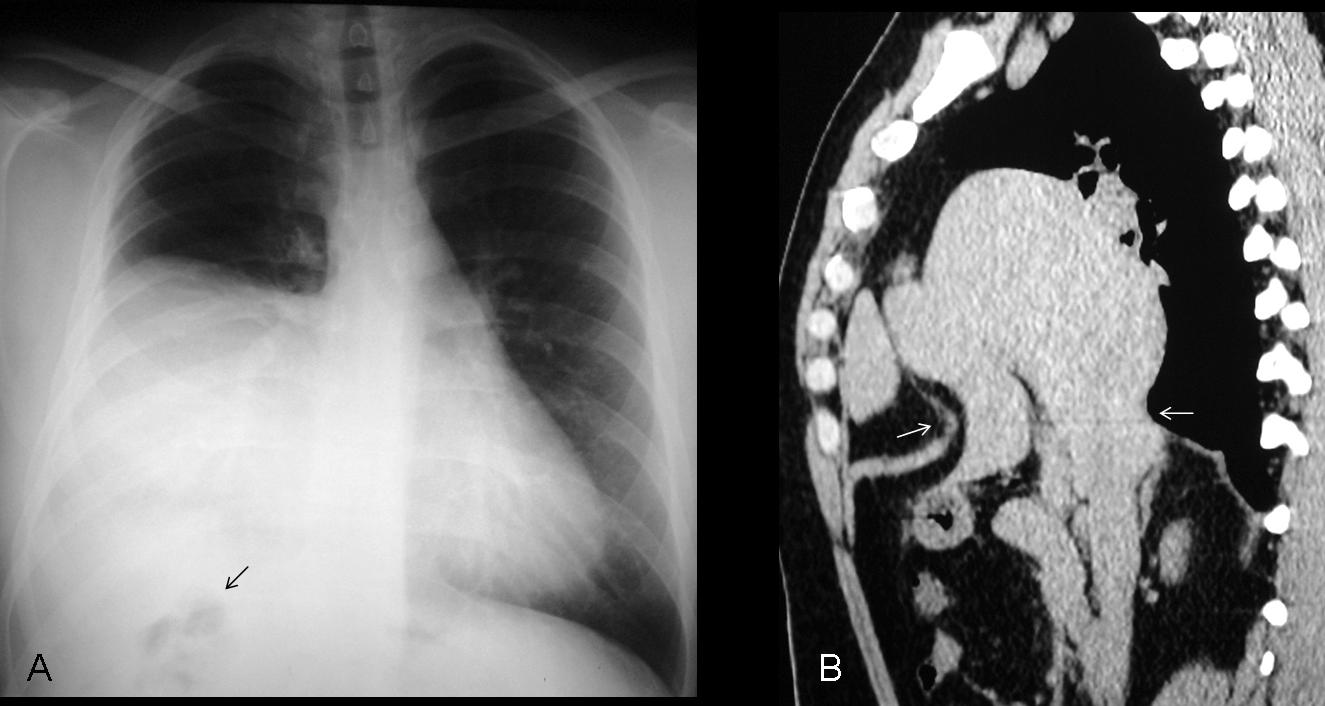
Fig. 7
Final diagnosis: traumatic diaphragmatic hernia, surgically proven.
Traumatic diaphragmatic hernias may be overlooked during the initial evaluation following trauma, being superseded by the most important pathology. The herniated viscera interpose between the diaphragm and the undersurface of the lung, simulating an elevated diaphragm. A history of significant trauma should alert us to perform a CT to exclude hernia (Fig. 8).
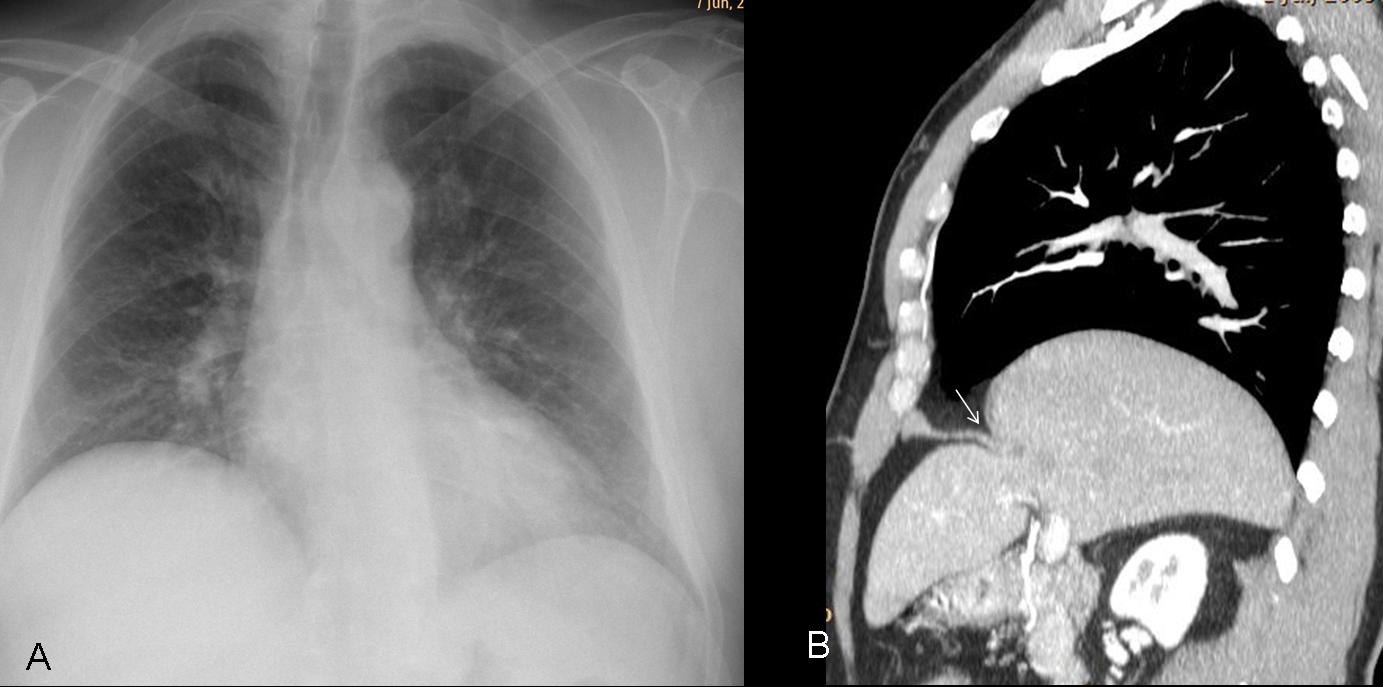
Fig. 8
Fig. 8 (above): 45-year-old asymptomatic male with previous history of trauma. Chest radiograph shows elevation of right hemidiaphragm. CT confirms the rent (B, arrow) and shows herniation of most of the liver.
Multislice CT is the technique of choice for studying diaphragmatic hernias. Barium is a safe and accurate method for detecting bowel hernias by demonstrating the narrow areas where the bowel crosses the rent (‘kissing beaks’ sign). Unfortunately, nobody uses barium any more. Had to dig up an old case to show the sign (Fig. 9).
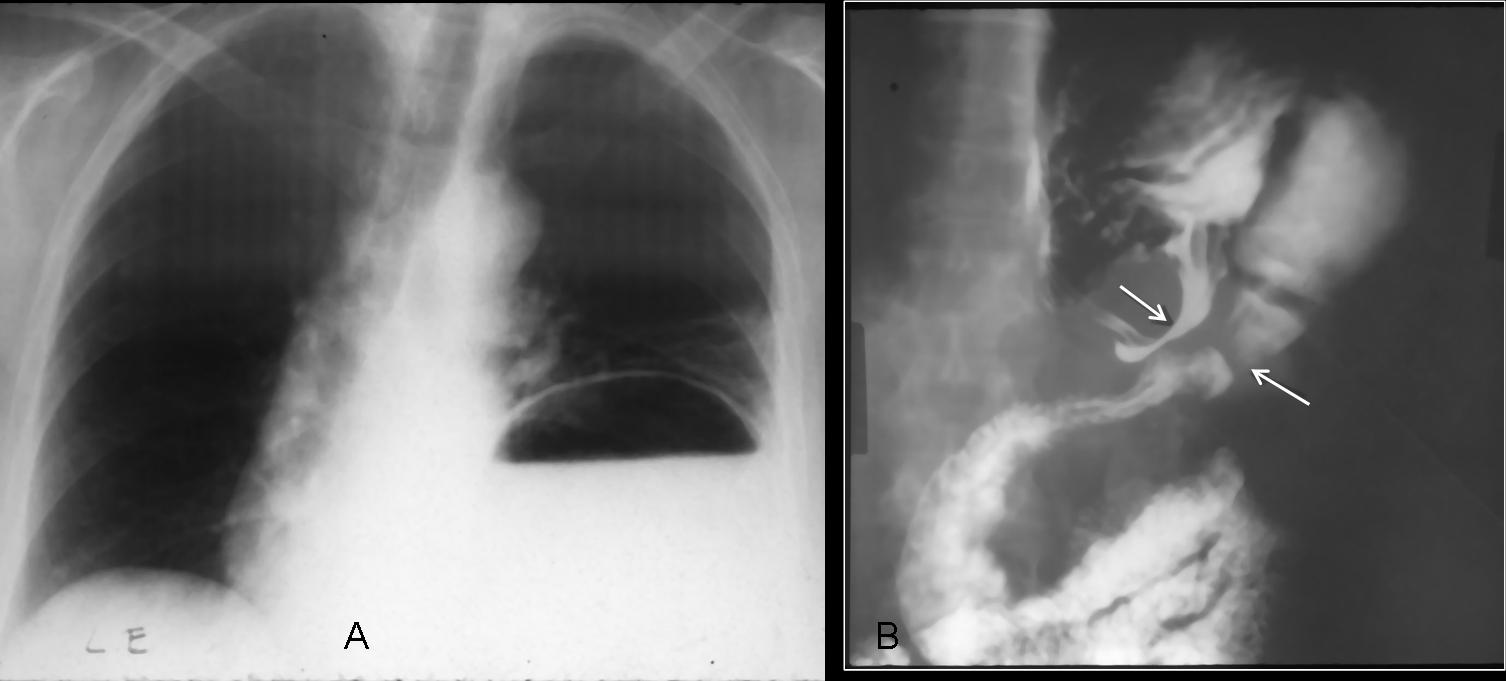
Fig. 9
Fig. 9 (above): marked elevation of left hemidiaphragm secondary to gastric hernia. Barium swallow shows the ‘kissing beaks’ sign which marks the location of the rent (B, arrows).
Fatty diaphragmatic hernias are common in elderly patients, and usually appear as localised diaphragmatic lumps. Occasionally, they may be large and simulate an elevated hemidiaphragm (Fig. 10).
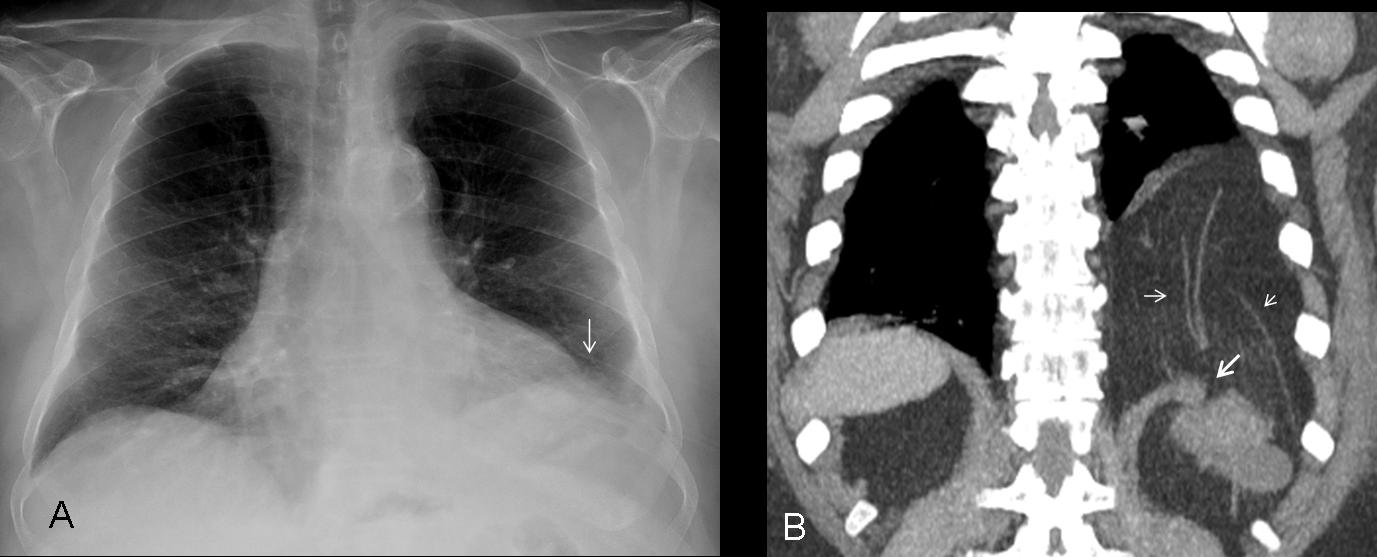
Fig. 10
Fig. 10 (above): elevated left hemidiaphragm with fuzzy border in a 74-year-old man (A, arrow). Coronal CT shows a large opening with herniation of fat and retroperitoneal vessels (B, arrows). Notice how the decubitus position increases the herniation.
Subpulmonic effusion is the most common cause of false diaphragmatic elevation. Pleural fluid collects between the diaphragm and the lung, simulating an elevated hemidiaphragm (Figs. 11 and 12).
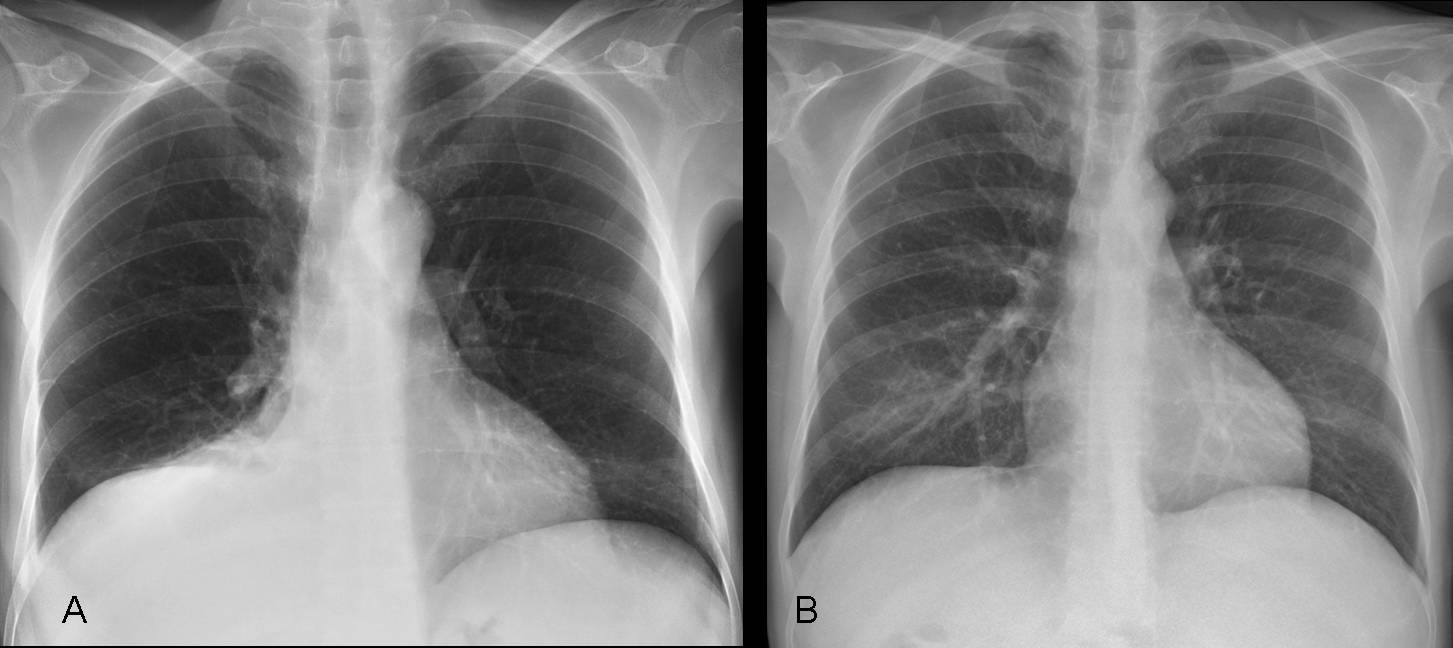
Fig. 11
Fig. 11 (above): chest radiograph (A) shows the classic signs of subpulmonic effusion: a dense and elevated hemidiaphragm. A shallow costophrenic sulcus is not seen in this case. Compare with radiograph after resolution of fluid (B).
TIP: in my experience, the lateral film is very helpful in the diagnosis of subpulmonic effusion. When the signs are not very evident in the PA film (Fig. 12a), there is always obliteration of the posterior costophrenic sulcus (12b, arrow). CT shows a significant amount of free fluid in the right pleural space. US study is easier than a lateral decubitus film to confirm the presence of fluid.
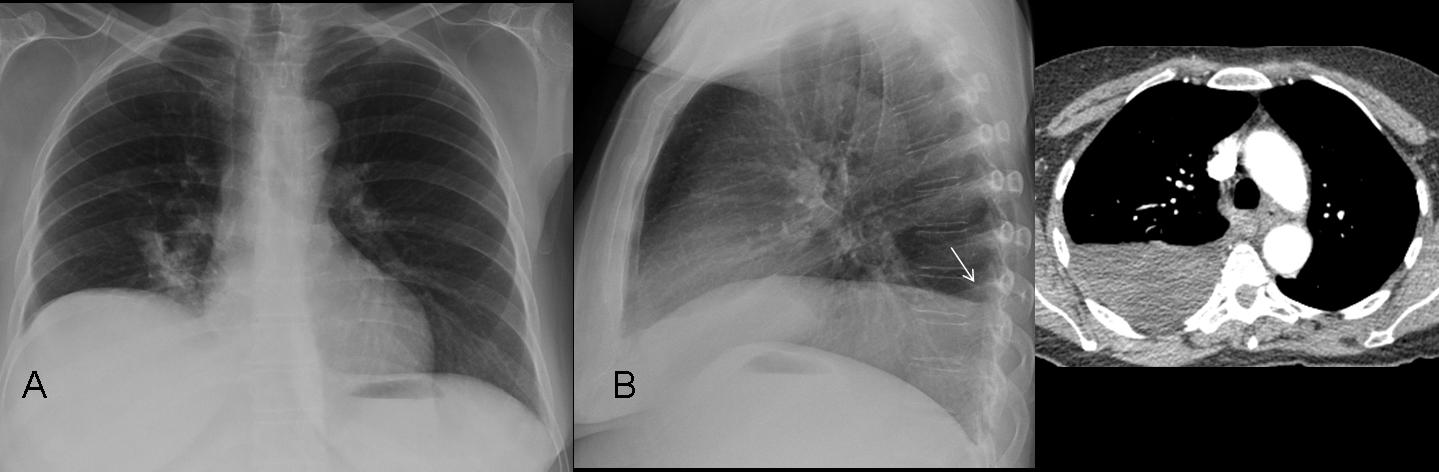
Fig. 12
When other causes are excluded, we have to consider eventration or diaphragmatic paralysis. In eventration, the muscle is replaced by fibrous tissue. Paralysis may be due to any process that affects the phrenic nerve, such as a tumor or surgery (Fig. 13), although in most cases, the cause is not found.
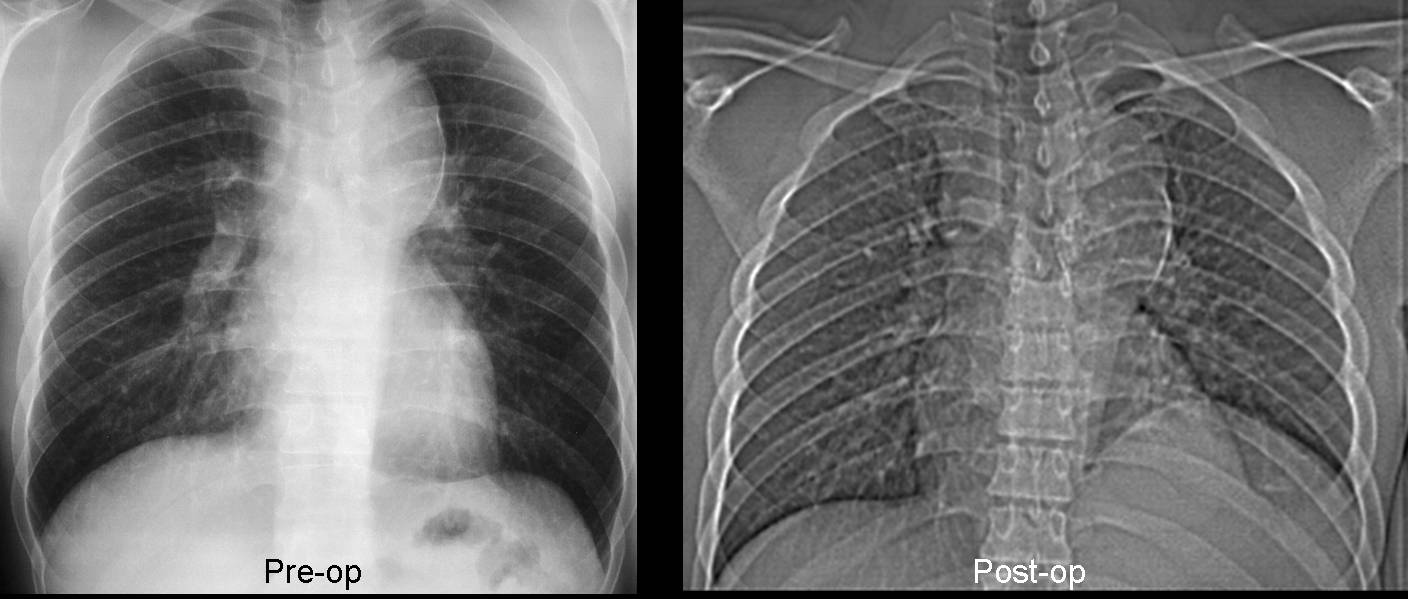
Fig. 13
Fig. 13 (above): chest radiographs before and after surgery for thoracic aneurysm. Post-op film shows elevation of left hemidiaphragm secondary to phrenic nerve injury.
Eventration/paralysis are not uncommon in elderly people, but such findings are usually irrelevant. Comparison with previous films helps to determine whether the condition is stable.
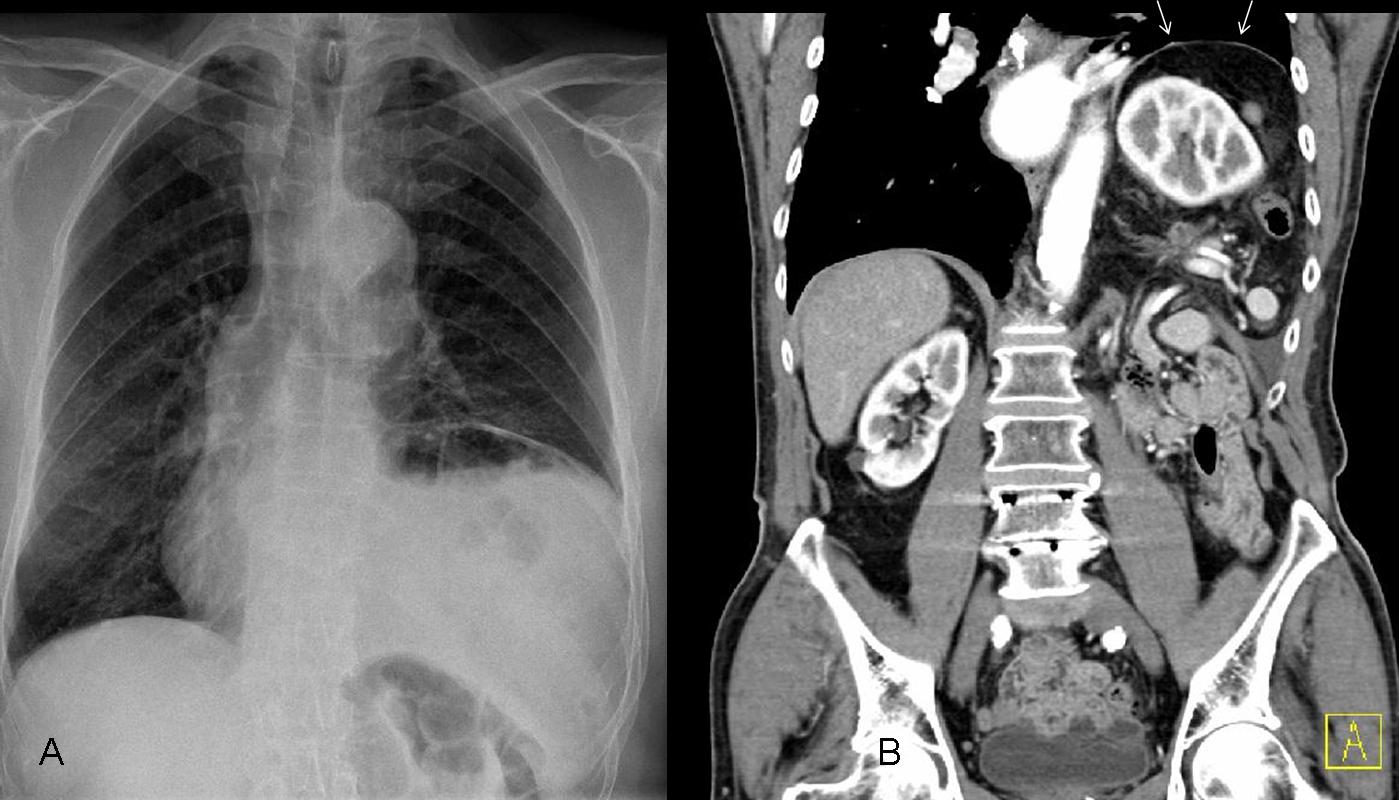
Fig. 14
Fig. 14 (above): a 76-year-old patient with eventration/paralysis of left hemidiaphragm. Coronal CT shows an intact left hemidiaphragm (B, arrows) that is markedly atrophic when compared to the right.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- The main causes of unilateral diaphragmatic elevation are paralysis/eventration, abdominal processes, loss of lung volume, and false elevations.
- The most common cause of false elevation is subpulmonic fluid
- When there is a significant history of trauma, rule out diaphragmatic herniation.
- Diaphragmatic eventration or paralysis are relatively frequent in elderly persons, but these findings are usually not significant.


errore od orrore? Dr Pepes rivedi le immagini: il caso è stato già presentato dal Professore Caceres!!!!Aneurisma del tronco brachiocefalico!
….sollevamento cupola diaframmatica, con strie disatelettasiche, nonché sospetto di addensamento polmonare alla base polmonare dx,(con D-dimeri elevati?), farei un ecodoppler arto inferiore per escludere un TEP(trombo-embolismpo polmonare).
D-dimer normal
….scusa gentile collega, ma il dubbio è atroce: avete fatto una ecografia dell’addome, preliminare, all’Rx-torace?
No, but we did a CT afterwards.
The images I see is belonged to the case of the last week, I think that there is an error in loading the images ??
Yes, there has been a big snafu. It will be corrected as soon as possible.
Thank you calling it to my attention
And you get your money back!
🙂
I seen in the lateral film that the posterior costo-pherenic recess is obliterated by homogenous opacity rising upward this is associated with eccentric dome of the right diaphragmatic copula so subpulmonic effusion is highly considered, …just one look with ultrasonography will solve the problem
is not so easy to say someone if there is sub pleural effusion because
-Dome is not laterally displaced and we dont have straight edge on lateral view at the major fissure
– we can see clearly the vascular shadows sub diaphragmatic.
it was helpfull a decupitus view.
the fact is that we have elevation of the right hemidiaphragm with subsegmental atelectasis
no shifting of mediastinum
and a small pleural effusion on the right costophrenic angle.
a woman with abdominal pain and moderate distension.
I agree with you.
Diaphragmatic eventration
1.pleuritis seq. Pulm dxt.
2. Linear atelektasis lobulus inf. Pulm. Dxt.
3. Diaphragmatic eventration
I agree with Gus’ initial assessment: a lack of lateral peaking of the right hemidiaphragm weakens the argument for a subpulmonary effusion. A right decubitus view would help to rule this in or out. Symmetric elevation of the hemidiaphragm is sometimes associated with phrenic nerve palsy, however, these patients are frequently asymptomatic making this unlikely here. Given our patient’s GI symptoms (abdominal pain and distention), I would seriously consider hepatomegaly secondary to hepatic carcinoma. But I don’t think one can definitively make this diagnosis based solely on these images. A CT would help. Looking forward to the answer 🙂
CT definitely helped in this case. I agree with your impression that the appearance of the elevated diaphragm is against subpulmonary effusion.
ALL OF YOU AGAINST ME, OK……:)
Tough luck! 😉
I seen that is not a typical subpulmonic effusion, but I suggested that is the possible diagnosis as the posterior costo-pherenic recess on the right side is obliterated and subpulmonic is often associated with free effusion, also the abdominal pain may be originated from basal pleurisy which may be associated with pleural effusion, However I see that ultrasonography is cheaper, rapid with no irradiation which may reveals that problem
None of the above:)
In the PA projection, the elevated right hemidiaphragm forms a round unbroken line arching from the mediastinum to the costal arch suggesting eventration, there is no Loss of the outline on lateral view ruling out pleural effusion, consolidation, however the unilateral right side eventration is extremely rare. There is some plate like Atelectasis on the ipsilateral side, and clinical history given by Dr. pepe indicating pathology below the diaphragm, a hepatic mass leading to hepatomegaly or Tumour of diaphragm (Lipomas – neurofibrimas, fibromas) could be considered.
Good discussion. CT on Friday.
Professor I forgot to mention metastasis as a cause of diaphragmatic elevation with particular reference to ovarian carcinoma and metastasis in these cases is not random. After initial implantation on the fallopian tube and to the contralateral ovary, then the most common sites for distant metastasis are the omentum and the peritoneum. The peritoneum beneath the right diaphragm and the small bowel mesentery are preferentially involved.
Good. Can you wait for the CT until Friday ?
NICE CASE PROFESSOR..REALLY TOUGH ONE !THE OVOID OPACITY IN THE LOWER LUNG IS CLUE TO DIAGNOSIS?BUT AT LEAST I THOUGHT SOME MALIGNANT PATHOLOGY BELOW THE DIAPHRAGM.BUT IF THE RADIOGRAPHS ARE PUT IN THE EXAM, DO WE NEED TO REACH THE EXACT DIAGNOSIS OR IS IT THE APPROACH THAT MATTERS??PARTICULARLY IN SUCH TYPE OF CASES.
1 i like to know the nationality of the woman or if she had a trip in a tropical place (Amebic abscesses)
2 if she had respiratory problems in the past, if is something new and if she has symptoms from respiratory system.
if she was operate or if she had viral infection.
(Phrenic Nerve Paralysis – unilateral side eventration)
3 if she had ovary problem?(mets – ascites meigs syndrom)
4 i need a extra Rx exams Breathe in-Breathe out and abdomen Rx.
is too many?:)
1. Spaniard. No
2. No. No
3. Yes
4. No
🙂
metast endobronchiali?
You may have a point there. Wait until Friday.
There is some degree of atelectasis of medial (and also of the nearby territory) segment of inferior right lobe probably due to the “compression” made by a sub-phrenic patologic involvement (metastatic? abscess? other?).
I choose answer 1 and 2 and wait for friday.
I think I a late..Anyway, my considerations are:
-Diafragm alteration (RDT, frenic nerve palsy)
-Loss Volume Right lower lobe ( I see some blurring of the posterior right hemidiafragm, could represent colalpse?
-Infradiafragmatic Process (hepatomegaly, liver tumor)
great case!!!!
HEPATOMEGALY