Dr. Pepe’s Diploma Casebook: Case 73 – SOLVED!
Dear Friends,
After mid-term vacation, I return with renewed energy! Presenting images of a 54-year-old man with a moderate cough.
Check the image below, leave your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Apical bulla with fungus ball
2. Carcinoma of the lung
3. TB and granuloma
4. None of the above
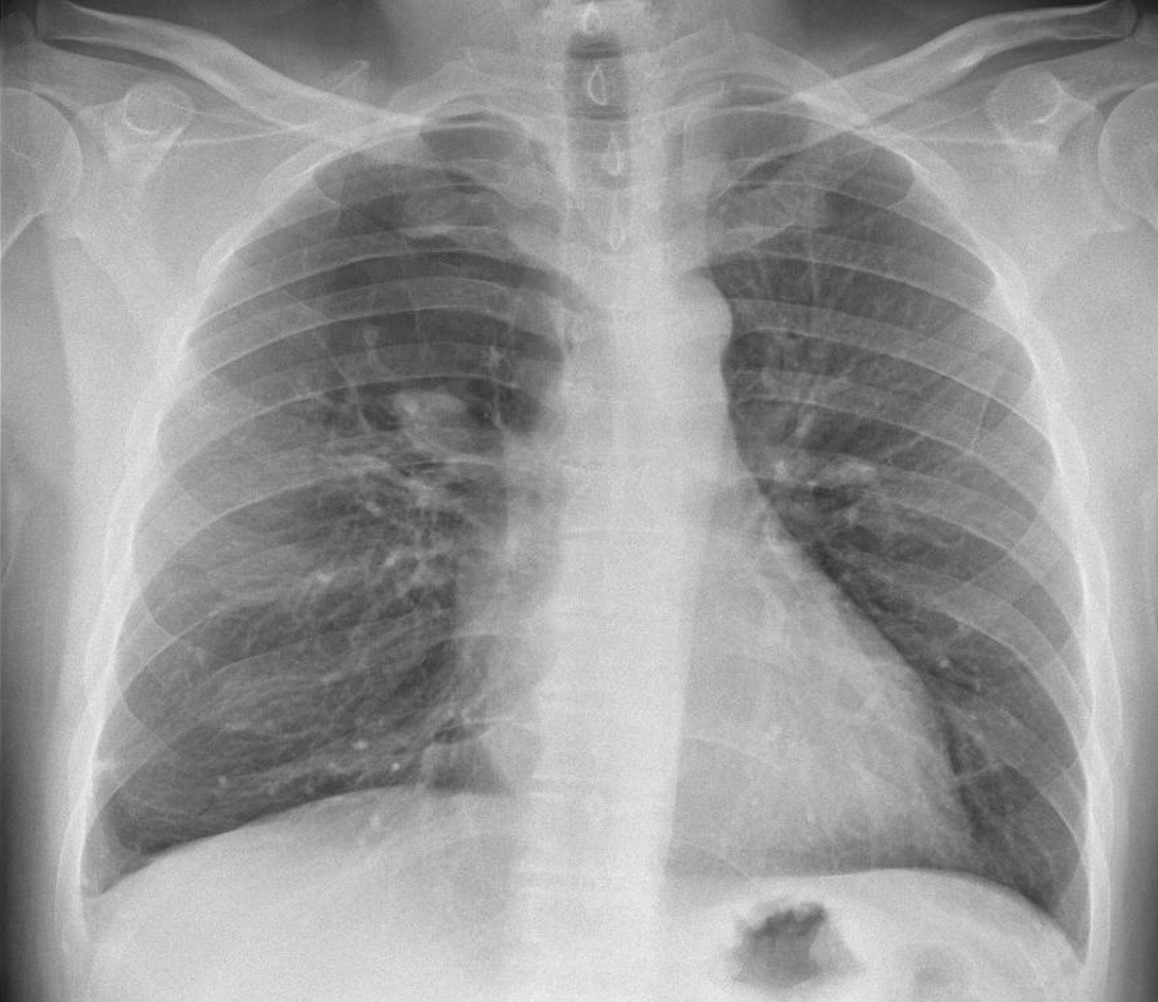
Findings: chest radiograph shows a hyperlucent area in the upper third of the right lung, with a lowermost round opacity (A, arrow). Coronal CT shows a large mucus plug at the origin of the apical bronchus of RUL (B, arrow) and no distal bronchi. The appearance is highly suggestive of segmental bronchial atresia.
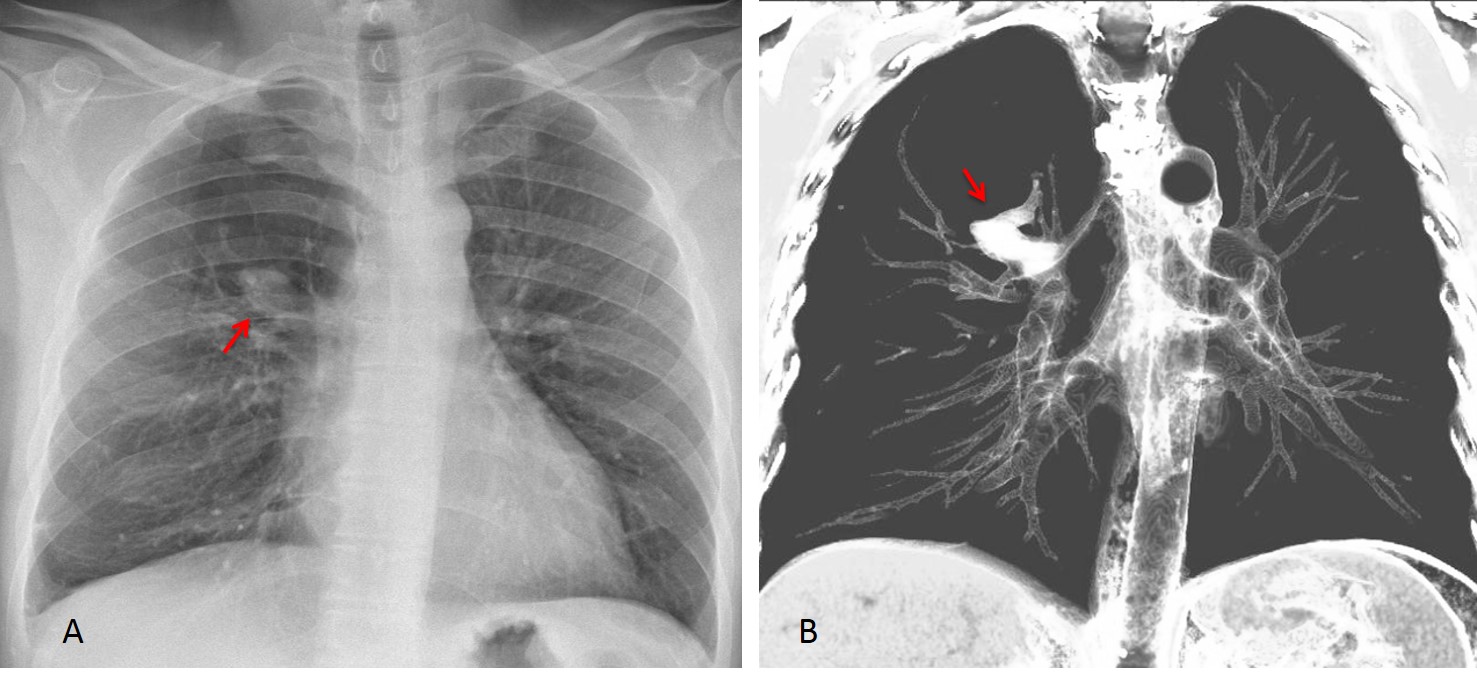
Final diagnosis: congenital bronchial atresia
The objective of this presentation is to discuss common congenital malformations of the lung. Contrary to what may be believed, congenital diseases are not rare in adults. My intention is to present the imaging features of the most common ones so that they will be recognised and not mistaken for more serious conditions. Congenital malformations can be focal (bronchial atresia and pulmonary sequestration) or affect one lung (agenesis of the lung and hypogenetic lung syndrome).
In my experience, congenital bronchial atresia is the most common lung malformation seen in adults. Congenital bronchial atresia results from proximal interruption of a segmental bronchus, which causes overinflation of the affected segment and secondary mucus impaction. Chest radiography shows a focal hyperlucent area with internal mucus impaction. CT depicts these findings better (Fig. 1). Inspiration and expiration films help to confirm air-trapping (Fig. 2). In case of doubt, bronchoscopy excludes other causes of bronchial obstruction.

Fig 1, A+B
Fig 1: PA chest film shows numerous serpiginous shadows in the LUL (A, arrows) with associated hyperlucency of the underlying lung. Serpiginous shadows bring to mind two possibilities: arteriovenous malformations and mucus plugs. The hyperlucent lung and the LUL location suggest congenital bronchial atresia as the first option.
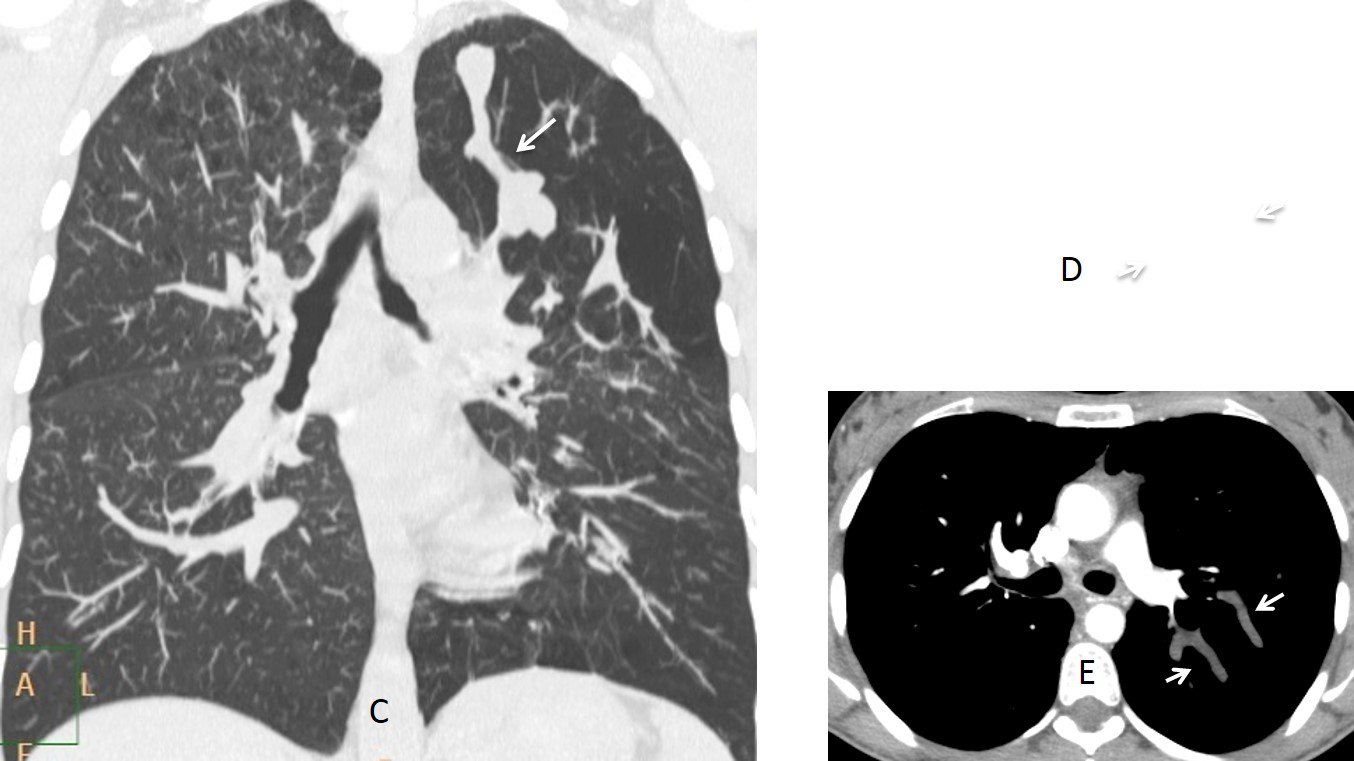
Fig. 1, C,D,E
Coronal and axial CT show the segmental hyperlucency and mucus plugs (C and D, arrows). Enhanced axial CT confirms the non-enhancing mucus plugs (E, arrows).
Diagnosis: congenital bronchial atresia
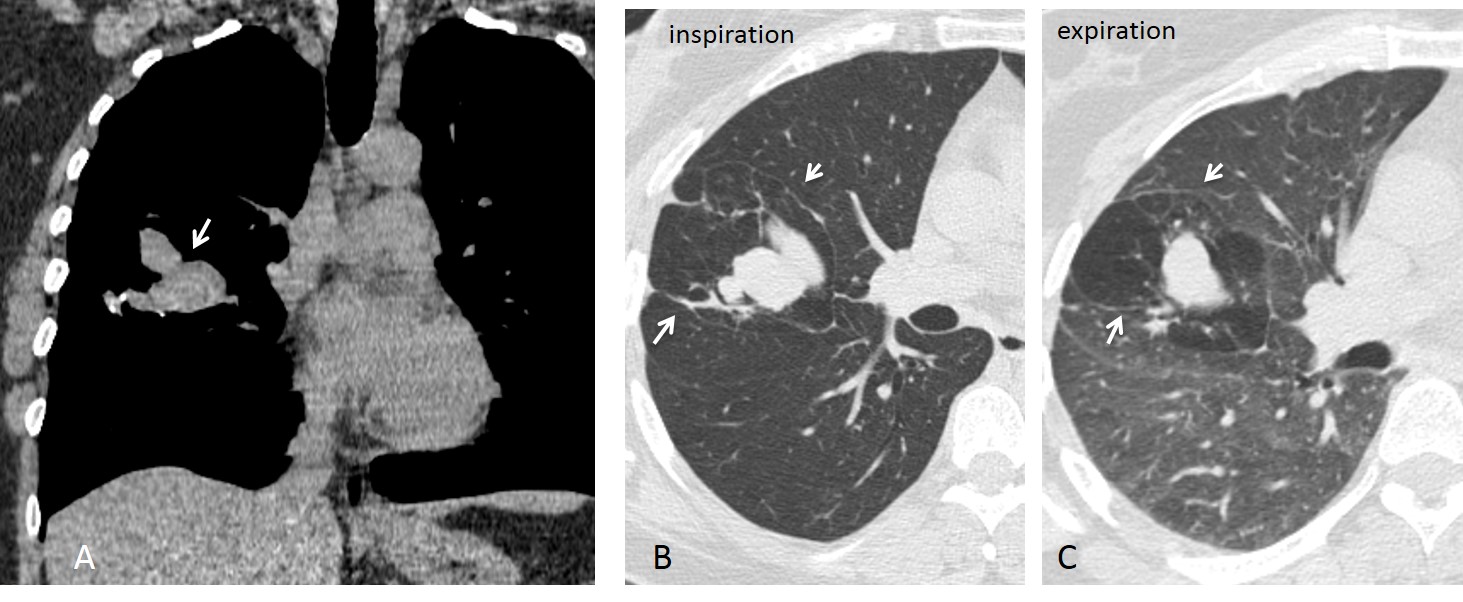
Fig. 2
Fig. 2: 48-year-old woman with bronchial atresia. Unenhanced coronal CT demonstrates the typical finger-in-glove appearance of mucus impaction (A, arrow). Axial CT with pulmonary window shows areas of emphysema around the mucus impaction (B, arrows), with air-trapping on expiration (C, arrows). Bronchoscopy was negative. This case emphasises the value of expiratory films to demonstrate air trapping.
Intralobar pulmonary sequestration consists of abnormal lung tissue that is not connected with the bronchial tree and is irrigated from systemic vessels. The chest radiograph shows a lower lobe opacity with recurrent infections that do not heal completely. CT confirms the diagnosis by demonstrating the systemic artery arising from the aorta (Figs. 3 and 4).

Fig. 3, A,B
Fig. 3: 41-year-old man with recurrent pneumonia in the RLL. PA and lateral radiographs depict an opacity in the RLL with cystic areas showing air-fluid levels (A and B, arrows). The appearance is non-specific, but the recurrent pneumonia and cysts suggest pulmonary sequestration. CT should be performed to investigate this possibility.
Enhanced axial CT shows cystic areas (C, arrows) within a large basal infiltrate. A caudal view shows a systemic artery arising from the abdominal aorta (D, arrow). The systemic artery is better depicted in the volume reconstruction (E, arrow). Surgical diagnosis: pulmonary sequestration.
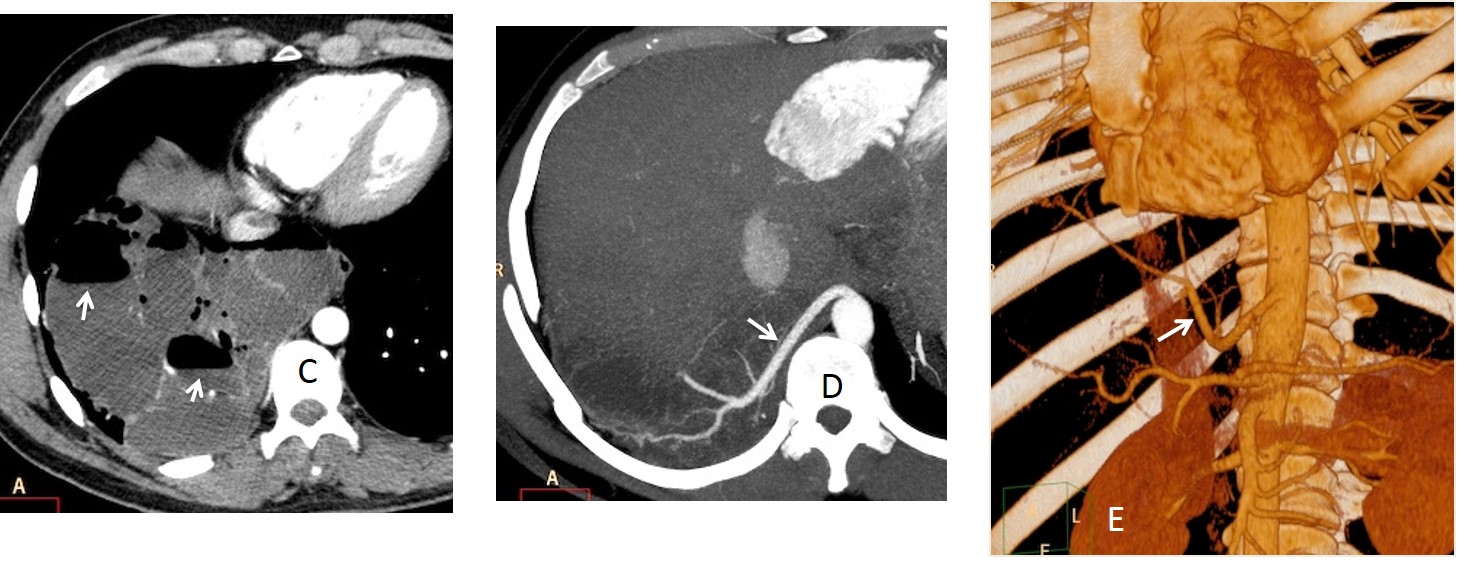
Fig. 3, C,D,E
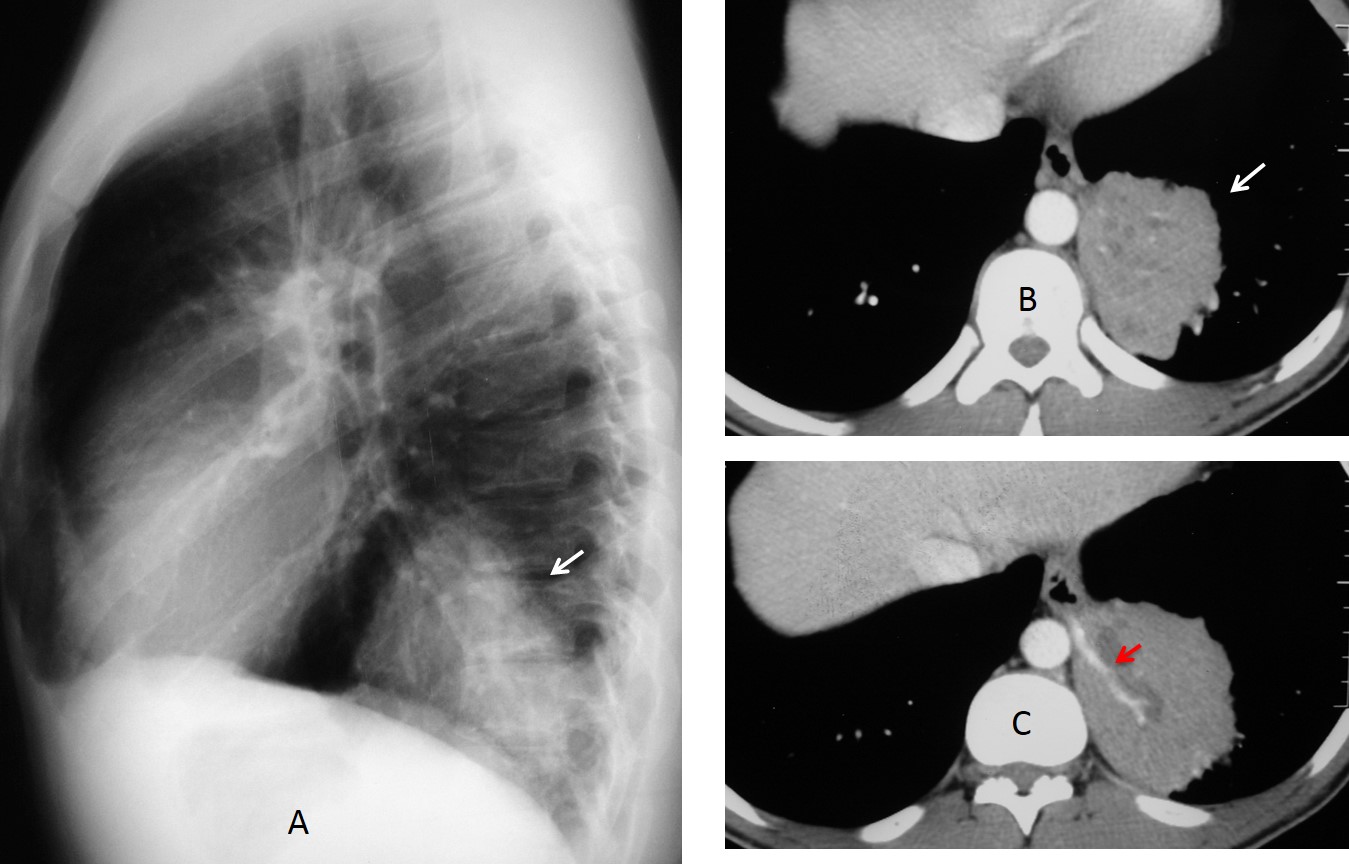
Fig. 4
Fig. 4: 25-year-old man with a solid-looking mass in the LLL (A, arrow). Enhanced axial CT shows a mass with minute cysts (B, arrow) with a systemic artery arising from the aorta (C, arrow). Surgical diagnosis: sequestration.
Hypogenetic lung (scimitar syndrome, venolobar syndrome) is a relatively common malformation that occurs secondary to agenesis of one or two lobes, with abnormal venous drainage of the lower lung in 80% of cases. The malformation usually affects the right lung. On plain films it appears as a small right hemithorax with mediastinal shift to the right. The scimitar vein is visible in about 50% of chest radiographs and is helpful in cases of mild hypoplasia. CT confirms the findings by demonstrating the absent lobe(s) and the abnormal vein, when there is one (Figs. 5 and 6).
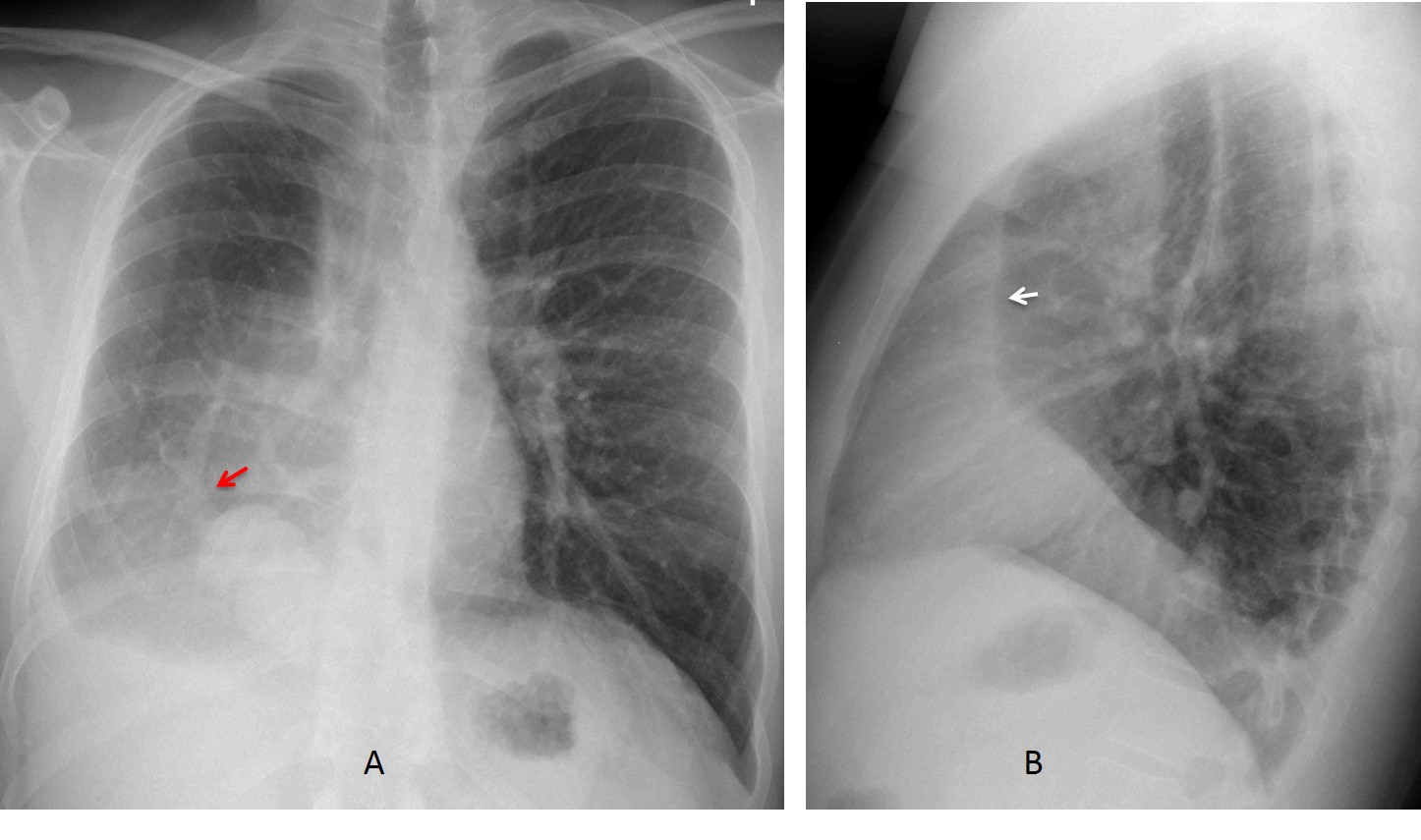
Fig. 5, A,B
Fig. 5: 22-year-old man, asymptomatic. PA radiograph shows typical findings of hypogenetic lung: small right hemithorax with right mediastinal displacement and blurring of the right heart border. A scimitar vein is visible (A, arrow). The vertical retrosternal line (B, arrow), is present in most cases.
Enhanced coronal reconstruction confirms the scimitar vein (C, arrow) Axial CT shows the abnormal bronchial branching (D, arrow) and the smaller right lung. The shortened A-P diameter of the lung is the cause of the retrosternal line in the lateral view. Diagnosis: hypogenetic lung.

Fig. 5, C,D
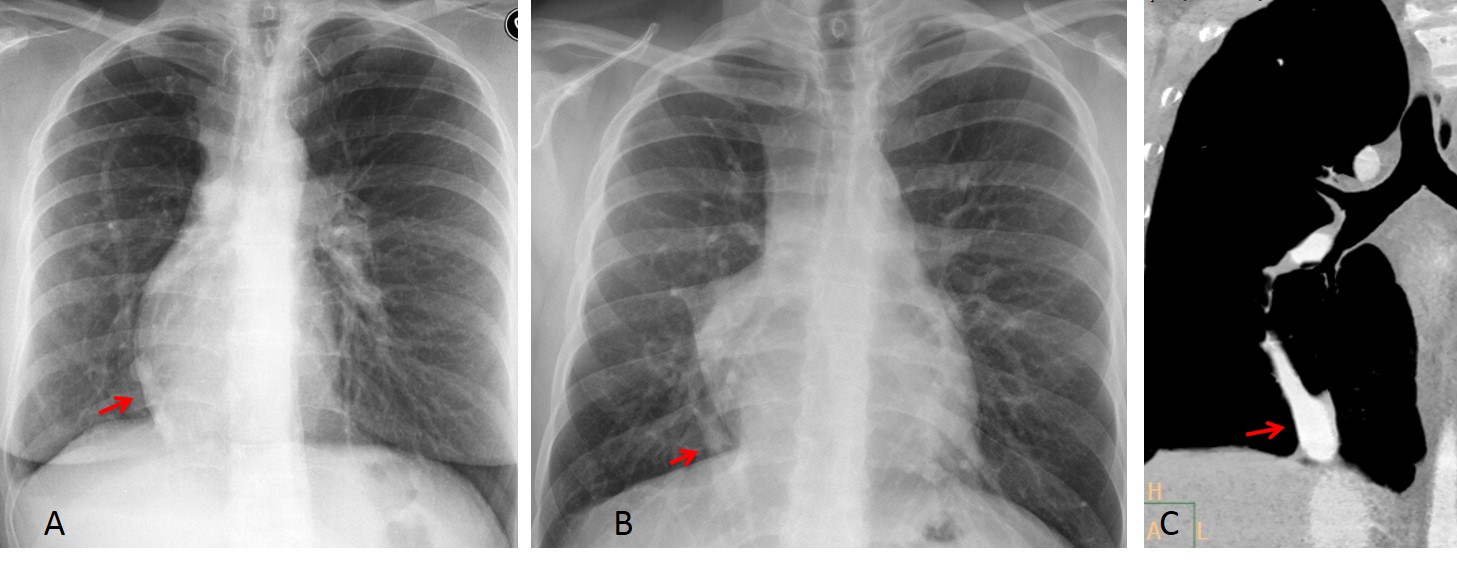
Fig. 6
Fig. 6: two examples of mild hypogenetic lung. In both cases, there is slight displacement of the mediastinum and heart towards the right, simulating dextrocardia. The scimitar vein helps to suggest the correct diagnosis (A and B, arrows). Enhanced CT confirms the vein in the second case (C, arrow).
Unilateral pulmonary agenesis is due to arrested development of one lung. It occurs equally on both sides. It is asymptomatic and usually discovered accidentally. Plain radiography shows opacity of one hemithorax with marked mediastinal shift, simulating a pneumonectomy. The lateral view shows en enlarged anterior clear space secondary to herniation of the opposite lung. CT confirms absent or minimal lung tissue.
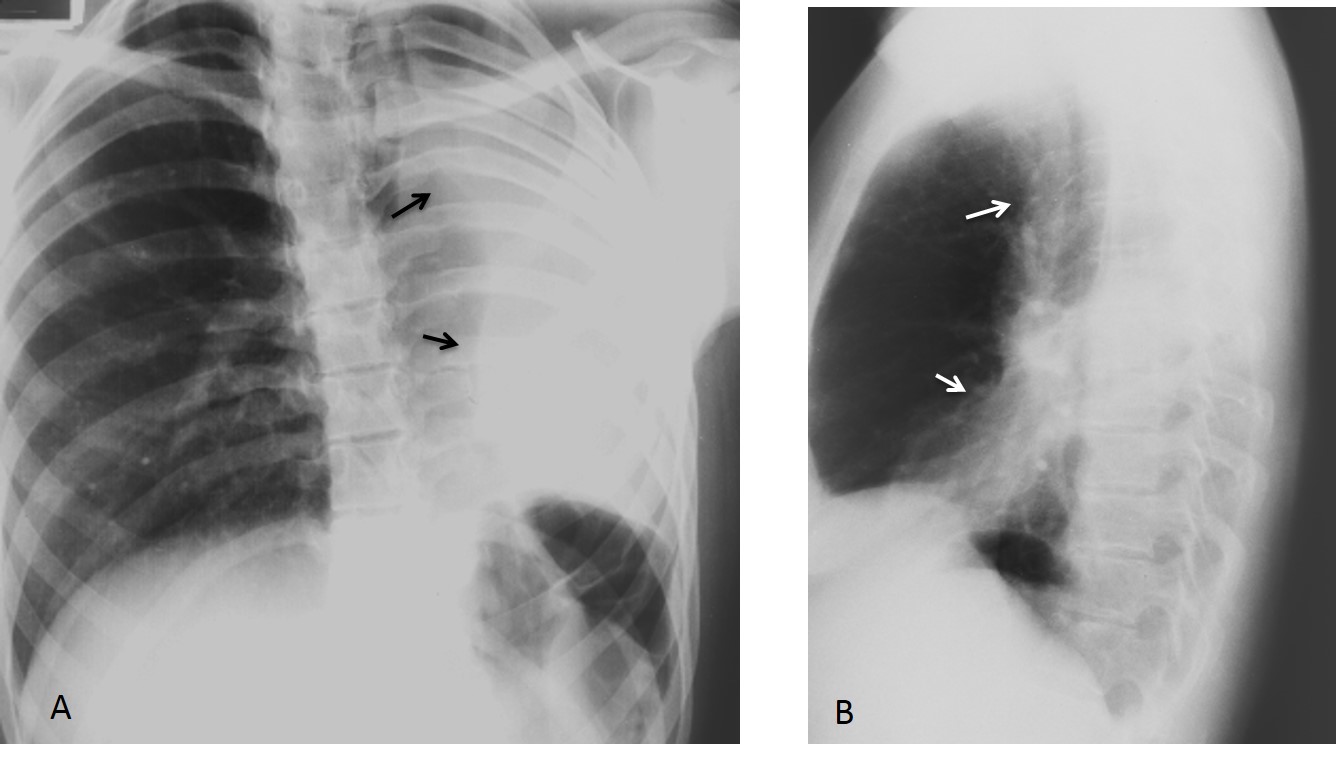
Fig. 7, A,B
Fig. 7: 40-year-old man with left lung agenesis. The PA radiograph shows a small airless left hemithorax with crowding of the ribs and marked herniation of the contralateral lung (A, arrows). The lateral film confirms herniation across the anterior clear space (B, arrows).
Axial CT depicts a small remnant of hepatised lung tissue (C and D, black arrows) and the absent left bronchus (D, red arrow). Note herniation of the right lung behind the sternum. An interesting finding is that the homolateral pulmonary artery is usually of normal size (C, blue arrow).
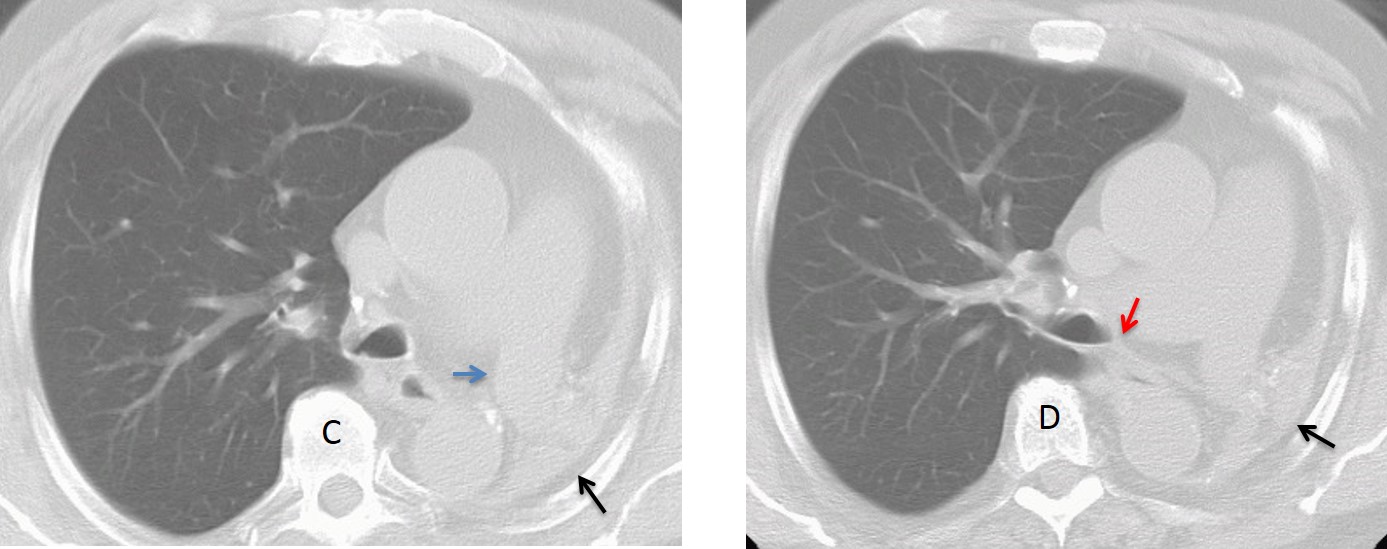
Fig. 7, C,D
In lung agenesis, the normal lung sometimes herniates markedly into the contralateral hemithorax. In the chest radiograph, this may produce the deceiving appearance of aerated lung with chronic pleural disease. The diagnosis is obvious on CT.

Fig. 8
Fig. 8: marked right lung herniation in left pulmonary agenesis. The PA view simulates chronic pleural disease of left side (A, arrows). CT shows marked herniation of the normal lung, reaching the opposite chest wall (B and C). There is considerable posterior displacement of the heart and mediastinal structures.
Follow Dr.Pepe’s Advice:
1. Congenital lung malformations are not unusual in adults. Most are asymptomatic and are discovered when a chest radiograph is taken.
2. Bronchial atresia is characterized by focal hyperlucency and mucus plug.
3. In intralobar sequestration there are recurrent lower lobe infections.
4. Hypogenetic lung is accompanied by a scimitar vein in 80% of cases.
5. Congenital agenesis simulates a previous pneumonectomy.


Hello,
there is nodular opacity in apex of right hilum connected with hyperlucency of upper part of right lung.
I suppose it is bronchial atresia.
I cannot explain clinical symptom -moderate cought- with radiologic findings.
I guess all of us have some cough sometimes
True:)
Opacity in the upper part of the right hilum with elevation of the hilum (lost of volume of the right upper lung) and hyperlucency in the upper right lung with a few visible vassels.
i think a lateral view can give us more informations.
My First choise is carcinoma because the age of the patient or carcinoid .
Second choise mucoid impaction
…l’opacita ” a dito di guanto” rappresenta un broncocele riempito di secrezioni mucose….mentre l’iperdiafania circostante rapresenta ” l’air trapping” determinato dalla circolazione collaterale , attraverso i pori di Khon, degli adiacenti segmenti polmonari normo-ventilati….Saluti da BARI…..
There is hyperlucency around the well defined nodule in the right upper lung zone. In this area of lung lucency, number of lung marking is lessor than other part of the lungs. Bronchial atresia is suspected.
Is there also a nodule at the left side, behind the heart apex? Or am I just hallucinating?
Or is that a monster nipple? 🙂
Regardless of my question. I will consider it a malignancy because of the elevation of the hilum. And I think there is no real lucency, it is caused because of the projection of scapula and rips.
PS. Amazing, how old school Radiologist survived without CT. 🙂
I will take it as a compliment! I just discovered in the chest radiograph a lung nodule that was missed in two previous CTs.
Yes, you are.
Apical bulla with fungus ball due to right mid-upper hyperlucency , splayed pulmonary vasculature and nodular opacity above right hilum. Also, elevation of right hilum. (small) left pleural effusion?
Right upper lung zone bulla ( devoid of lung markings) with right hilar opacity, likely nodal. TB is most likely
Slight Right pleural effusion with intersticial parahiliar nodule that could be related to: 1. carcinoma vs 2. Carcinoid vs 3 hamartoma vs metastasis
considerar aneurisma de rasmusen
Well lucency is there involving Rt lung parenchyma upper zone with visualization of vascular makings…soo no pneumothorax….Rt perihilar nodular opacity is there with tiny scattered calcification rt lower zone….will prefer TB more then malignancy….
Hmm…by the way what’s moderate cough???… Do we grade cough as mild, moderate n severe….:-):-):-)
I usually grade it as: a little, a little more, annoying and obnoxious 😉
Right perihilar tubular like opacity with paucity of lung markings distally in the right upper zone. Overall features are of bronchial atresia with mucus impaction.
Also blunting of right costophrenic recess and small opacity at the periphery of right lower zone with radiating reticulation towards it, representing pleural thickening and fibrosis. – think this is more of incidental finding.
The correct diagnosis is bronchial atresia.
Congratulations to Borsuk, who was the first to make the diagnosis.
….complimenti anche al dott. GEnchi che ne ha descritto la semeiotica elementare ed il substrato anatomopatologico !LUNARE il Barca visto contro il Paris S. Germain!!!!
[…] Most are asymptomatic and are first discovered in the adult age. Some of them were reviewed in Dr. Pepe’s Diploma Casebook Case #73. One of the most common is hypogenetic right lung (scimitar syndrome), which gives the chest […]