Dr. Pepe’s Diploma Casebook: Case 99 – A painless approach to interpretation (Chapter 6) – SOLVED!
Dear Friends,
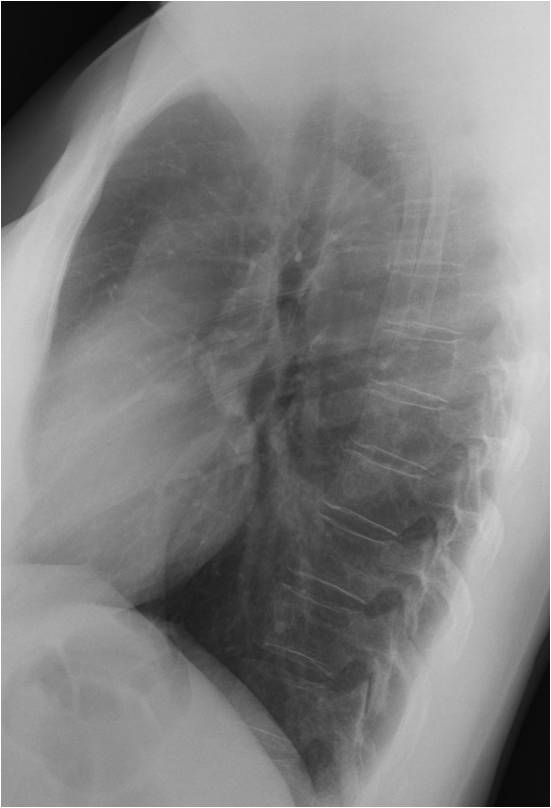
We’re moving on to a new chapter of the Painless Approach to Interpretation, and this week I’m showing the routine control radiographs of a 48-year-old woman, surgically treated for carcinoma of the breast ten years ago.
What do you see?
Check the image below, leave your thoughts in the comments section, and come back for the answer on Friday.

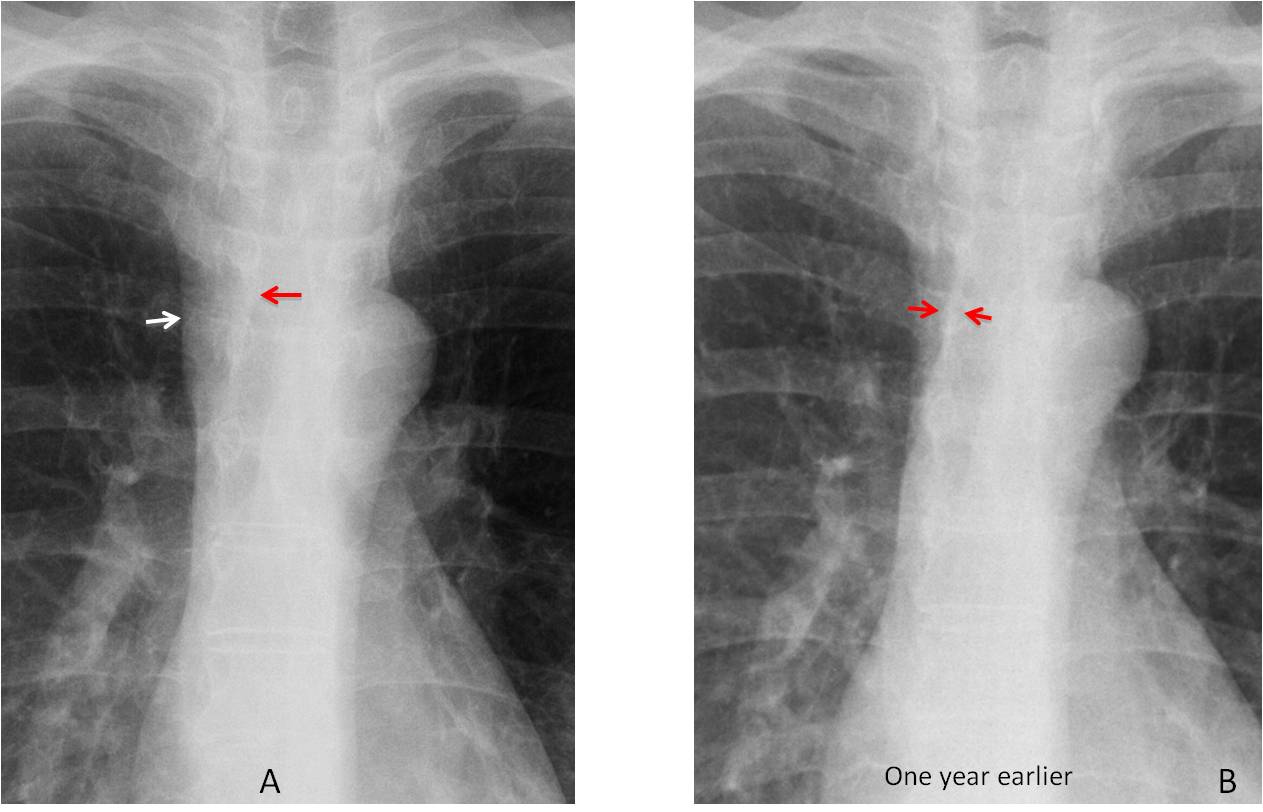
Findings: the PA radiograph shows obvious widening of the right paratracheal line (A, white arrow), which is more evident when compared with a previous examination made a year earlier (B). Note that both borders of the line were seen in the previous radiograph (B, red arrows), whereas only the inner border is visible now (A, red arrow).
Enhanced axial CT confirms the presence of a large right paratracheal lymph node (C, arrow) and bilateral hilar nodes (D, arrows). PET was negative. The nodal distribution in an asymptomatic patient raises the possibility of sarcoidosis, which is known to occur after treatment for solid tumours.
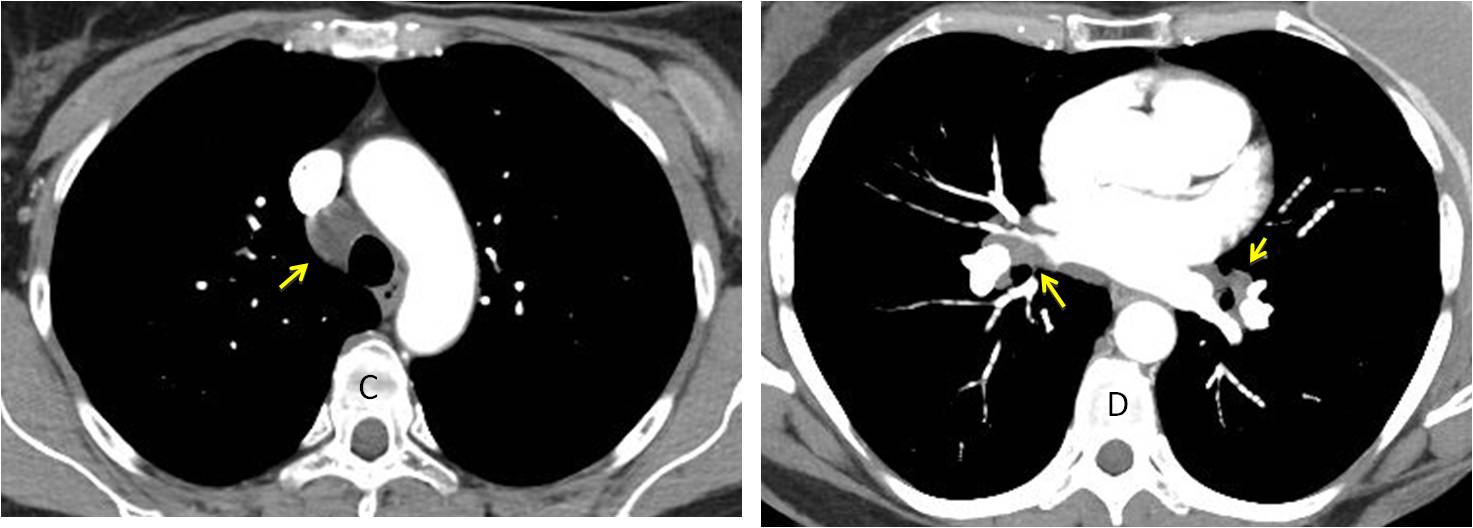
Final diagnosis: sarcoidosis following breast carcinoma treatment.
As we all know, an obvious mediastinal mass is easily seen, but it is equally important to detect subtle mediastinal abnormalities that may uncover serious disease. In this presentation I’d like to discuss a checklist of structures to be examined in the mediastinum to avoid overlooking abnormalities.
The basic checklist for the mediastinum includes the following structures:
1. Mediastinal lines:
– Right paratracheal line
– Paraesophageal line
2. Mediastinal contour:
– Right side: azygos vein and ascending aorta
– Left side: aortic knob and pulmonary arch
Of all the mediastinal lines, the right paratracheal line is the most useful for detecting disease. It is less than 3mm thick and visible in about 95% of PA chest films. Any increase in width over 3mm should be investigated, the most common cause being enlarged lymph nodes (Fig. 1).
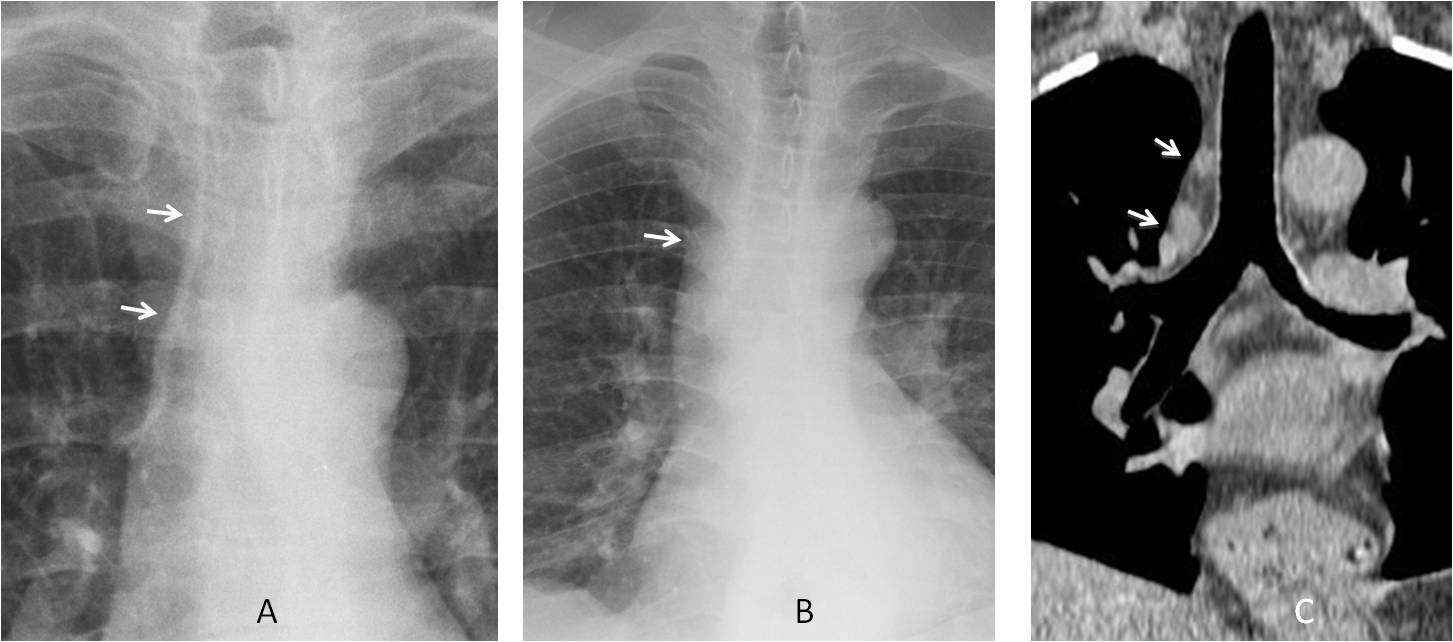
Fig. 1
Fig. 1. A. Normal paratracheal line (A, arrows). B. Widened paratracheal line (B, arrow) in a patient with fever and malaise. Coronal CT confirms mediastinal lymph nodes (C, arrows). Diagnosis: lymphoma.
The paraesophageal line is created by contact of the right lung with the oesophagus and it is seen as an oblique line projected over the spine. Displacement of the interface suggests oesophageal dilatation or hiatal hernia (Fig. 2). Focal bulging may be due to enlarged lymph nodes, oesophageal tumour, or mediastinal cyst.
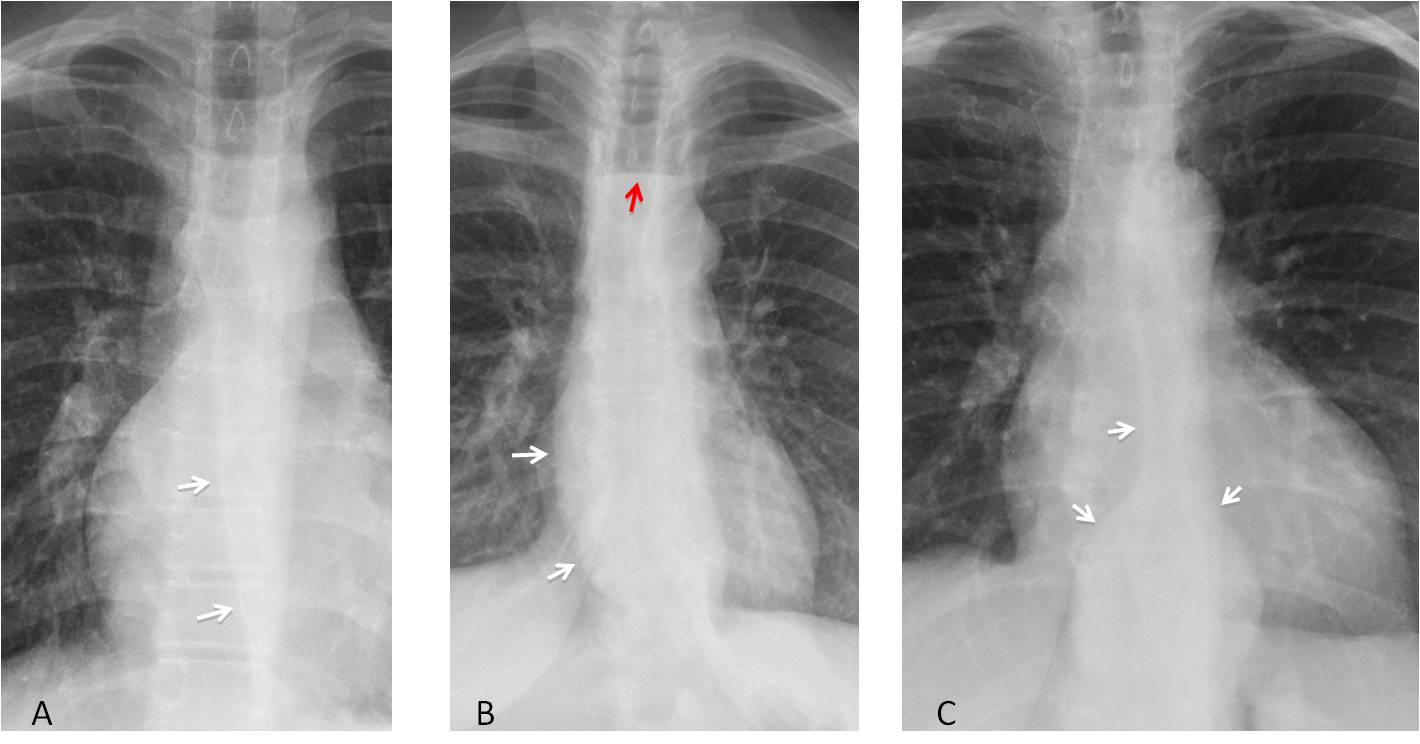
Fig. 2
Fig. 2. A. Normal paraesophageal line (A, arrows).B. Bulging of the oesophageal interface due to achalasia (B, white arrows). Air-fluid level in oesophagus (B, red arrow). C. Hiatal hernia opening the distal paraesophageal line (C, arrows).
The right mediastinal contour has four components: superior vena cava, azygos arch, ascending aorta and right atrium. In my opinion, the two that should be included in the checklist are the azygos arch and the ascending aorta (Fig. 3).
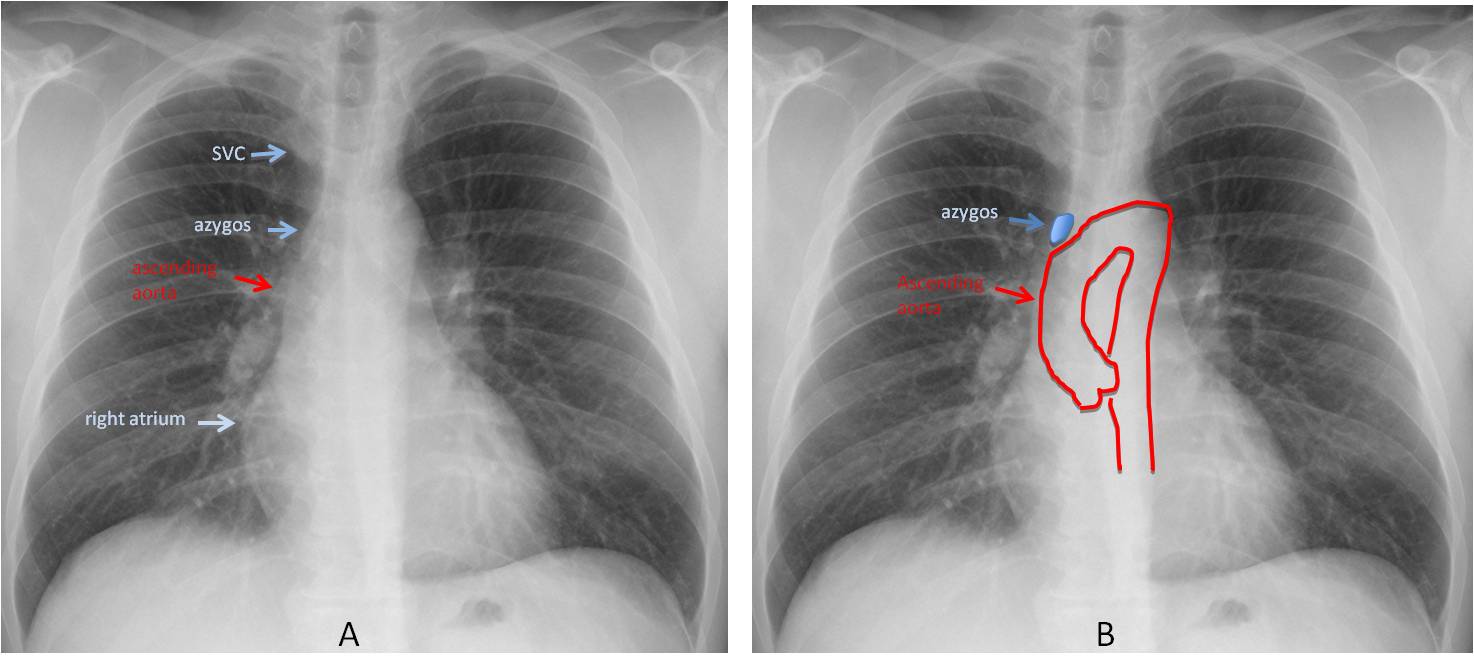
Fig. 3
Fig. 3. Normal chest film showing the four components of the right mediastinal border (A,B).
The azygos arch is the only part of the azygos vein visible in the PA radiograph. It is seen in about 10% of upright PA views. An azygos arch larger than 1cm usually indicates increased blood flow in the azygos system. It may be non-obstructive or secondary to obstruction of the superior or inferior vena cava, in which case the azygos system acts as collateral drainage (Fig. 4).
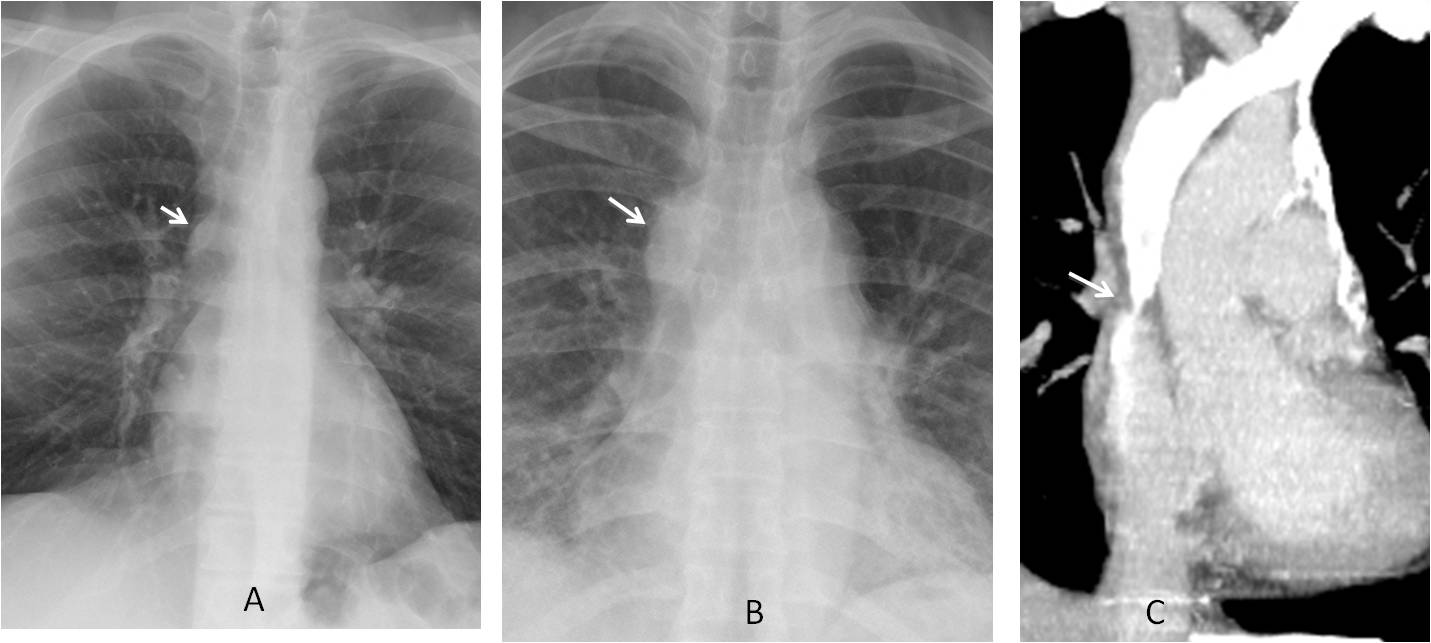
Fig. 4
Fig. 4. A. Normal azygos arch, with typical lenticular shape (A, arrow). In B, the azygos arch is obviously enlarged (B, arrow), as it is acting as a collateral channel for SVC obstruction (C, arrow).
Prominence of the right mediastinum middle segment is usually due to dilatation of the ascending aorta. Four conditions can lead to isolated ascending aorta dilatation: bicuspid aortic valve, ascending aorta aneurysm, type A aortic dissection, and aortic coarctation (Fig. 5).
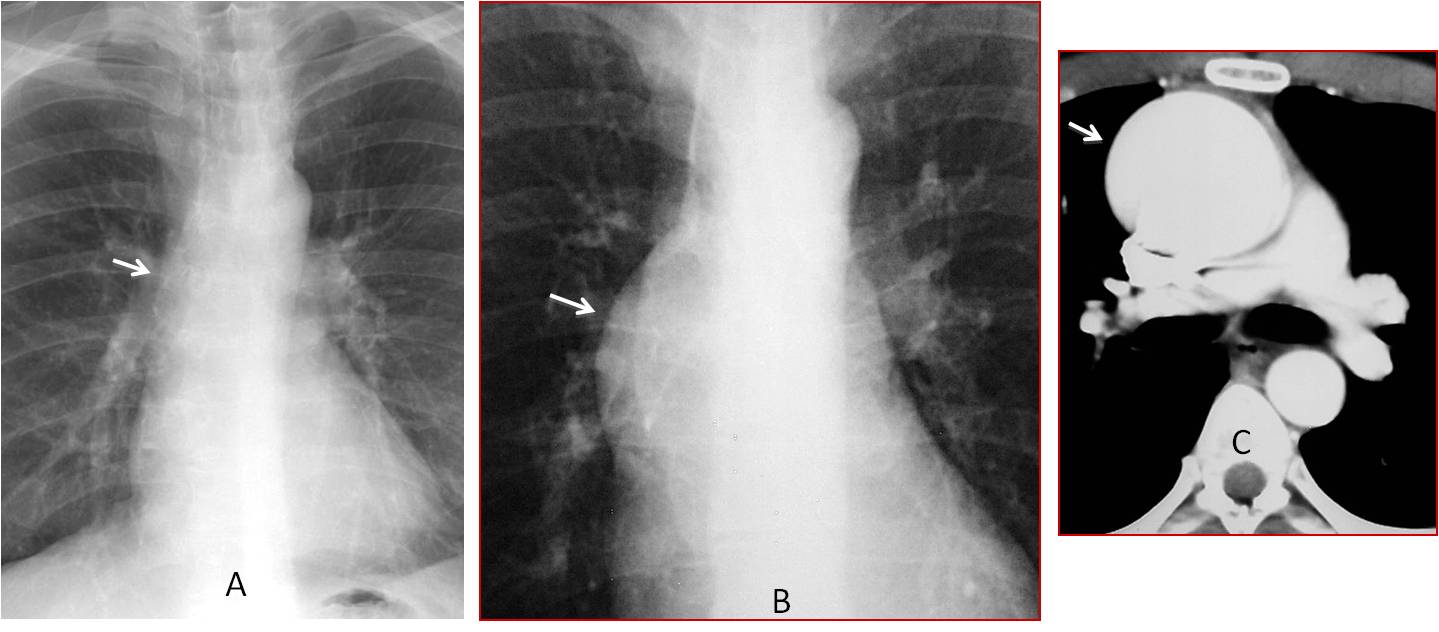
Fig. 5
Fig. 5. A: Normal appearance of ascending aorta (A, arrow). B: Marked prominence of the ascending aorta in an 18-year-old male with Marfan syndrome (B, arrow). Enhanced CT shows an ascending aorta aneurysm (C, arrow).
The left mediastinal contour has three components: the uppermost is the aortic knob, the middle one corresponds to the main pulmonary artery, and the lower one represents the left ventricle (Fig. 6). In my opinion, the aortic knob and pulmonary artery arch should be included in the checklist.
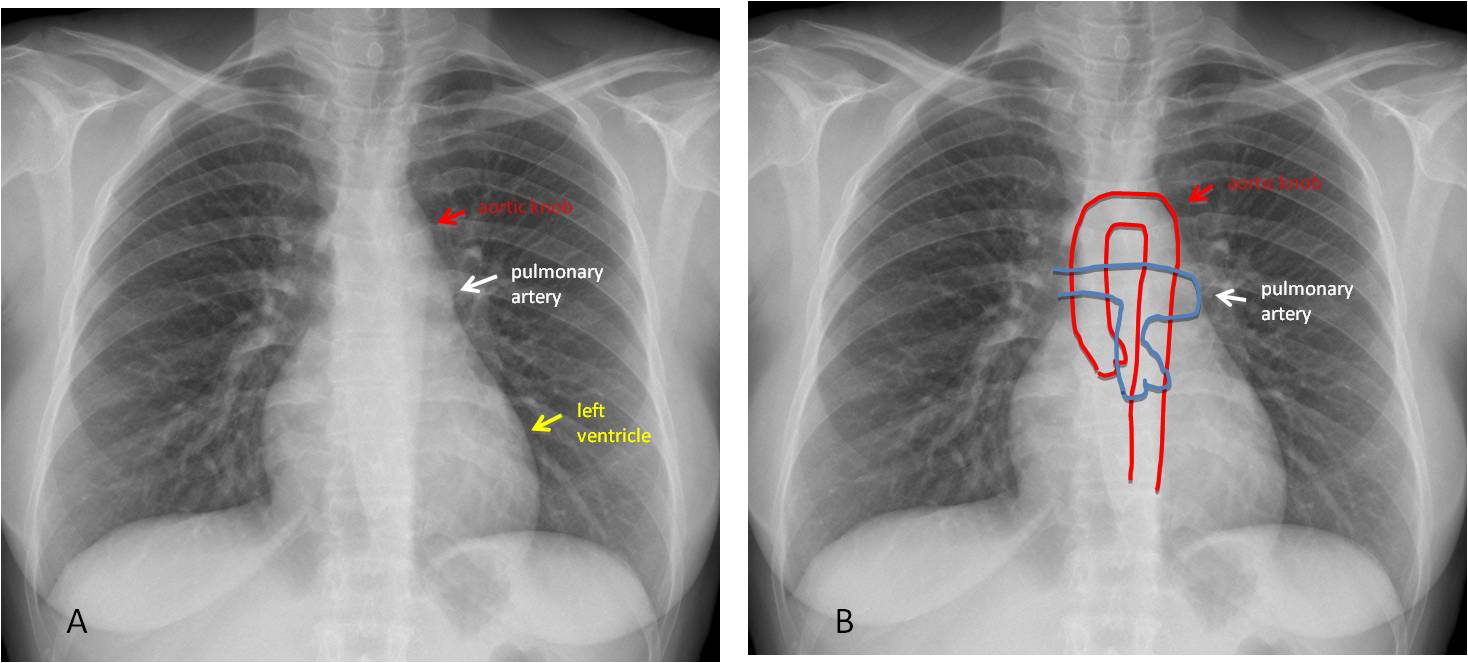
Fig. 6
Fig. 6. Normal chest films (A and B) showing the three components of the left mediastinal border.
The aortic knob should be examined in every chest radiograph. The most obvious finding is a change in size. The knob increases in size with aging, but a large aortic knob in a relatively young person should bring to mind an aneurysm or a type B dissection (Fig. 7).
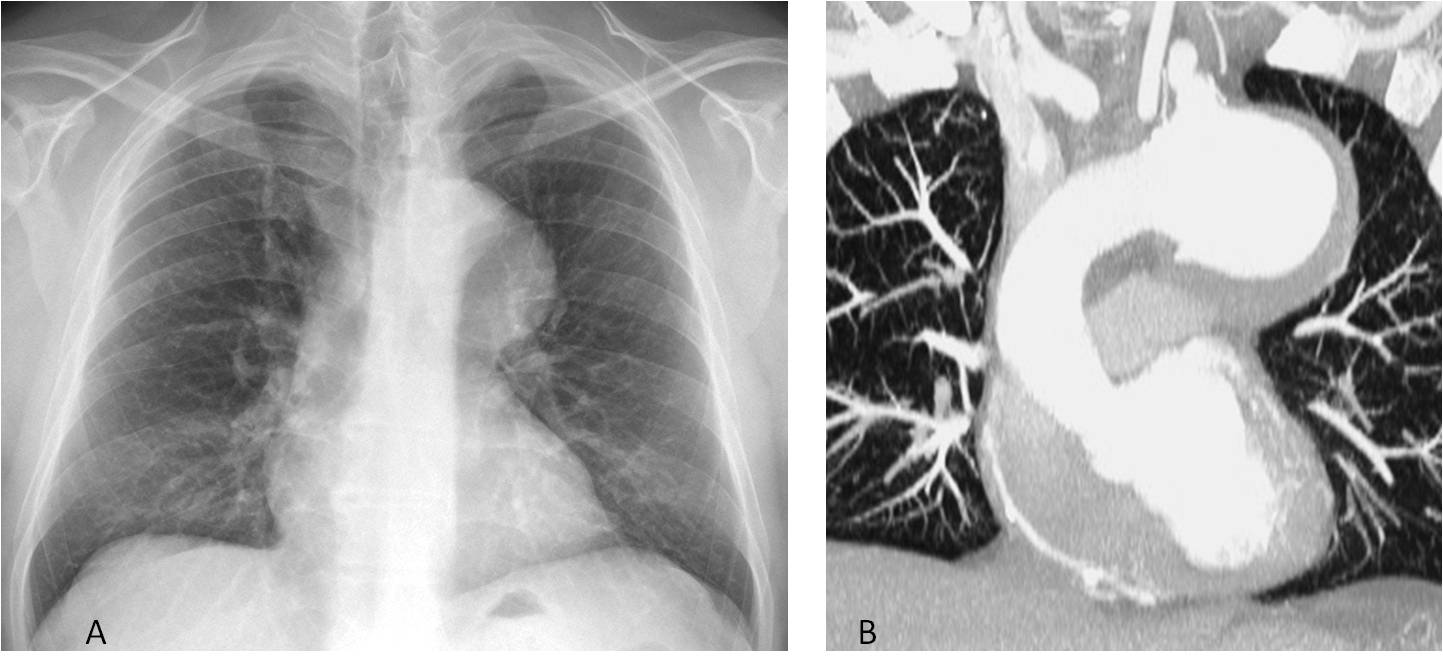
Fig. 7
Fig. 7. 54-year-old patient with a large aortic knob (A, arrow). Enhanced coronal CT confirms an aneurysm of the aortic arch (B, arrow).
In my experience, one of the most common causes of a small left aortic knob in adults is a right aortic arch. This congenital variation is easily detected by recognising the knob at the right mediastinal border and detecting the imprint in the right tracheal wall (Fig. 8).
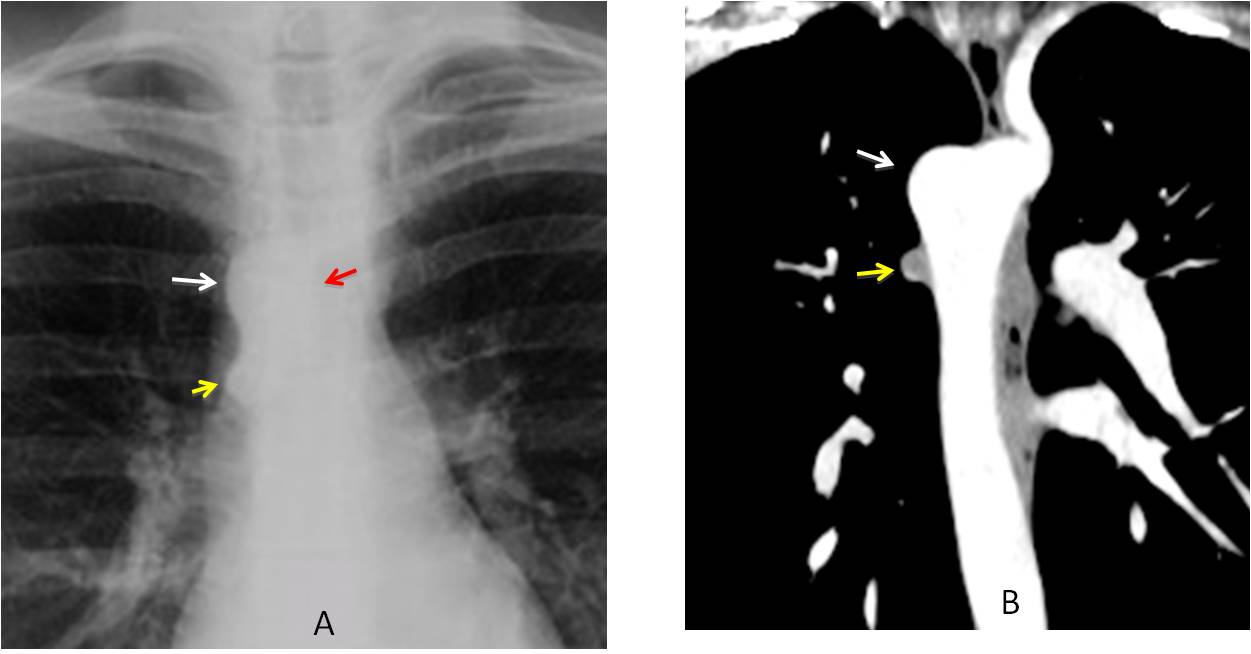
Fig. 8
Fig. 8. 27-year-old woman has no obvious left aortic knob; instead, the knob is located on the right side (A and B, white arrows). Note the imprint in the right tracheal wall (A, red arrow). The small bump under the right arch represents the azygos vein (A and B, yellow arrows).
Occasionally, a small mediastinal mass may hide behind the aortic knob, and careful inspection is needed detect it (Fig. 9).
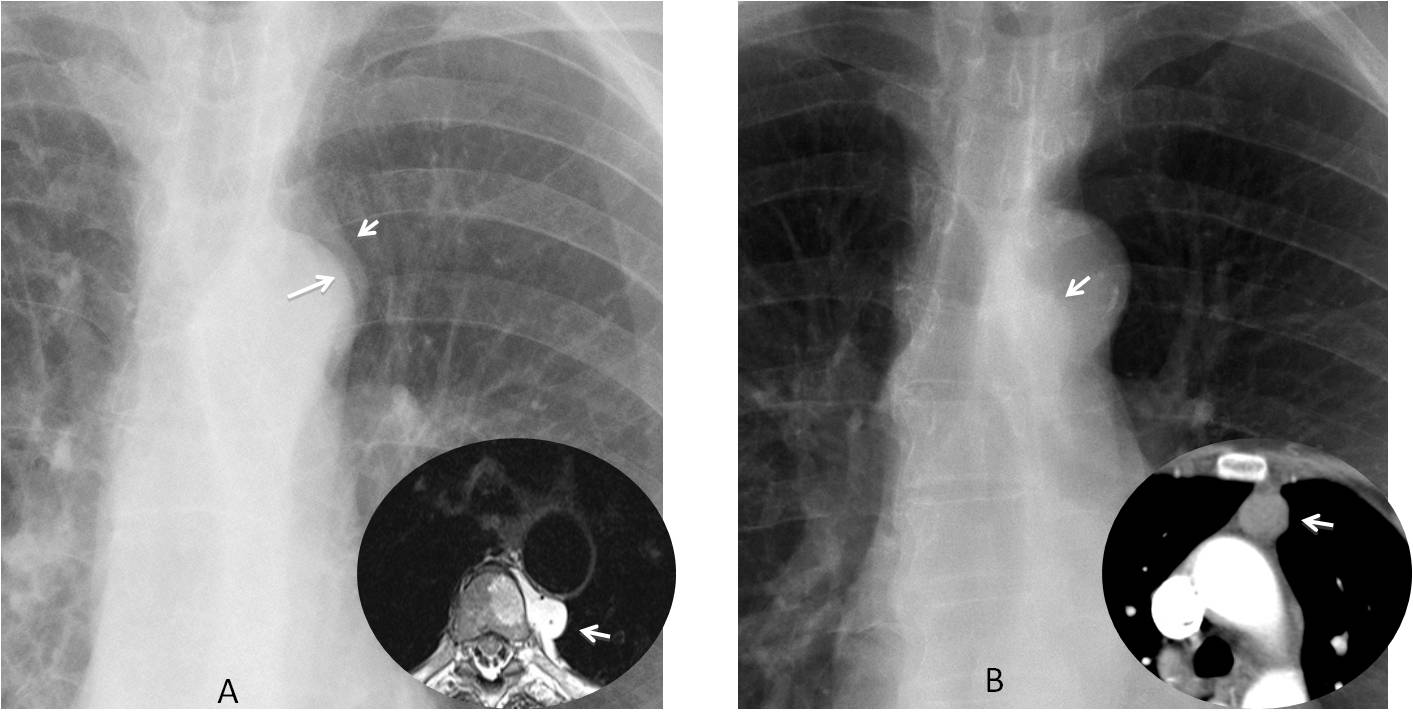
Fig. 9
Fig. 9. A: Control radiograph in a patient with leg sarcoma. The aortic knob shows a double contour (A, arrows). Axial MRI confirms a metastatic mass invading the spine (insert, arrow). In another patient, a small mass is seen through the aortic knob (B, arrow), confirmed with CT (insert, arrow). Diagnosis: thymoma.
Bulging of the pulmonary artery arch usually indicates dilatation of the main pulmonary artery, which can be caused by 3 conditions. The most common is pulmonary arterial hypertension, followed by left-to-right shunt and pulmonary valve stenosis (Fig. 10).
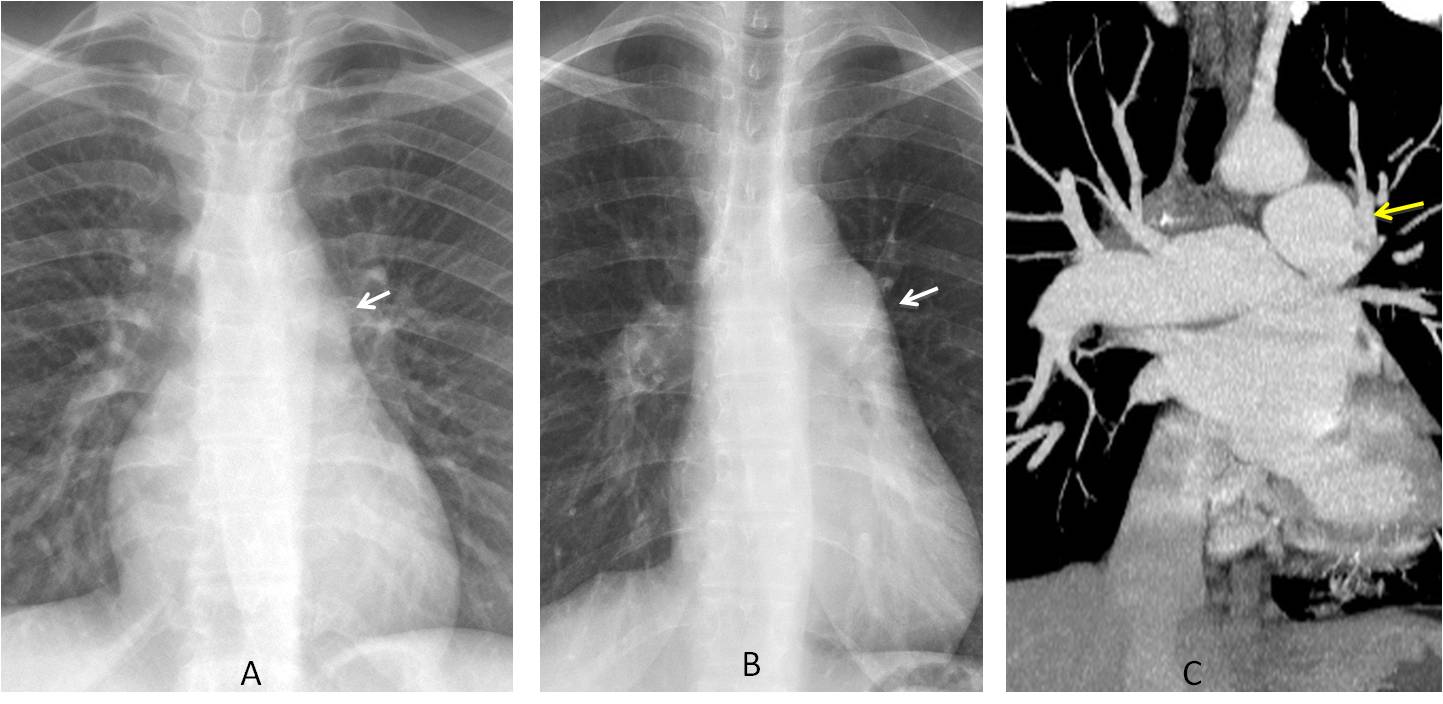
Fig. 10
Fig. 10. A: Normal pulmonary artery arch (A, arrow). B: Bulging of this segment in another patient (B, arrow). Coronal enhanced CT shows enlargement of the main pulmonary artery (C, arrow), which is wider than the aorta. Diagnosis: pulmonary arterial hypertension
In conclusion, the following mediastinal areas should be investigated in the PA view:
The paratracheal line, to evaluate changes in width usually due to enlarged lymph nodes, and the paraesophageal line, which may be displaced by esophageal dilatation, enlarged lymph nodes, or congenital cysts.
The azygos vein. Enlargement is usually due to thrombosis of the superior or inferior vena cava.
The ascending aorta. Enlargement can be due to bicuspid aortic valve, ascending aorta aneurysm, type A aortic dissection, or aortic coarctation
The aortic knob, to detect changes in size and, occasionally, hidden mediastinal masses.
The pulmonary artery arch. The most common cause of prominence is pulmonary arterial hypertension.
Next week I will continue with further checklists.

Follow Dr. Pepe’s advice:
1. The mediastinum checklist includes mediastinal lines and bulges of the outline.
2. The main lines to examine are the paratracheal line and the paraesophageal line.
3. On the right mediastinal contour, look at the azygos vein and ascending aorta.
4. On the left mediastinal contour, look at the aortic knob and pulmonary arch.


Hello.
I think there is mild elevation of the right hilum, thickening of the right paratracheal stripe and a triangular shaped opacity in the right upper lung field best seen on profile. These findings are probably due to volume loss of the right upper lobe, or at least one segment of this lobe.
I believe the triangular opacity in the lateral view is due to the soft tissues of the armpit. Note how the anterior line goes out of the lung.
Left breast implant.
There is a subtle hyperlucency of the LUL, and an asymmetry between both breasts, because of surgical changes.
I can see an increased vascular right hilum.
…..professore stimatissimo……dove. è’ l’arco anteriore della 5 costa di Sx ?….la patologia è’ una probabile metastasi litica ….un augurio per il tuo Barca che non decolla…..il mio Bari ha ancora perso…..un grande saluto…
Ribs are OK. The problem with high-KV images is that the bones are burned out (like Barça!)
…mediastinite fibrosante post-radioterapica ?’
Oval hyperlucency in the posterior right 8th rib. Also round hyperlucencies in the 8th and 11th thoracic vertebra. The right hilum also appears slightly elevated.
The left upper lung zone appears slightly more lucent compared to the right. I also noticed a round focal lucency between the 7th and 8th left posterior ribs.
Lucencies may be due to superimposition of scapula. There were no bone lesions.
There seems to be widening of the upper mediastinum on the right side appearing as a soft tissue density. May be associated with enlarged mediastinal lymph nodes.
Now you are using your knowledge! 😉
Dear my Prof, how can we distinguish the widening of right paratracheal from real lesion to widening of SVC, especially in rotation patient, I always worry about variant in rotation patient, more important when we have a CXR with wrong technique, low KVp. Thanks
Right upper paratracheal líne is thickened, perhaps because of mediastinal lymph node secundary to breast neoplams
And right hilar adenopathy
Dear dr Pepe, according to your previous lecture, we can say that both hila are the same density and lay on the same level so they are normal. Both main bronchi have a proper angulation.
There is no hidden masses in apices and in costophrenic angles.Mediastimum isn’t widened, nie fluid in both c-p angles. Bones have low density probably because of anti estrogenic theraphy, but no signs of maetastatic disease. Round opacity at the level of Th8-Th9 is probably the scapula’s angle.
I would say it’s normal
I believe showing a normal chest
insults the audience. Believe me, the chest ain’t normal;-)
The left upper(AP) and lower(Lat) hyperlucencies are probably due to prior surgery.
Both the right paratracheal and left apical shadows look within normal limits.
Cant really see added hilar opacity in the lat view.
So will have to say normal images.
One of your statements isn’t true…
Micronodular spread
Left inferior lobe nodule pa-retrocardiac ll-projects over the dorsal body
there is sight hyperlucency of left hemithorax probably post surgery.
Some of the thoracic vertebrae show hyperdensities. Comparison with previous and follow up X-ray’s required to rule out Mets Vs being lesion
widening of the upper mediastinum and two small nodules in Lateral view
There is small nodular opacity on lateral view on the level of thoracic vertebrae
This opacity is near the vessels.
And in lingular segment it seems to be also opacity, which join with heart shadow
A little bit higher above that small opacity on the vertebrae level, there is bigger opacity which is connected with vessels
normal
I never show a normal film, although this one seems normal. Use your checklists
Round lucency Rt hilum?
Lateral view – abnormal opacity in subcutanneous tissue, at upper part of sternum.
right hilum at the same level as left?
Right paratracheal line is thickened (enlargment mediastinal lymph nodes?), and on the lateral view behind the heart (at the level of Th9/10) is round opacity, probably vessel but it also could be metastatic nodule, so CT should be performed:)
Left hilar increased density with lobular outline, may represent hilar lymphadenopathy or medially located lung nodule
Before the answer is posted I want to congratulate MK, who saw the abnormality and made a correct evaluation.
…grazie Professore per la bellissima lezione !
Thank you. I believe this case emphasizes the importance of checklists. And of playing well against Real Madrid 😉
Beautiful presentation thank you
Glad you like it. Thank you
Excelente trabajo. Muchas gracias profesor.