I am spending few days near Barcelona and, of course, I had lunch with my friend José Caceres, master of the blogs. José ( and the Muppet) advised me to show you this case, so here it is.
This is a case that will test your ability to integrate the findings. Lets see…
56-year-old woman who has persistent cough.
Dear Friends, some of you saw the pulmonary infiltrate and thought of Pneumonia, but obviously, and especially having to share it with José Caceres and the Muppet, I had to make the case a little bit harder…
Let us see the findings.

The PA chest radiograph shows a right thoracic opacity with an air bronchogram as small branching tubular structures (white arrow). The presence of air bronchograms indicates that the pathology is in the lung, and involves the alveolar space. Pneumonia is a good choice, but since there are no signs or symptoms related to an infection, other diagnostic possibilities should be considered.
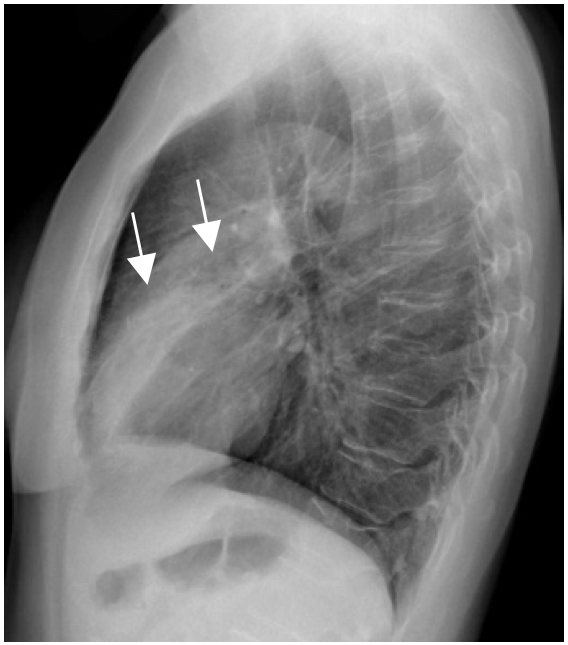
In the lateral radiograph the consolidation is in the middle lobe, well limited posteriorly by the major fissure, but the minor fissure is not displaced. The upper limits of the consolidation are poorly defined (white small arrows), indicating, as in the air bronchogram sign, the air space nature of the pathology.
And now, the clue: If you look carefully at the PA image, you will see that there is no right breast. In this case you can suspect that the pathology could be related to breast cancer. A look at the clinical history informs you that this lady has had radiotherapy to the right hemithorax.
Pulmonary changes after radiotherapy occur as Fibrosis and pneumonitis that commonly involve the radiation field area. The other cause of pulmonary infiltrates related to Radiation Therapy is Organising pneumonia which was the cause in this case of the pulmonary opacity. Organising Pneumonia may occur after radiotherapy. The infiltrates may be in areas not exposed to the radiation field, may be migratory and even occur long time after the treatment
A CT (One month before) showed multiple parched pulmonary opacities, some of them had the “Inverted halo” or “Atoll” sign so characteristic of Organising pneumonia. (Red Arrow).
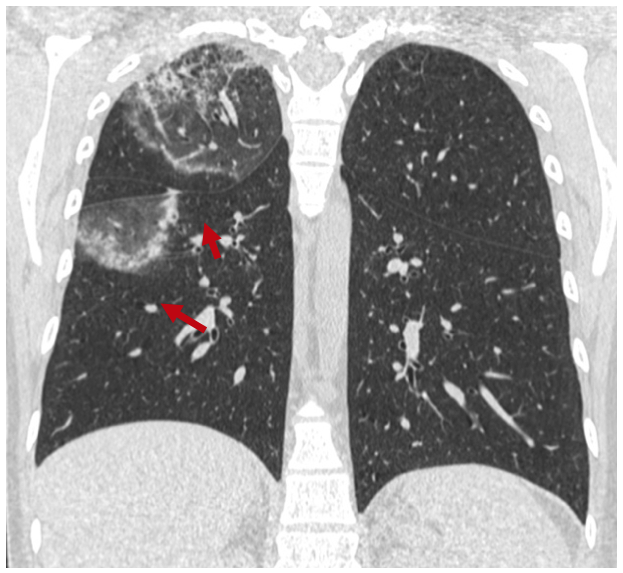
Chest CT, coronal with lung window settings: Two large areas of Organising Pneumonia are seen as curved dense areas with ground glass density within them. ( Inverted halo).
CONCLUSION:
- Always look for any additional information present in the images.
- Think of Organising pneumonia if the patient has had radiation therapy to the thoracic region (Breast, Lungs, Mediastinum).




Pneumonia in the Middle lobe
Middle lobe consolidation
Rt Middle lobe consolidation with collapse
Pneumonia is a possible diagnosis, but the patient had no fever or other symptoms of infection. Any other possibilities?. Do you see any additional finding that could help?.
I think that an Atelectasia of the middle lobe can be another option.
There is a displacement of the minor and oblique fissures of the right lung in the PA and lateral films.
There is a elevation of the right diaphragm too.
In fact, the defined density abulting the right heart border
pneumonia with air bronchogram sign seen in the rt middle lobe with partial volume loss, the oblique fissure moving forward.
the minor fissure is seen in frontal projection. there is also pneumonic patch in the ant segment of upper lobe. there is also ectasia of bronchiole aroud the rt hilum.
right mammary shadow not seen
there is suggestion of widening of pedicle of d 10 vertebra in lat view.
probably a case of ca breast with mastectomy with radiation pneumonitis
Radiation pneumonitis