Dear friends,
Thank you for joining. The last case was a warm up. This one is a little bit more complicated but I know that you will be able to help me with the diagnosis.
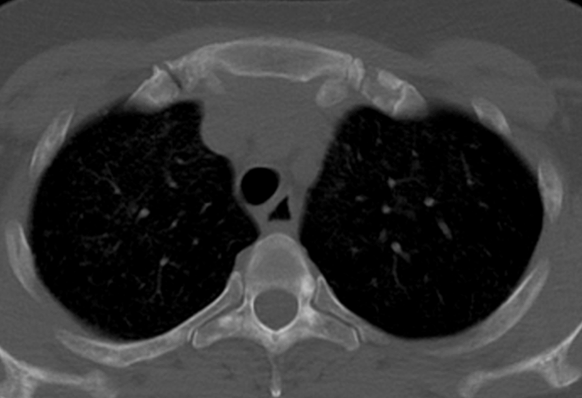
This is a 54 year old woman with long standing renal disease.
What do you think?
Check the image below, leave your thoughts in the comments section and come back on Friday for the answer.





Click here for the answer
The following findings are shown:
1- Multiple pulmonary nodules with a random distribution and few lung cysts (yellow arrows).
2- Large kidneys with multiple cysts
3- In the CT, Bone window settings small sclerotic areas are seen in the vertebrae. (red arrows)
Diagnosis: Multifocal pneumocyte hyperplasia in tuberous sclerosis
Comment: The patient had Tuberous sclerosis with renal cystic disease (no angiomyolipomas in this case). Pneumocyte hyperplasia occurs in tuberous sclerosis as another expression of the disease in with multiple hamartomas are present in different organs including bones (sclerotic lesions)-
Pneumocyte hyperplasia may coexist with lung cysts in some cases. IN our case there were few cysts (yellow arrows), but the nodular pattern was predominant.


Two teaching points:
1- Look at the bones when suspecting tuberous sclerosis.
2- Yes: multiple random pulmonary nodules may be present in Tuberous sclerosis.


{kind=link}
Multiple reticulonodular tiny opacities with few bony sclerotic lesions and enlarged cystic kidneys – Aquired cystic renal disease with infectious bronchiolitis
Small difuse dense (calcified) nodules in a patient with polycystic renal disesae, osteopenia and rugger-jersey spine. no evidence of lymphadenopathy.
I would go for metastatic pulmonary calcification and renal osteodystrophy. Milliary calcifications are also possible. TB milliary disesae is less likely in the abscence of adenopathy.
Multiple centrilobular nodules
Pulmonary oedema and pulmonary hypertension due to renal failure
Hello
Multiple centrilobular nodules without lobar predilection. Mild subpleural sparing. Enlarged kidneys containing multiple cysts.
Has there been a renal transplant? Subacute hypersensitivity pneumonitis secondary to immunosuppressant medication?
Good morning!
In the x-ray and CT there are multiple bilateral, diffuse and randomly distributed micronodules. In the osseous window there are some blastic lesions and in the abdomen there is a policystic renal disease. I am thinking about hyperparathyroidism.
Greetings,
on the CXR, a coarse reticulonodular pattern can be seen without volume loss, which was confirmed by CT, the kidneys appearance is consistent with autosomal dominant polycystic kidney disease.
considering the history and radiographic appearance I would consider a drug-induced interstitial lung disease.
You guys are getting close but not completely. The case is quite difficult as you will soon se, but I believe that theres is a teaching clue…
Hello,
Probably the lung and bone changes can be explained by amyloidosis secondary to the chronic kidney disease.
Cheers!
Look at the bone window settings in the chest CT. Does it help?
Greetings,
I was wondering… would it be possible to get another images with bone windowing? I am not quite sure what we can see in this one. It looks like multiple small sclerotic lesions that are found in patients with tuberous sclerosis, however, with one scan only I do not feel very confident about this differential.
Thank you 🙂
Hello
on the thoracic X-ray and CT there are multiples multifocal micronodules centrolobulaires.In bone window some sclerotic bone lesions. In the abdomen there is an aspect of polycystic kidney disease. I think of tuberous sclerosis.