José Vilar and Friends Case 35 (Update: Solution + Teaching points!)
Hello Friends.
This patient is 42 years old without significant respiratory symptoms.
Hello Friends here is some help.
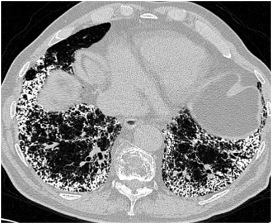
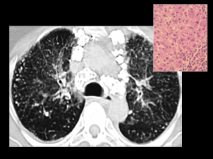
Here is a CT image. Diagnosis?
Click here for the answer
Hello Friends.
Congratulations to some of you who got the case correctly.
Let’s review it:
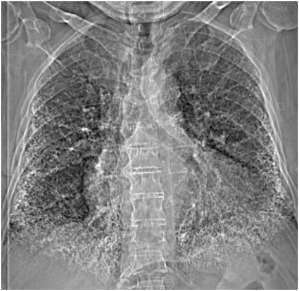
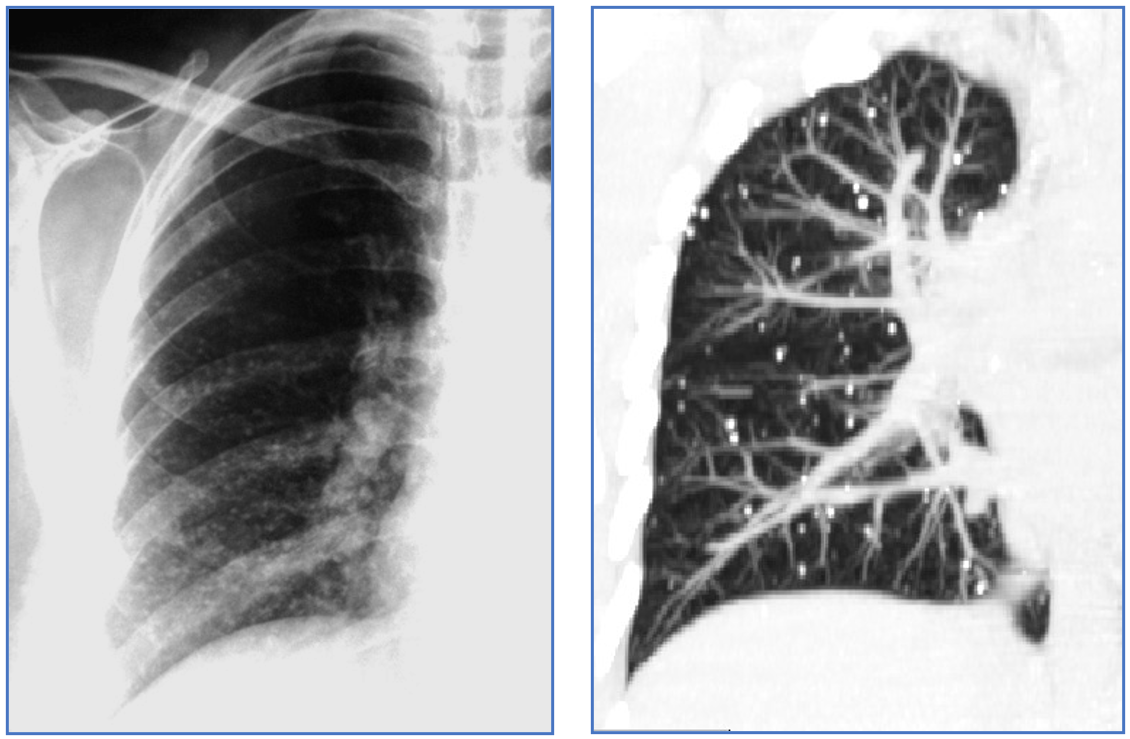
The original image shows innumerable calcific densities in both lower lung fields.
I added another image: A CT that confirms the presence of multiple calcifications in both lower lobes. The calcifications are millimetric and seem to spare the pleura. These are typical findings of Alveolar Microlithiasis.
The principal characteristics of Alveolar Microlithiasis are:
- Calcific concretions in the alveoli
- Familial disease
- Poor prognosis that may end up in lung transplantation
- More frequent in women
- Appears in the second decade of life
- It is more common in Turkey.
The most important imaging findings are:
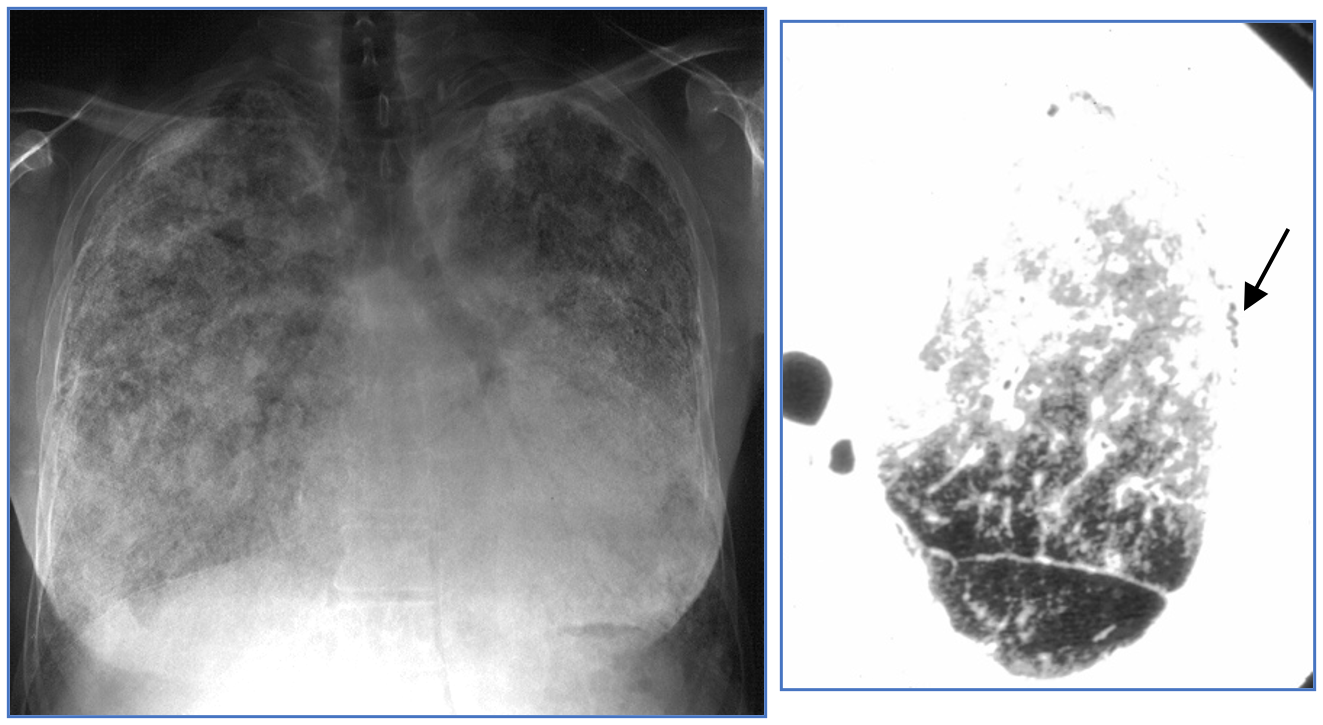
- Chest XR:
- “Snow storm” pattern: white lungs.
- Dark pleural line: ( Arrow)
- CT:
- Ground glass, generally diffuse.
- Multiple small calcifications in alveoli.
- Subpleural cysts ( Responsible for the black pleural line in CXR)
- Pulmonary fibrosis
- Pleural calcifications.

- MRI:
- High signal intensity in T1.
- NM:
- Uptake of Gd 99m diphosphonate.
Differential diagnosis: The presence of multiple, diffuse calcifications in the lungs raises some other diagnostic possibilities:
- Metastatic calcifications (due to altered levels of calcium) ( Renal insufficiency, Hyperparathyroidism)

(Courtesy of Tomas Franquet MD).
- Healed Varicella Pneumonia (Fewer calcifications, asymptomatic)
- Silicosis. (Usually presents with additional findings such as adenopathy in this case).
- Pulmonary ossification in chronic mitral disease (Chronic pulmonary venous hypertension).

In most of these cases the clinical information will clearly help in the diagnosis.
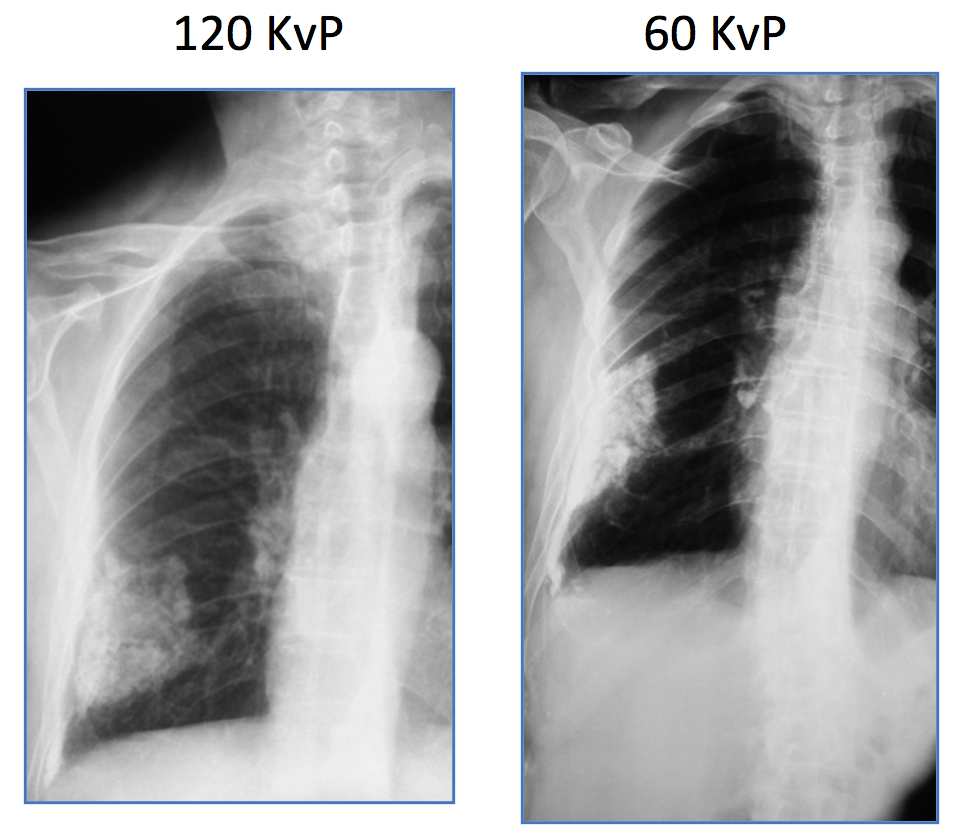
One last question: Why is it so difficult to see these calcifications in the chest radiograph?
Answer: Because we use high kvP in regular CXR . A low KvP ( such as the one we use to detect rib lesions) would enhance calcium due to photoelectric effect as you can see in this case (Pleural plaque).


Se ven opacidades reticulares subpleural a predominio basal, parece dentro de los patrones de alta densidad. Se me ocurre una osificación pulmonar difusa por sus caracteristicas. Se que se asocian mas a intersticiopatias fibrosantes con patron de UIP, lo que me hace dudar es que es joven y asintomatico. Patrón restrictivo en los funcionales respiratorios?
Bilateral interstitial thickening and multiple tiny calcifications throughout both lungs predominantly affecting lower and mid zone peripherally more than centrally, this appearance along with the history of no respiratory symptoms – pulmonary alveolar microlithiasis is the diagnosis.
tiny calcification distributed throughout the lungs,bilateral with middle to lower zone predilection.
Normal lungs volume.
no evidenced of pleural effusion.
cardiothoracic ratio is mildly prominent.
In patient without respiratory symptoms, i would suspect pulmonary alveolar microlithiasis.
ddx: pulmonary hemosiderosis.
PAM(Pulmonary Alveolar Microlithiasis)
Symmetrical linear reticular calcifications are seen predominantly in both lower lungs could be pulmonary alveolar proteinosis ( quite sharp and well defined due to alveolar pathology) in contrast to metastasis calcifications that prone to be more ill defined due to interstitial pathology
Pulmonary alveolar microlithesis***