José Vilar and Friends Case 38 (Update: Solution + Teaching cases)
Hello everybody. Are you ready for another case?
This is a case that was provided by Drs Isarría and García Dosdá from the Radiology Dept. Hospital Universitario Dr. Peset. Valencia.
This patient is a lady 78 years old with suspected eventration. In her workup she had a Chest Radiographic examination and an abdominal CT.
Please look carefully at the images. The case is not easy, but I believe that it contains some teaching points…




Where is the pathology?
Additional images:
As I see you have not been able to identify the pathology. Don’t worry. This case was missed also by the radiologist until almost two years later. In this occasion the patient was dyspneic and not feeling too well.
Looking at these images, can you identify where the original lesion is?

The updated information will be up until Friday 11th. Please check back for the solution on that day to see if you identified the original lesion correctly.
Click here for the answer
Hello everybody. Are you ready for the answer to case 38?
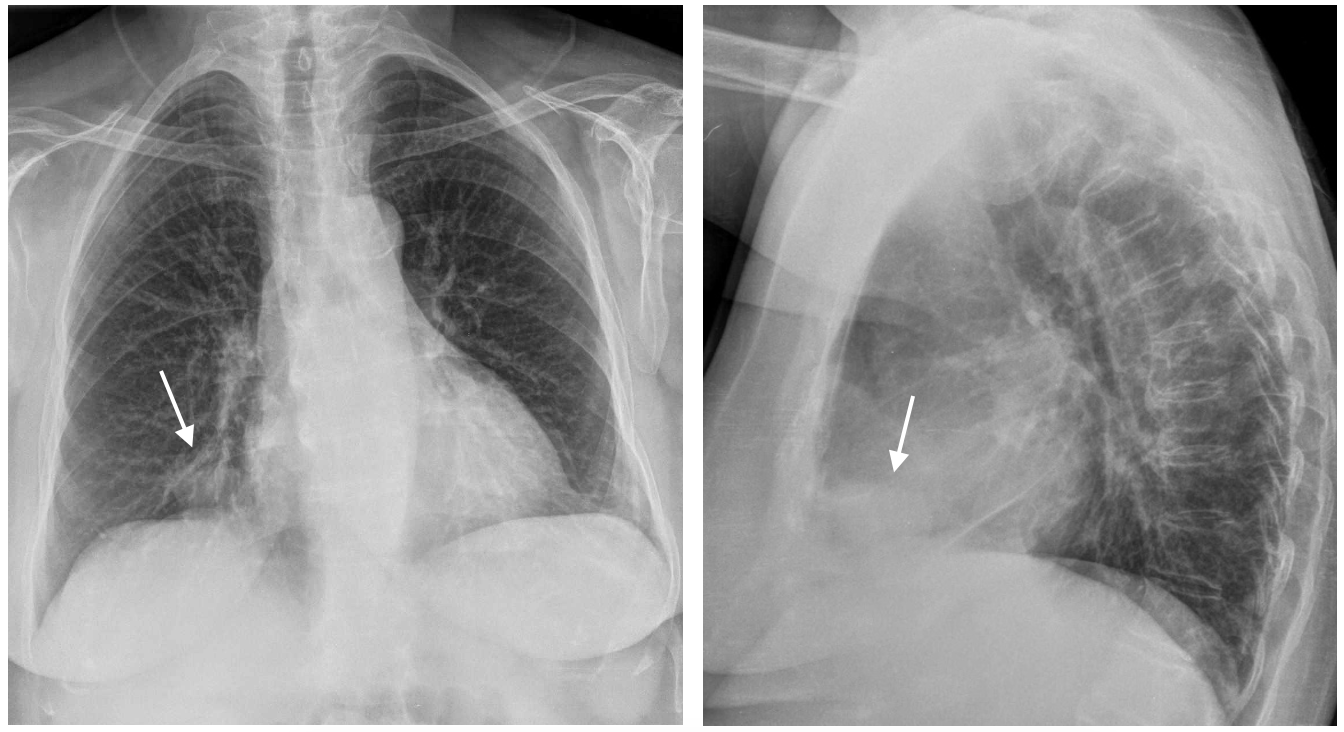
The chest radiographs show a subtle density near the right cardio phrenic angle in both PA and Lateral projections ( Arrows).
Right cardio phrenic angle lesions are most of the time not significant, the main differential diagnosis is between, fat, pleuro-pericardial cyst or Morgagni hernia. In those cases fat, fluid or even air could be present.
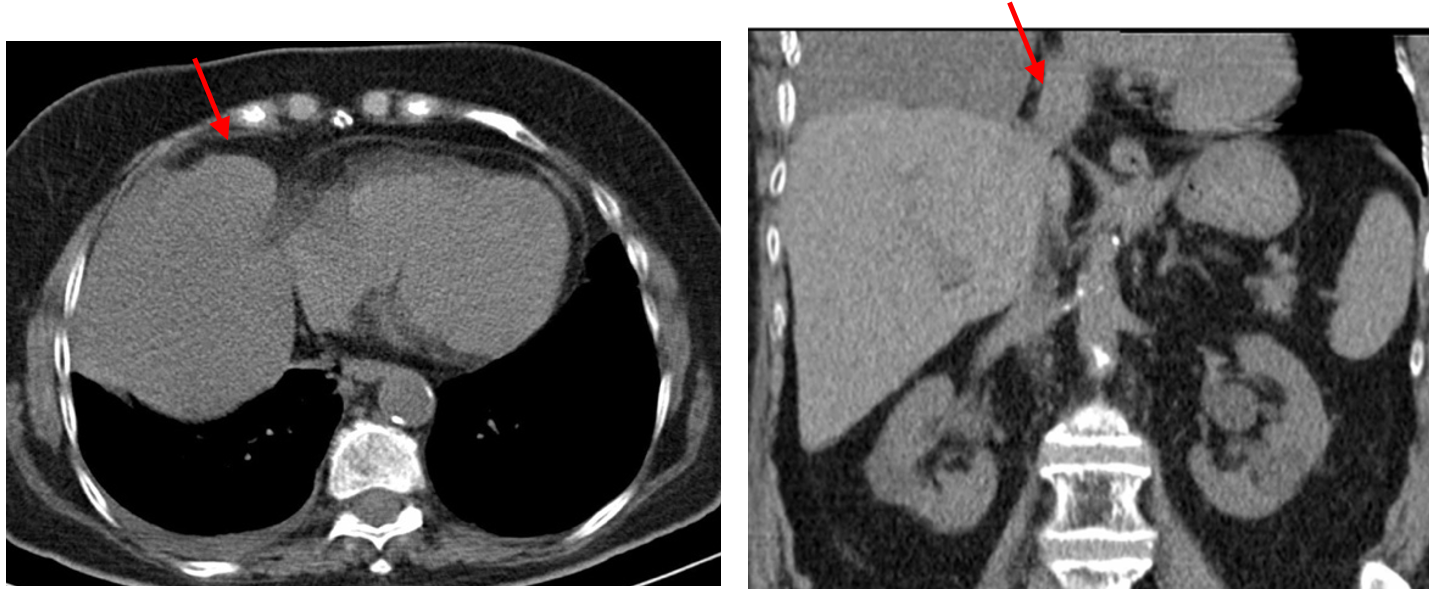
If you look at this non contrat CT that was performed for abdominal problems, there is a solid lesion next to the liver that coincides with the roght cardiophrenic angle image. This lesion was overlooked in this CT, an error that is not uncommon if you do not confront all the images (chest and andomen).
Therefore a lesion was missed in the initial study, and only after almost two years the nature of that lesion was not discovered. A Large thoracic mass with pleural effusion.

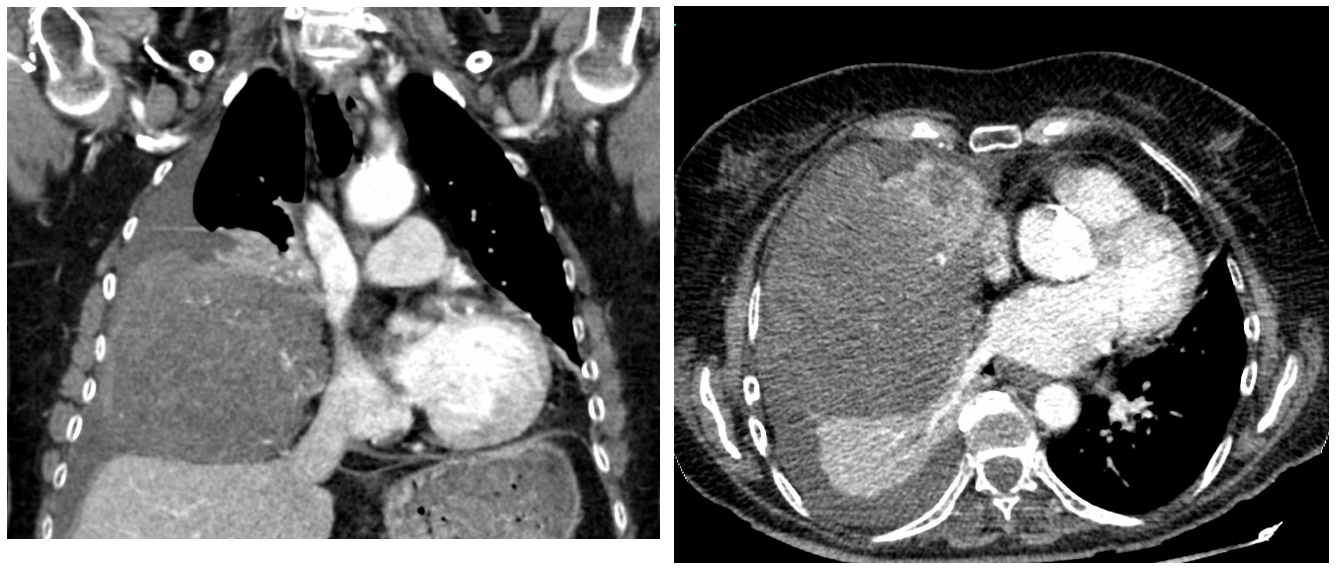
There is a large heterogeneous mass compressing the lung, and displacing the mediastinum. No infiltration of the diaphragm or mediastinum is seen. Thus, the mass has extrapulmonary characteristics and suggests a pleural origin.
A biopsy of the mass revealed that it was a solitary pleural fibroma.
Pleural fibroma constitutes 5% of pleural tumours. They present as masses, more commonly in the middle or lower thorax. Fibromas may associate hypoglycemia (2%) and pleuro-pulmonary osteoarthropathy (20%).
In CT fibromas are usually homogeneous and have contrast uptake.
Pleural fibromas may be malignant. Radiologic signs of malignancy are large size (above 10 cm), infiltration of near structures, necrosis and pleural effusion. Mitosis and cellularity are also indicators of malignancy.
Our case was considered malignant due to the large size and the non-homogenous uptake despite the fact that the number of mitosis was low. ( Below 10).
Teaching points:
This is a hard case, but it shows some important facts aside from the rareness of the tumour.
- Look carefully at PA and Lateral and remember the cardio phrenic angle.
- Analyze all the images and look at all the “corners” because often the answer is there. (The initial CT was the clue in this case).
- Regardless of your subspecialty (abdominal or chest radiology) the patient is the same, therefore lesions in the transition zones, such as this one, must be analyzed fully by the radiologist taking care of the patient.


excellent case