José Vilar and Friends Case 39 (Update: Solution + Points to remember!)
Hello everybody,
welcome to the new year 2021! We all wish you a much better year, especially regarding the terrible pandemia and its consequences.
Here is a case from 2018 ( Dr. Edgar Lorente, Hospital Universitario Dr. Peset. Valencia) that I was reviewing recently. Let’s see what you think.
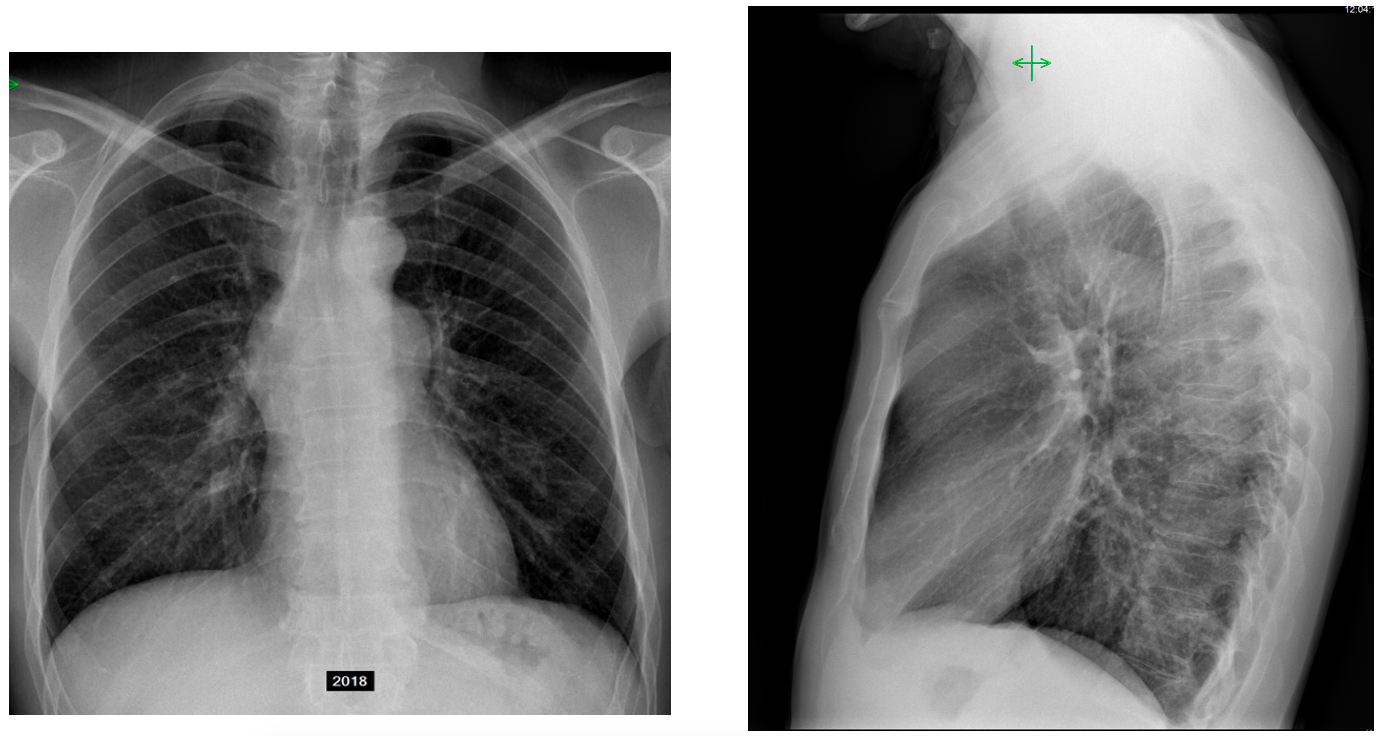
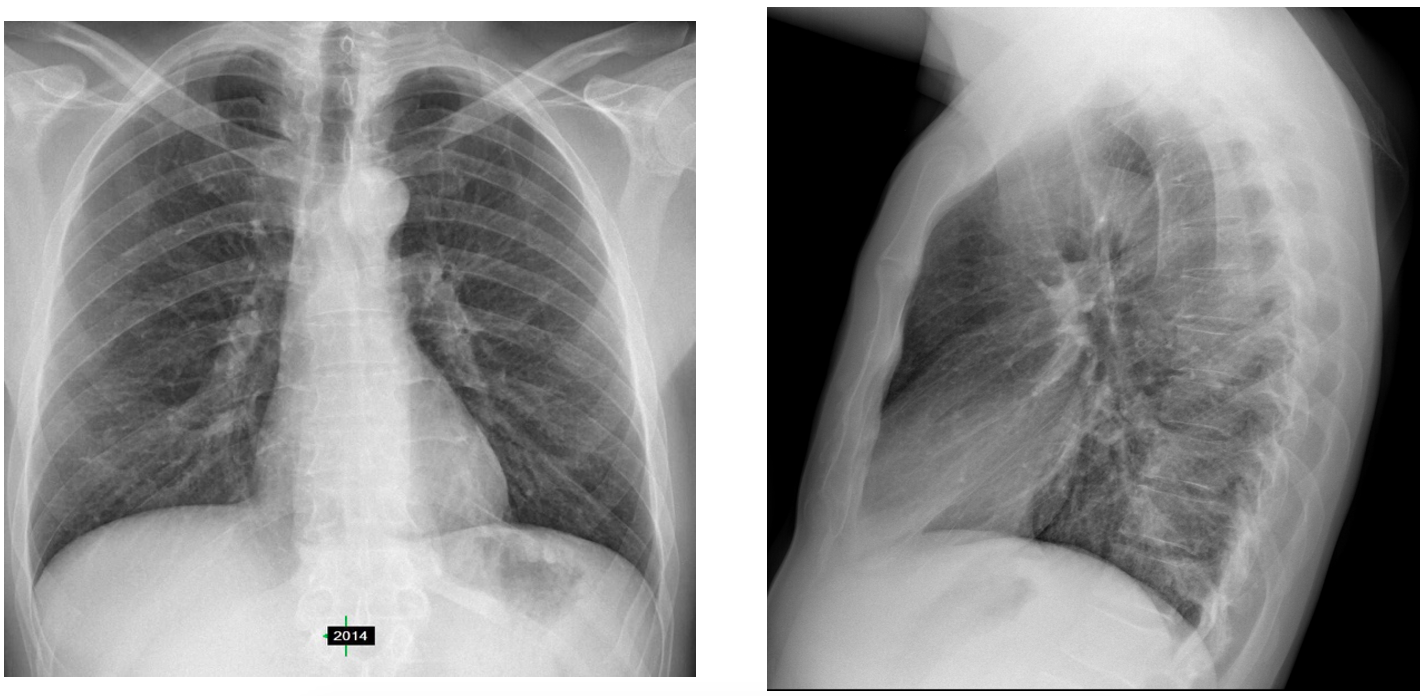
This is a 45-year-old male with long standing treatment for ankylosing spondylitis. I am showing you previous images from 2014 and the actual radiographs in 2018.
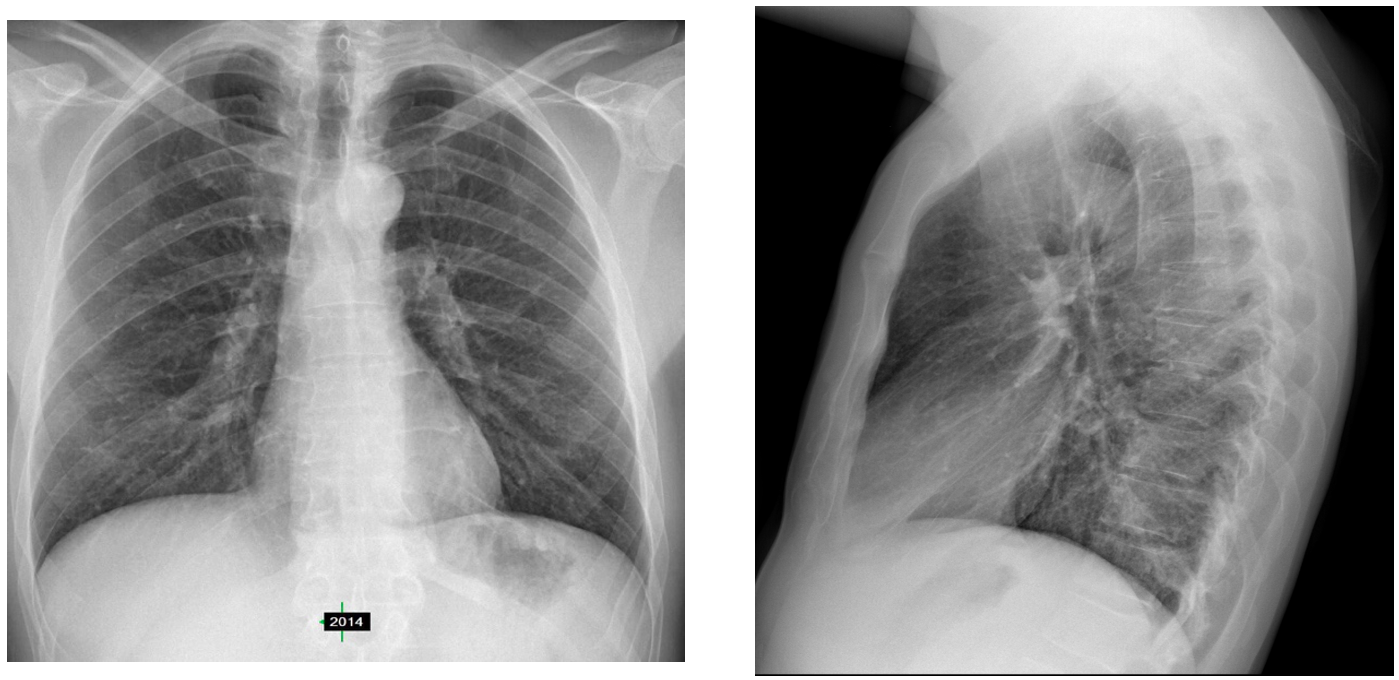
Where are the main findings and what is the probable diagnosis at this moment? Do you think that the lateral radiograph helps?
Click here for the answer
Hello everyone!
I must say that some of you were quite quick locating the findings and identifying the case as an anterior mediastinal mass.
- The main differential diagnosis is:
- Thymoma/Thymic carcinoma/Neuroendocrine tumours
- Teratoma
- Lymphoma.
- Thyroid should not be considered, especially since the trachea is not displaced.
You did well. Congratulations! This 2021 is looking good…
Let’s look at the findings.
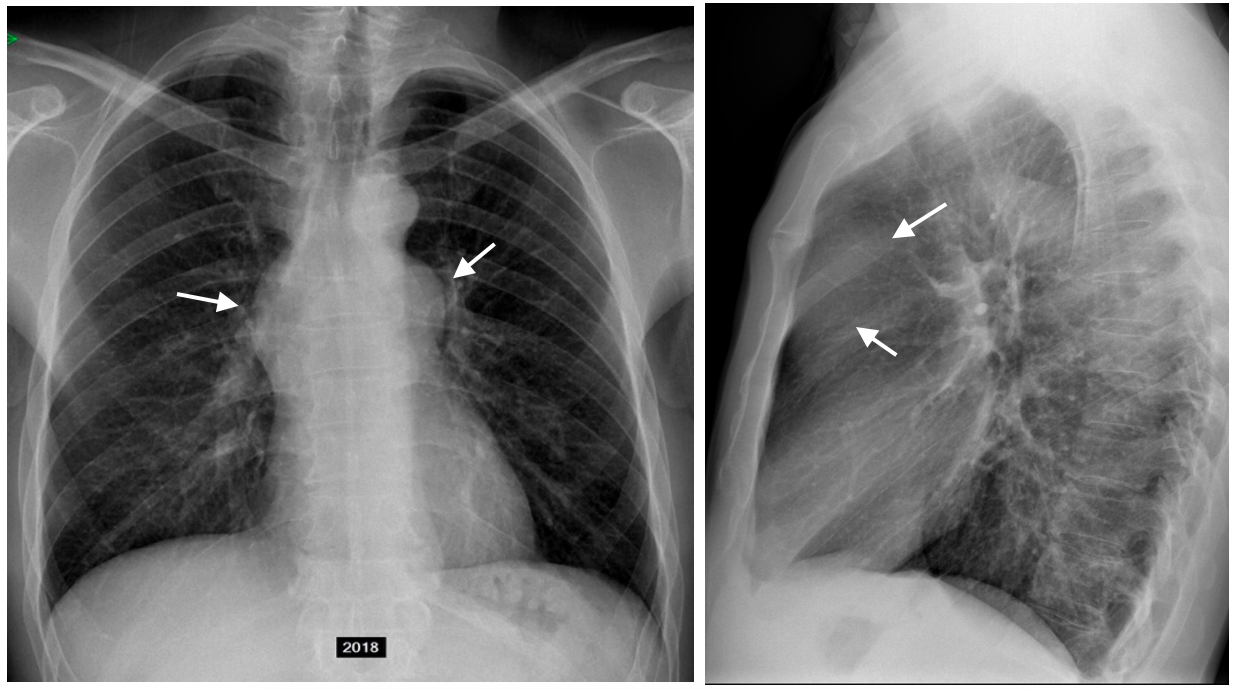
The radiographs from 2014 are normal and are excellent for comparing and seeing the main findings: In the PA you can see two convexities (arrows) indicating the presence of a mass in the mediastinum. The lateral projection is the clue: the lesion is very well seen in the anterior clear space behind the sternum, therefore the lesion is in the anterior mediastinum.
Chest radiographs are quite good for detecting anterior mediastinal tumours and other space occupying lesions, especially the lateral projection as you can see in our case.
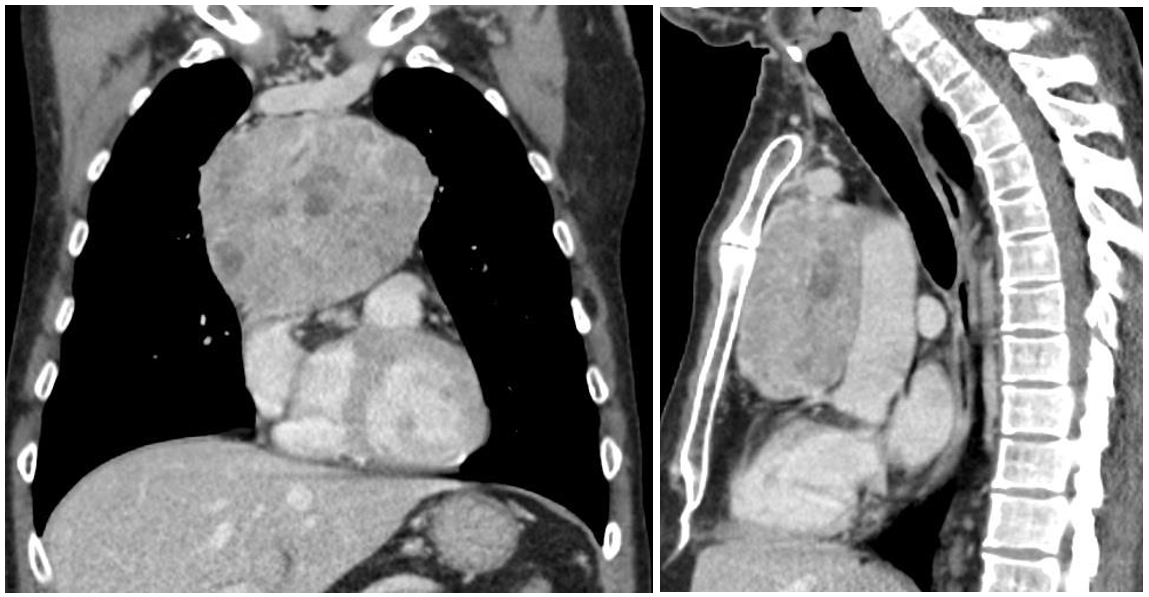
Once we find a possible tumour in the mediastinum, the next step is to see what it is. CT is the principal tool for this matter, although MRI could also be an alternative.
Contrast CT, coronal and sagittal projections showed a solid mediastinal tumour, well defined, with some hypodense areas of probable necrosis.
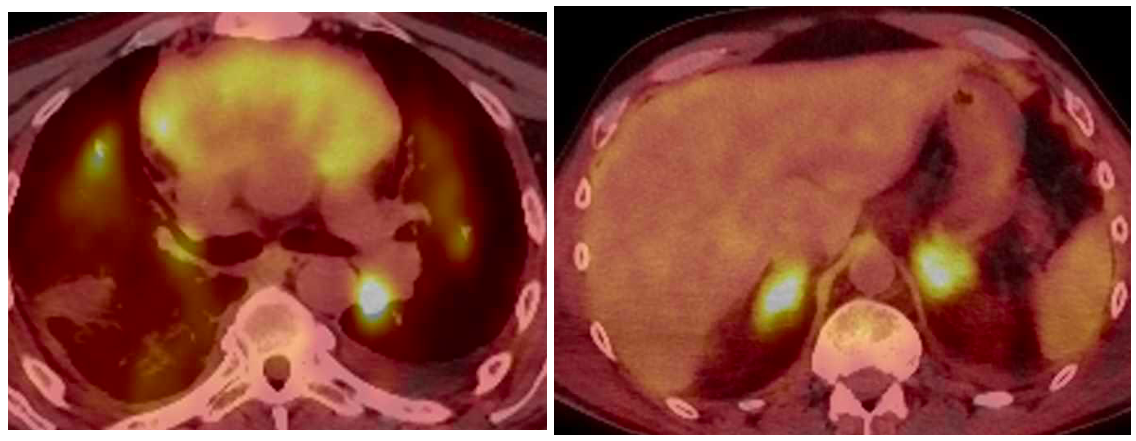
The biopsy of this lesion revealed that it was a Carcinoid (Neuroendocrine tumour). Staging was performed with PET/CT and SPECT/CT with somatostatin receptor.
In PET/CT metastases in both adrenals and the lung were detected.
Additional characterization of the tumour was made possible using somatostatin receptor SPECT/CT.
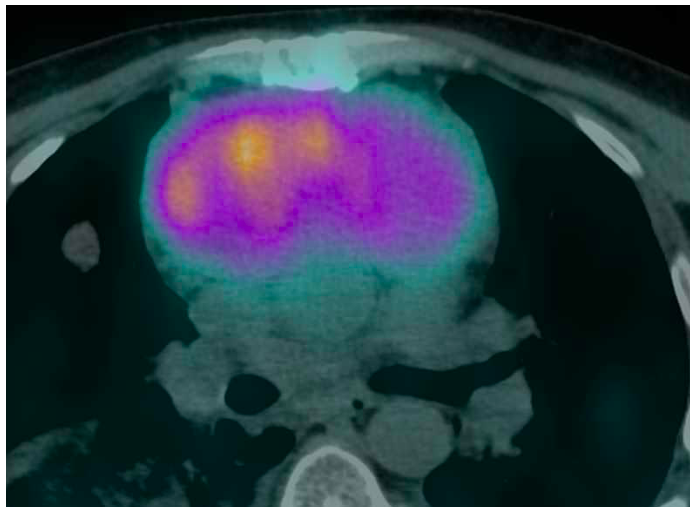
SPECT with 99mTc-Tektrotyd shows intense
signal in the carcinoid tumour.
No specific relation could be established with the ankylosing spondylitis.
Points to remember:
Anterior mediastinal masses are easily detected in lateral chest radiographs: look at the anterior clear space.
CT with contrast is the recommended technique to characterize mediastinal tumours. MRI is an alternative
Most anterior mediastinal tumours originate in the thymus, being Thymoma the most frequent one, but others, such as Lymphoma, Germ cell tumours, Thymic carcinoma and Neuroendocrine tumours also originate in the thymus.
Addendum: If you remember our CASE 24, you will see another Thymic neuroendocrine tumour and another good example of the value of the lateral chest radiograph.


Possible aortic root aneurysm due to aortitis
Reactive lymphoid hyperplasia
Linfoproliferative syndrom
Anterior mediastinal mass, most likely lymphadenopathy
Some of you are doing very well, approaching the diagnosis. Aside from lymphatic origin any differential diagnosis?.
As it in anterior mediastinum. Other than lymphatic ,thymal mass (thymoma, thymal cyst, thyilipoma),
Other possiblity acquired cyst e.g hydrated cyst
Teratoma another differential but no previous mass in old x-ray so it less likely
Retrosternal goiter (thyroid) less likely as no obvious soft tissue in front of trachea
Masa mediastinal anterior. Me gusta el diagnóstico de timoma/hiperplasia timica debido quizas a algún tratamiento por su enfermedad reumatológica. Más también por la edad 45-50 años timoma creo que es lo más frecuente…
Enlarged pulmonary arteries secondary to right heart strain caused by fibrosis secondary to AS.
Pulmonary hypertension. Enlarged hila, the pulmonary arch has a convex configuration and also some basal fibrotic bands.
Anterior mediastinal masses differential diagnosis with 5 Ts: thymoma, thoracic aorta, teratoma, lymphoma, thyroid. I don’t know which have thigh association with autoimmune spondylitis, I would say something inflammatory, like thyroid or aortitis though aorta looks normal to me in AP and it’s a little low for a thyroid. Therefore maybe thymoma or lymphoma are the more suitable.