José Vilar and Friends Case 48 (Update: Solution+Teaching tips!)
Hello friends, this time, my good friend and former Resident, Dr Lucía Flors sends me a case that fits perfectly with our line of interesting and teaching cases.
Dr Flors is presently at UCLA in Los Angeles as Associate Professor of Clinical Radiology with special dedication to thoracic imaging. She has already participated in this blog with interesting cases.

A picture some years ago when Dr Flors, to my right side, was finishing her residency at Hospital Universitario Dr Peset. To my left Drs Elena Lonjedo and José Martinez, excellent interventional radiologists actually in Valencia.
The case: This is an 84-year-old patient with acute chest pain.
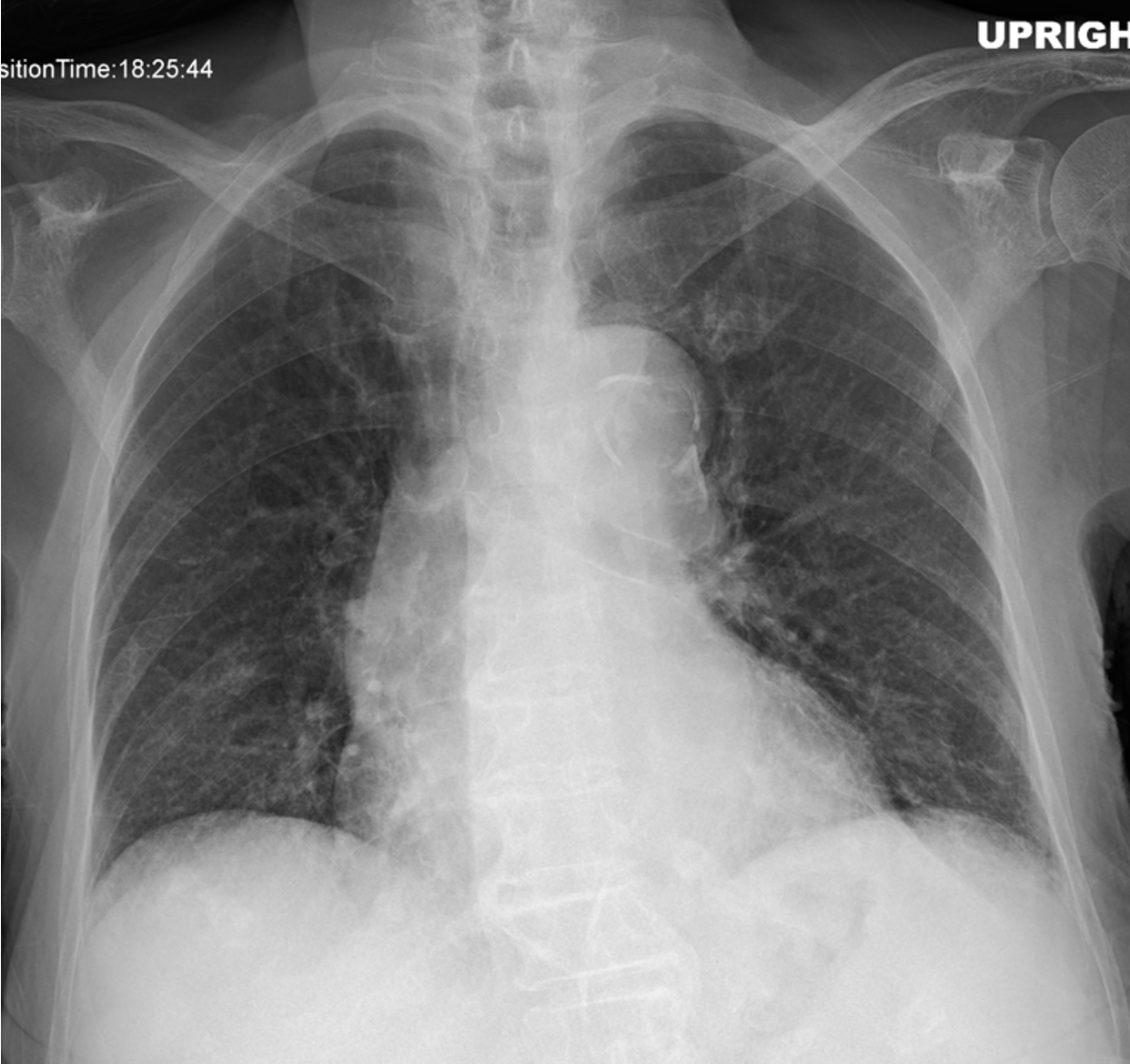
What do you see, what do you think and what would you do?
Click here for the answer
This case was not very difficult if you know what to look for. Our three colleagues (Doukopoulou, Kanakaraj and Marcos Mestas) did exactly that, and got the right diagnosis.
The main finding in this case in the PA chest radiograph, as Dr Flors indicates, is the abnormal position of the calcified plaque in the aorta (Arrow). The intima is displaced inward. Typical sign of aortic dissection (AD).
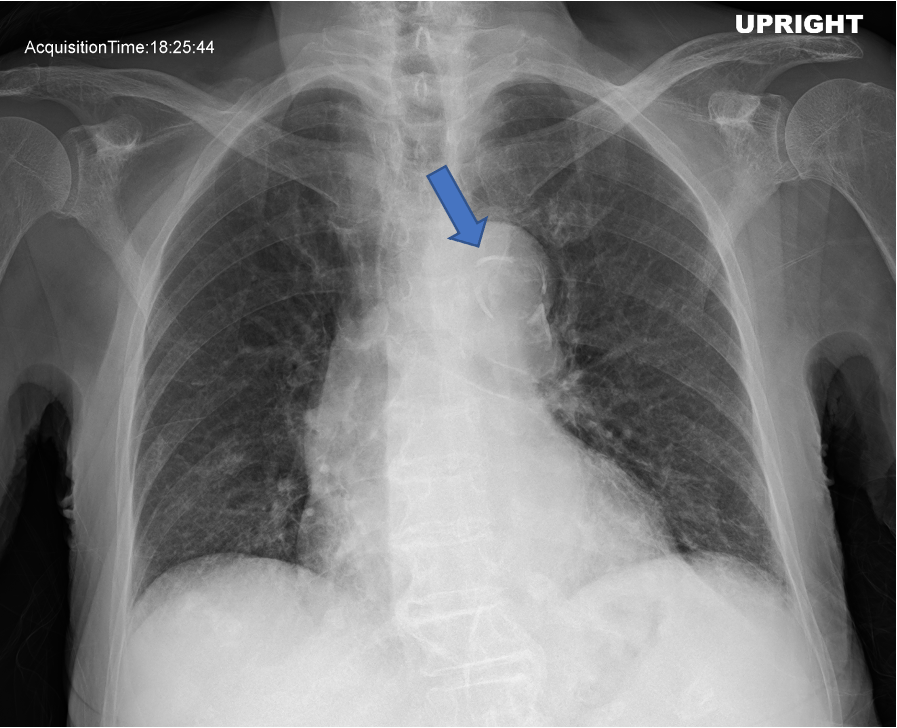
Three main signs in the chest radiograph are described in AD.
- Widened mediastinum
- Double aortic contour
- Inward displacement of atherosclerotic calcification (>1cm from the aortic margin), like in our case (arrow)
The next examination will be CT. These are the CT signs of AD:
- CT:
- Non-contrast:
- Displacement of atherosclerotic calcification into the lumen
- May demonstrate intramural hematoma
- CTA:
- intimal flap
- double-lumen representing the true and false lumens
- Mercedes-Benz sign in the case of a “triple-barreled” dissection
- Non-contrast:
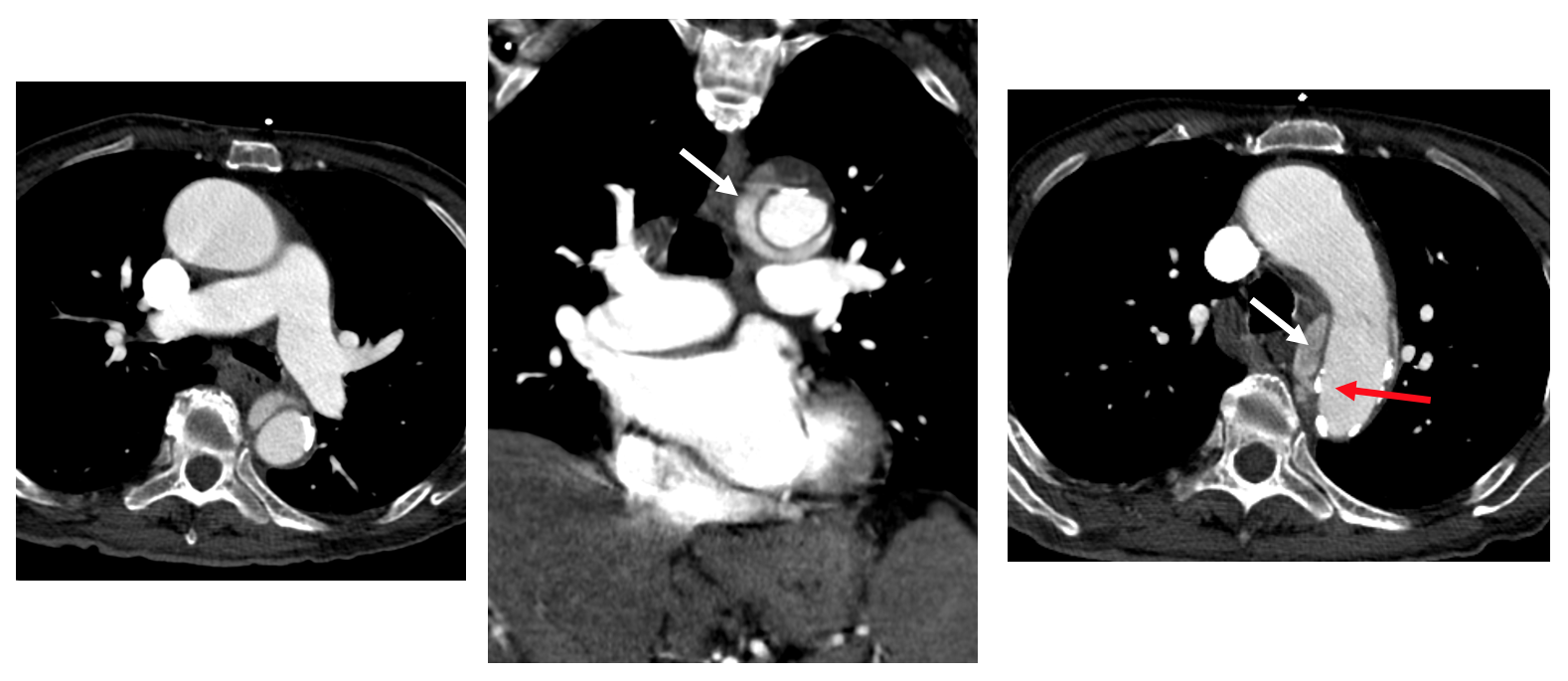
Contrast CT showing a descending aorta haematoma (false lumen) (White arrows) and the displaced intimal calcium (Red arrow).
Aortic Dissection main features:
- Most common acute aortic syndromes
- It occurs when blood enters the medial layer of the aortic wall through a tear or penetrating ulcer in the intima and tracks longitudinally along with the media, forming a false lumen within the vessel wall.
- Stanford classification:
- Type A: affects the ascending aorta
- Type B: begins beyond the brachiocephalic vessels
Tip to remember: In an elderly patient with acute chest pain and a wide mediastinum: look at the aorta, and especially calcification of the wall.
PD: Next week I will make it a bit more difficult…



We have an upright chest x-ray. The main finding is a dilated & calcified aortic arch with inward displacement of calcification. This is the calcium sign and is highly suspicious for aortic dissection, so given the history of acute chest pain I would suggest a contrast enhanced chest CT as next step.
apparent cardiomegaly.
dilated,unfolded aorta from aortic root down to abdominal aorta
calcification of aortic knuckle, descending thoracic aorta extending to abdominal aorta.
to consider 1. aortic aneurysm, 2.aortic dissection 3. aortic valvular disease aortic stenosis with involvement of coronary ostia.
interstitial markings are prominent.
osteoarthritic changes in lower dorsal spine.
further imaging with echocardiography and contrast ct chest.
Como comento Anastasia se ve agrandamiento del cayado aórtico con calcificaciones circunferenciales desplazadas hacia el centro de la “luz” en su borde interno.
Estamos frente a un sindroma aórtico agudo, muy probablemente una disección aorta que compromete al cayado aunque no podemos descartar un hematoma intramural. Necesitamos una angioTC no solo de tórax sino también de abdomen y pelvis para visualizar tipo, extensión y definir tratamiento.
Una última cosa, me sobra una opacidad de contornos definidos inmediatamente por debajo del cayado, asumo que puede ser debido a la tortuosidad de la aorta pero no me queda claro.
There are some calcifications projecting inside the aortic arch. Since the patient has acute chest pain, this finding can be an aortic dissection and must have a CT angiography.