José Vilar and Friends Case 50 (Solution+Case Lessons!)

Dear friends,
sorry about the wait, but I do hope you enjoy it!
This case was shown to me by Dr Santiago Isarría from Hospital Universitario Dr. Peset. Valencia. Spain. The case was a bit shocking to me, and I asked Dr Isarría if he could let me show it in the blog because it contains several interesting features. Dr Silvia Medrano, a smart radiology resident, provided me with the images and the pertinent information.
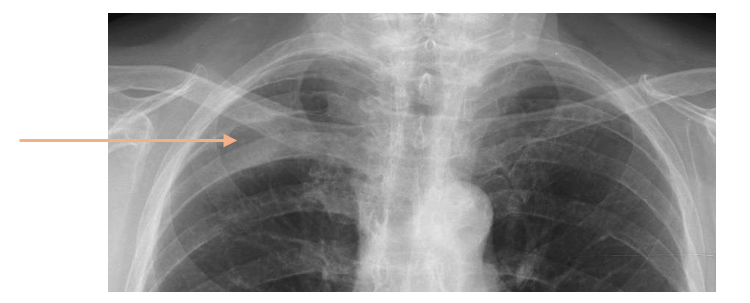
The patient is a 72-year-old lady with a history of multiple myeloma being followed. Now she complains of right dorsal chest pain.

Do you see something? (It’s subtle).
23.6. Update: Additional Information!
You guys are a bit reluctant. Let me help you a little bit.
The patient comes back to the hospital 10 months after the previous radiographs. Take a look at the images and go back to the previous films. Do you see something now?
This is an example of missed pathology.
Now what do you think? What would you do?

I will post another update on Friday!
25.6. Update: CT Images
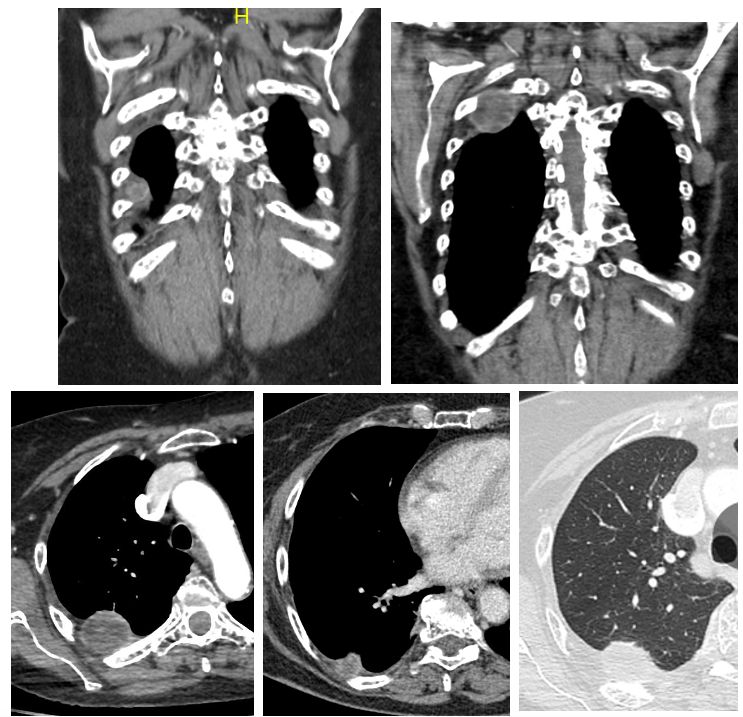
A CT was obtained. Here are the main images.
What is the most probable diagnosis? Any differential?
The answer will be posted on Tuesday..
Click here for the answer
Let us review the radiological findings in this case.
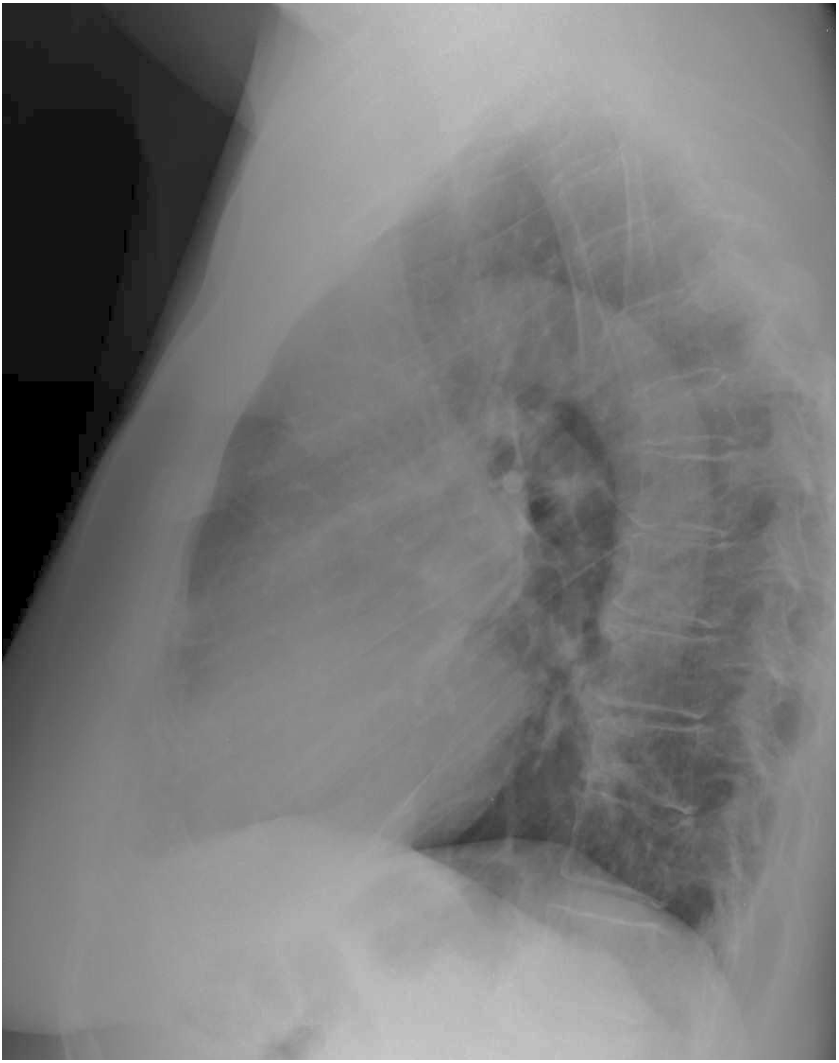
The first radiographic study, when the patient presented with chest pain shows a subtle finding: In the PA projection there is an increased density in the right upper hemithorax (white arrows). Also, if you look carefully the lateral there is also an abnormal bulge/density posteriorly. (Yellow arrow).

The radiographic study 10 months later shows definitely abnormal masses in the right hemithorax with rib destruction.

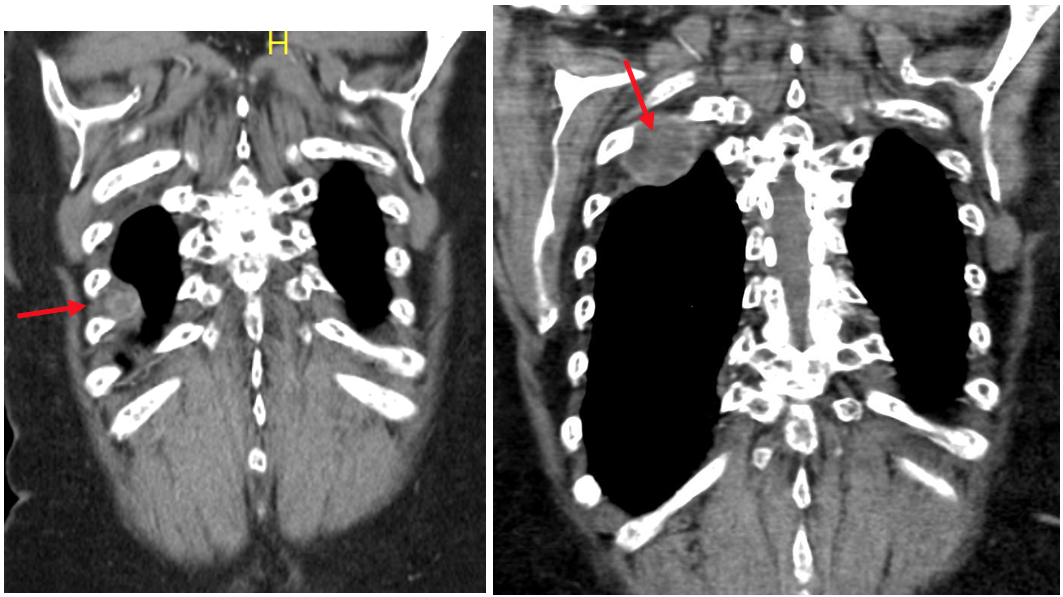
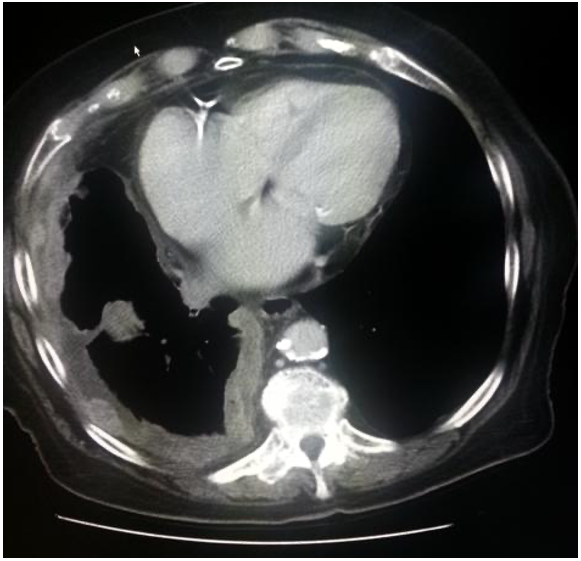
The CT confirms and outlines these findings. Extrapulmonary masses with rib involvement. Note that the mass has an heterogeneous density.
(Red arrows).
In view of the radiographic abnormalities in a patient with multiple myeloma, the most common diagnostic choice should be multiple myeloma.
Yet, the biopsy of the lesions revealed a surprise for the radiologists: The pathologists reported that the tumour was a primary localized biphasic malignant mesothelioma.
This is a rare case of isolated mesothelioma in a patient with no history of exposure to asbestos or other related factors.
The differential diagnosis of an extra pleural mass includes:
- Mesothelioma
- Metastases
- Bronchogenic carcinoma
- Primary pleural tumour
- (Fluid).
Pleural mesothelioma:
- Is a tumour originating in the mesoderm. (Pleura, Pericardium, peritoneum and tunica vaginalis of testicles).
- Is the most common primary neoplasm of the pleura.
- Imaging. Thickening of the pleura with nodular/mass appearance.
- Affects mediastinal pleura.
- Tendency to grow towards the lung.
In this case: localized biphasic ( Epithelioid -Sarcomatoid) malignant mesothelioma the main features are:
- Circumscribed masses
- Heterogeneous masses in CT
- May have cysts formations.
- Local invasion
- It contiguous to the pleura.
This is a very rare type of mesothelioma that sometimes may be difficult to diagnose by pathologists. Biomarkers such as EMA, WT-1 or molecular markers may help with the diagnosis.
Typical Asbestos related mesothelioma

Isolated Biphasic Mesothelioma
This is a quite rare case in which the presence of a disease (Myeloma) confused the radiologists and clinicians. Trying to correlate the findings other alternatives such what proposed Andrea: Extramedullary hematopoiesis could be considered. Nevertheless, we can obtain some lessons from the case:
Main points of this case:
- Any asymmetry in the PA radiograph such as the density seen in the first radiograph, must be further investigated.
- Extrapulmonary masses: include mesothelioma in your differential.
PD: With this case I conclude the blog cases and wish you a very happy and healthy summer vacation. Be good, enjoy nature, friends and family. I will try to do it too and hope to come back after the summer with more cases for you.


I have to right in spanish because I am not sure of anything.
Creo que hay una opacidad a nivel de la 1er articulación costocondral derecha en la Rx frente, en la Rx lateral me parece que es paravertebral. Todo sin mucha confianza…
También dos vértebras dorsales disminuidas de altura y secuelas de fracturas costales izquierdas.
write*
Excellent Marcos you are getting close. Now try to give a differential
Extramedullary hematopoiesis in a pt with MM.
Diffuse decreased bone density with reduced vertical height of possible T4 vertebrae. Rounded enhancing peripherally soft tissue mass pleural based posteriorly on right chest.