José Vilar and Friends Case 52 (Solution+Teaching tips!)
Dear Friends,
After our last case that was successfully analyzed by everybody…
Today I bring a case from Dr Santiago Isarría (Hospital Universitario Dr. Peset, Valencia).
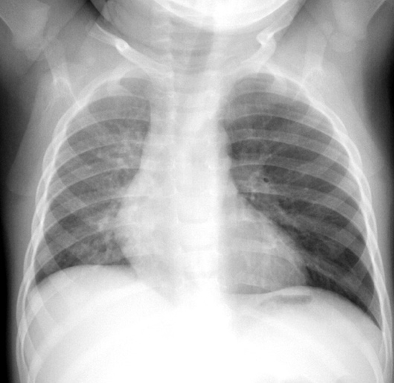
A patient referred from the cardiology clinic refers mild chronic shortness of breath.
As always, look carefully and let me know what you see and what you think.
( Disregard metallic image in left lower hemithorax)

Wednesday update: Additional images
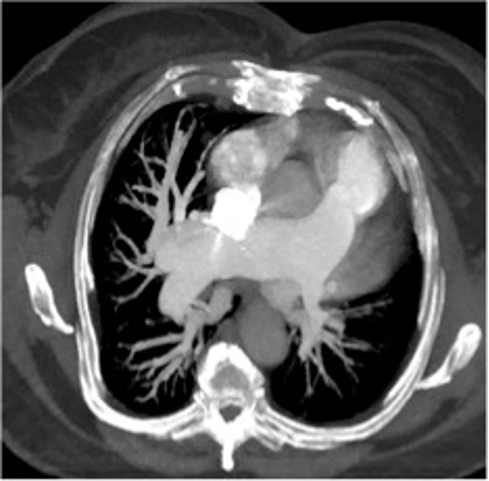
Here are some CT images:
Click here for the answer
This case is a classical example of what has been called “ Hyperlucent Lung”.
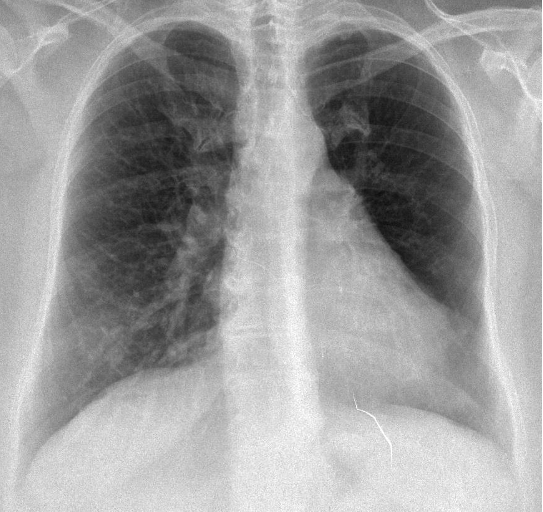
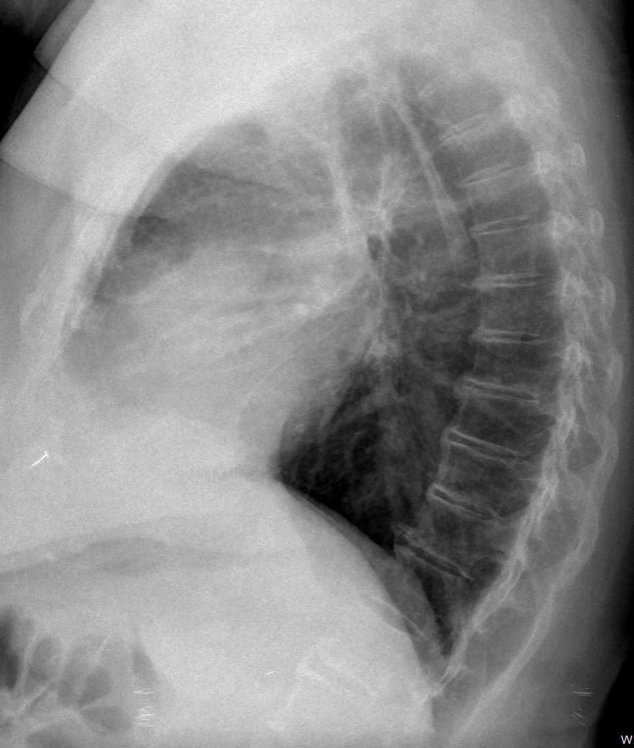
The frontal chest radiograph shows (as Dr Doukopoulou said wisely) that the left lung is darker. A close look also shows an asymmetry in the pulmonary vascularity: the right lung has many vessels while the left has few and smaller vessels.

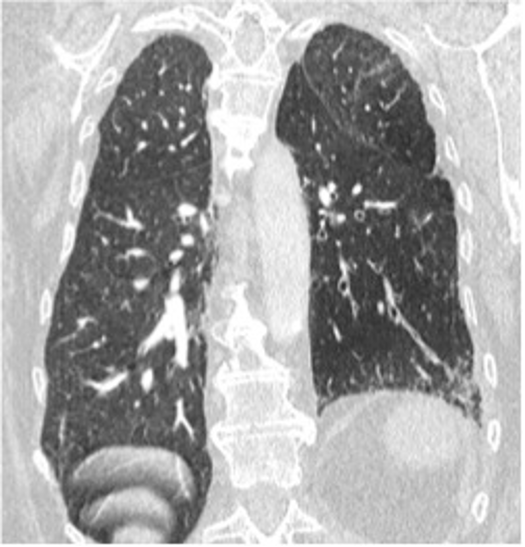
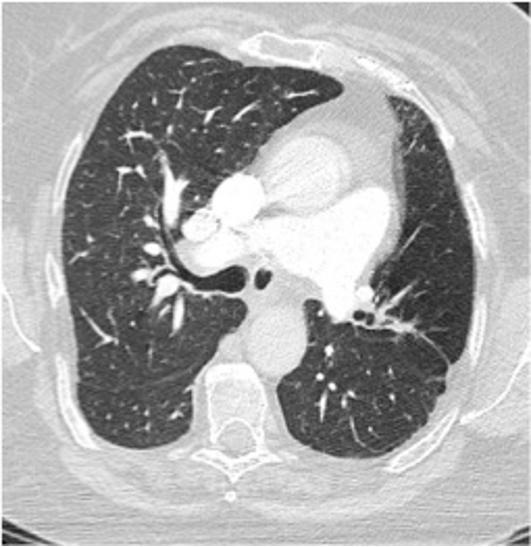
The CT confirmed these findings showing a small left pulmonary artery. Other findings in CT are the presence of some airway disease, bronchiectasis, in the left lower lobe as well as hypodense areas (low perfusion).
A ventilation/perfusion examination showed the areas of matching diminished ventilation and perfusion in the left lung.
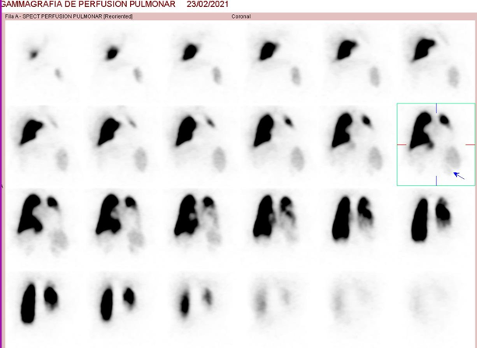
Perfusion

Ventilation
Diagnosis: Swyer James McLeod syndrome.
Swyer-James Mc Leod (SJM) is a variant of post-infectious bronchiolitis obliterans. Usually the sequela of a viral infection during infancy or early childhood. Several viruses or even mycoplasma have been attributed the responsibility of this pathology where the airways are involved permanently.
SJM may be asymptomatic or associated with respiratory infections due to the presence of abnormal bronchi.
This case brings me to the classical differential diagnosis of a Hyperlucent Lung.
When we see in the PA chest radiograph a hemithorax that is darker that the contralateral, we must think of several possibilities according to the origin of the pathology:
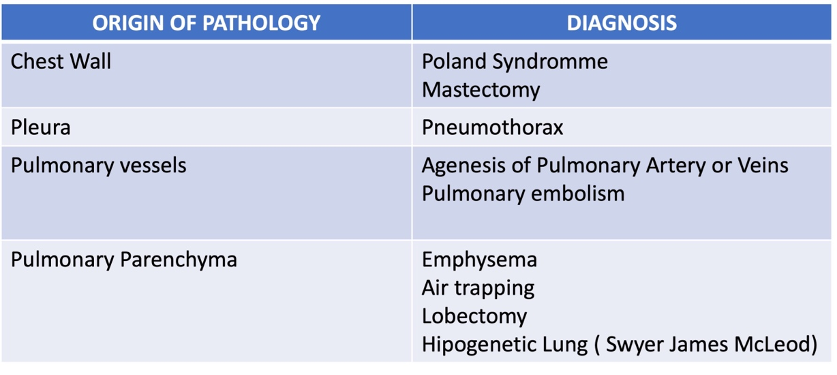
Two tips regarding the chest wall anomalies that simulate hyperlucent lung:
- Look at the edges of the image, especially the axilla and compare it with the other side. When the problem is in the chest these areas will also be darker.
- Look at the pulmonary vessels that, in these cases, should be as large and numerous as in the other side.
- And, always, if it’s a woman, look for the breasts! Quite often mastectomy goes unrecognized. ( I used to ask my residents, after reading a chest x ray, “did she have both breasts?” and very often they had to go back to the case and look…).

Mastectomy simulating hyperlucent lung.
Other causes. Lung hyperinflation such as in air trapping due to bronchial obstruction. Remember this case of a child with a foreign body in the left main bronchus. (Case 46 in our Blog). (Of course, the clinical scenario in this case was revealing).
Finally vascular abnormalities, such as pulmonary artery agenesis, or large pulmonary embolism (Westermark sign) may also show a hyperlucent lung due to the decreased vascularity.


The frontal chest radiograph demonstrates a unilateral left hyperlucent lung with diminished vasculature. We also notice a prominent left pulmonary artery. It could be Swyer-James syndrome. The next step is a chest CT scan.
Welcome back Anastasia
In the additional CT images i notice that the left lung is smaller, there are some bronchiectasis and the left pulmonary artery is small, hence the diminished vascularity in the periphery.
I stick with my previous diagnosis of Swyer-James syndrome.
Thank you Dr Vilar for the challenging cases.