Advanced MR imaging helps in interpretation of brain tumours
Watch this session on ECR Live: Saturday, March 9, 16:00–17:30, Room G/H
Advanced MR imaging techniques such as perfusion and functional imaging have been a great help in improving the diagnosis and staging of brain tumours. Unlike conventional MR techniques, advanced MR techniques can be used to obtain information not only on the morphological, but also on the functional characteristics of tumours.
One of the most common types of brain tumour is glioblastoma, which is highly malignant and has a high cell reproduction rate due to the fact that it is nourished by a large network of blood vessels. According to the American Brain Tumour Association there are two types of glioblastoma: primary glioblastomas, which tend to form and make their presence known quickly by growing aggressively, and secondary glioblastomas, which are also aggressive but show slower growth and only represent 10% of all diagnoses.
Due to a lack of effective of therapies, the prognosis in cases of glioblastoma remains poor, and so there is an urgent need to find new therapeutic approaches.
One of the reasons why the treatment of glioblastoma is such a challenge is that it consists of various cell types, which may react differently to various forms of treatment. As a result, the treatment, in most cases, combines several methods.
“Overall there is no effective treatment for high-grade glioblastoma. The current therapeutic approaches are surgical resection of the tumour bulk if possible, depending on the location of the tumour, followed by radiation and chemotherapy. One of the main difficulties is that it can be difficult to exactly measure the tumour‘s extent, since malignant tumour cells often infiltrate the brain parenchyma beyond the tumour’s contrast-enhanced portion, which makes it difficult to completely surgically resect the initial tumour,” said Professor Pia C. Maly Sundgren, head of the department of diagnostic radiology, Clinical Sciences, Lund University, and Senior Consultant at Skåne University Hospital, Lund, Sweden.
Radiation and chemotherapy are used to slow the growth of tumours that cannot be removed surgically. Chemotherapy may also be used in young children to delay the need for radiation.
Despite achievements in the field of advanced imaging techniques it still remains difficult to predict and monitor brain tumour response in individual patients, especially when it comes to the use of anti-angiogenic therapies, during which uncommon patterns of tumour response and progression can be seen.
Pseudoprogression for example usually occurs early while treating a brain tumour with radiation and Temodar, which makes the tumour appear to progress due to its increased size and contrast enhancement. This is a common reaction to the treatment, but the lesion will decrease in size and concentration on its own if the initial treatment is continued without any change.
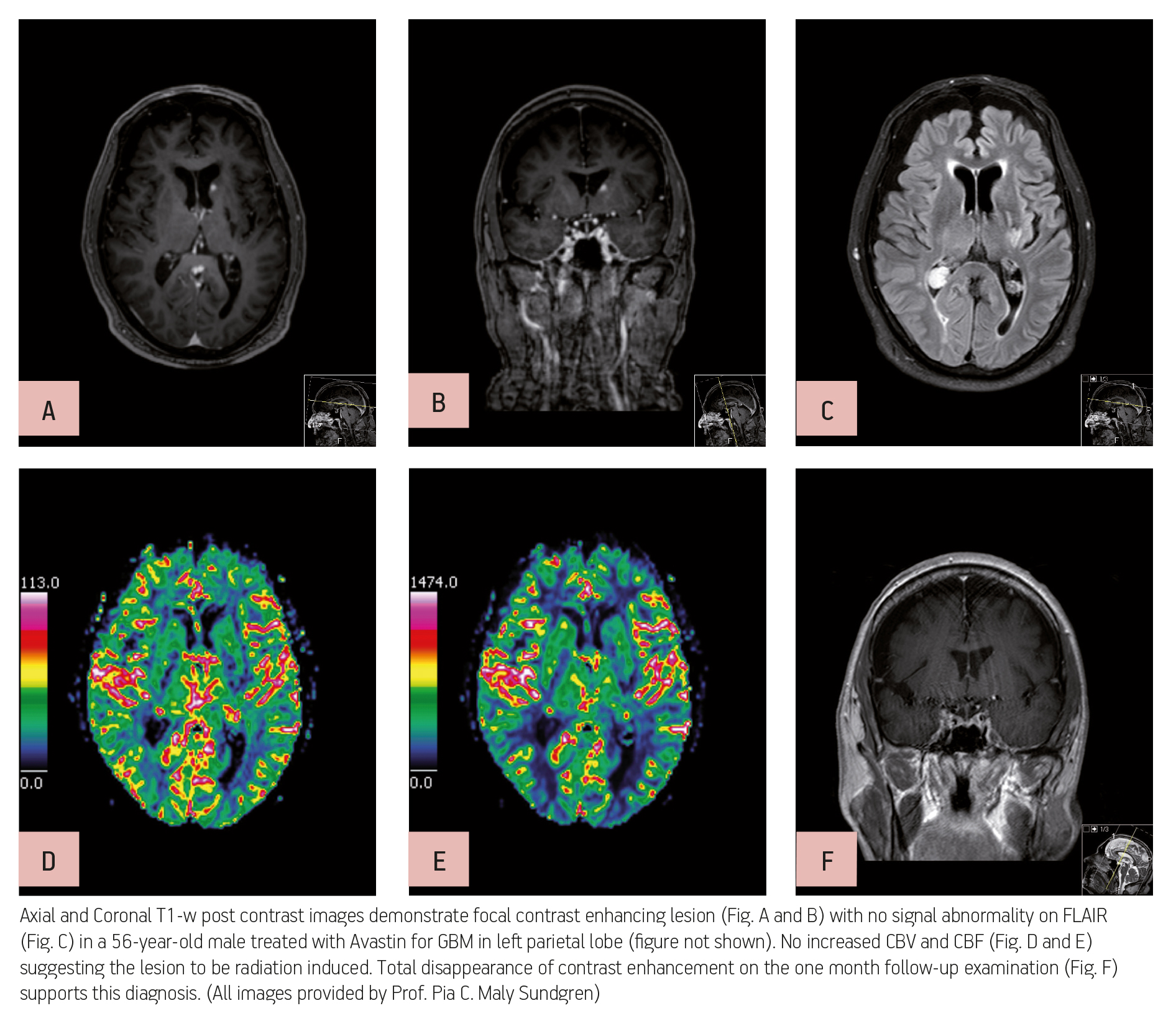
Pseudo-response on the other hand occurs during anti-angiogenic therapy, for example the use of Avastin, which causes significant reduction in contrast enhancement due to changes in vascularity, but should not be mistaken for a real reduction in the extent of the lesion.
Prof. Sundgren explained how to spot these pseudo-reactions: “Both can be best detected with advanced MR imaging especially diffusion-weighted imaging, which looks at the random motion of water molecules and perfusion imaging, which studies the cerebral blood volume and cerebral blood flow in the brain, including the tumour. Though MR spectroscopy is less helpful.”
Confusion and incorrect interpretation can, in part, be avoided by having good clinical information about the original tumour type; tumour extent, as seen through MR imaging after contrast administration; current course of chemotherapy treatment; radiation dose; and the time between radiation treatment and imaging findings. It is also helpful to use perfusion and diffusion imaging as part of the MR imaging protocol. The use of PET imaging might also be valuable, as well as a combination of information gained from both modalities.
Despite the fact that the long-term prognosis remains poor, there have been recent studies which have shown an increase in the overall survival rate for glioblastoma patients treated with Avastin, according to Prof. Sundgren.
Especially in recurrent glioblastoma, the treatment options have mainly been limited to high-dose chemotherapy. The administration of Avastin alone or in combination with CPT-11 has shown a significant improvement in response rates, progression-free survival times and overall survival.
A more recent study has shown that Avastin alone was nearly as effective as it was in combination with chemotherapy, but with much milder side effects. When dealing with patients suffering from terminal glioblastoma a stand-alone Avastin therapy may lead to an improvement in quality of life, without the common toxic side effects of chemotherapy.
When asked about whether we need advanced imaging techniques in daily practice, Prof. Sundgren gave a very clear answer: “Yes, I strongly advocate the use of advanced MR imaging in the work-up and follow-up of a patient with brain tumour. It is helpful for the radiologist or neuroradiologist to give the correct interpretation and it is helpful for the clinician in the treatment of the patient.”
The session will also feature a talk by Professor Meng Law from the Los Angeles County Hospital & USC Medical Center on the topic of diffusion-weighted imaging (DWI) and diffusion tensor imaging (DTI). His talk will include information on how to use diffusion imaging for predicting the response to radiation while using functional diffusion maps, as well as chemotherapeutic agents such as temozolomide and bevacizumab. The challenges and pitfalls of using DTI, fibre tractography (FT) and fractional anisotropy (FA) maps for presurgical planning will be discussed.
“There is significant error in comparing FT and FA presurgical maps to intraoperative electrophysiological mapping up to 8.7 mm and sometimes even more. This is due to errors in co-registration, brain shift, imaging error and surgical error,” explained Prof. Law.
Some controversial issues about whether DTI is really useful in the clinical setting or merely just a mathematical tensor algorithm will also be raised.
The session will conclude with a talk on perfusion imaging from Professor Yelda Özsunar from the Adnan Menderes Universitesi in Aydin, Turkey.
Refresher Course: Neuro
Saturday, March 9, 16:00–17:30, Room G/H
RC 1111: Brain tumours: advanced imaging techniques in daily practice – do we really need them?
Moderator: Z. Merhemic; Sarajevo/BA
A. Diffusion-weighted imaging (DWI) and diffusion tensor imaging (DTI)
M. Law; Los Angeles, CA/US
B. Perfusion imaging
Y. Özsunar; Aydin/TR
C. Follow-up after treatment
P.C. Maly Sundgren; Lund/SE

