Dr. Pepe’s Diploma Casebook: Case 95 – A painless approach to interpretation (Chapter 2) – SOLVED!
Dear Friends,
As you may remember from Diploma Case 94, when I’m facing a chest radiograph I start by asking three questions:
a) Is there any visible abnormality?
b) It is intra- or extrapulmonary?
c) What does it look like?
Today we will discuss the second question, showing chest radiographs in two different patients. Is the abnormality intra- or extrapulmonary? Check the images below, leave your thoughts in the comments and come back for the answer and discussion on Friday.

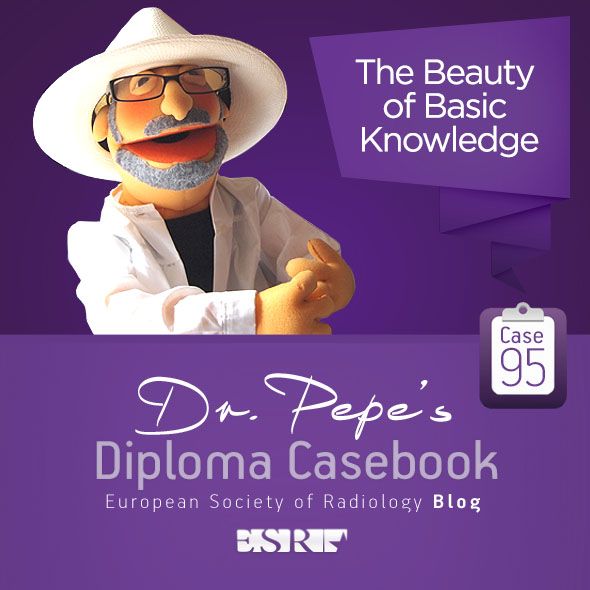
CASE 1: 58-year-old man with pain in left hemithorax

CASE 2: Pre-op radiograph for renal carcinoma in a 62-year-old male smoker. A previous study three years earlier was normal.
Second question: Is the lesion intra- or extrapulmonary?
If you answered intrapulmonary in Case 1 and extrapulmonary in Case 2, you’re right.
Case 1 (below) shows a peripheral mass that looks extrapulmonary on first impression. However, part of the contour is ill-defined (A, arrow), which is a strong argument for an intrapulmonary lesion. Enhanced coronal CT confirms an irregular solid intrapulmonary mass (B, arrow). Final diagnosis: carcinoma of the lung.
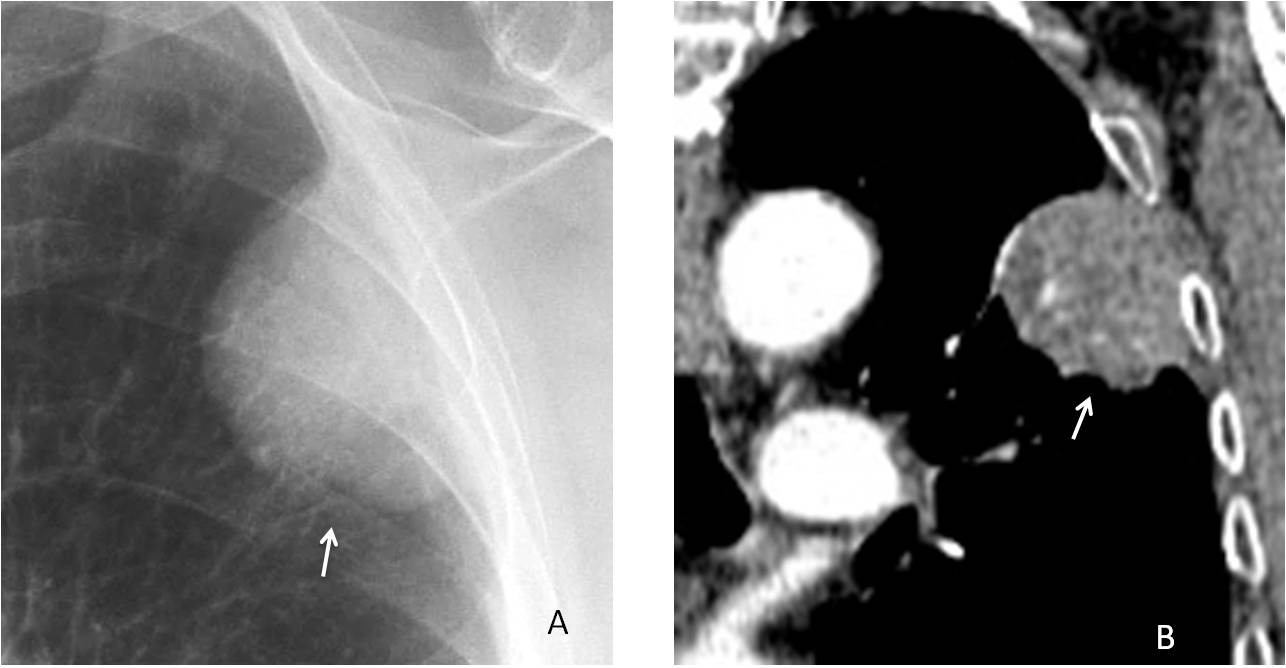
Case 2 (below) shows an apparent LLL nodule (A, black arrow) that was not visible 3 years before. The diagnostic clue is an old fracture of the 7th left rib (A, red arrow). CT shows that the nodule corresponds to a non-consolidated fracture of the 10th left rib (B,C, arrows). There is also an old fracture of the 11th rib. The patient had a car accident two years ago.
Final diagnosis: multiple old rib fractures, one of which simulates a lung nodule.
As is illustrated in Cases 1 and 2, extrapulmonary lesions can simulate lung lesions and vice versa. In this chapter I would like to focus on signs that point to a diagnosis of extrapulmonary lesion. Recognising these signs simplifies the diagnostic approach and avoids taking the wrong diagnostic path.
An abnormality that arises from the pleura or chest wall can simulate a lung lesion when:
a) it presents as a peripheral mass
b) it projects over the lung parenchyma
The appearance of peripheral extrapulmonary masses in the PA radiograph changes depending on their location relative to the x-ray beam.
When the mass is lateral and tangential to the x-ray beam, it typically shows a well-defined border, tapering distal edges, and an elongated shape (pregnancy sign) (Fig. 1).
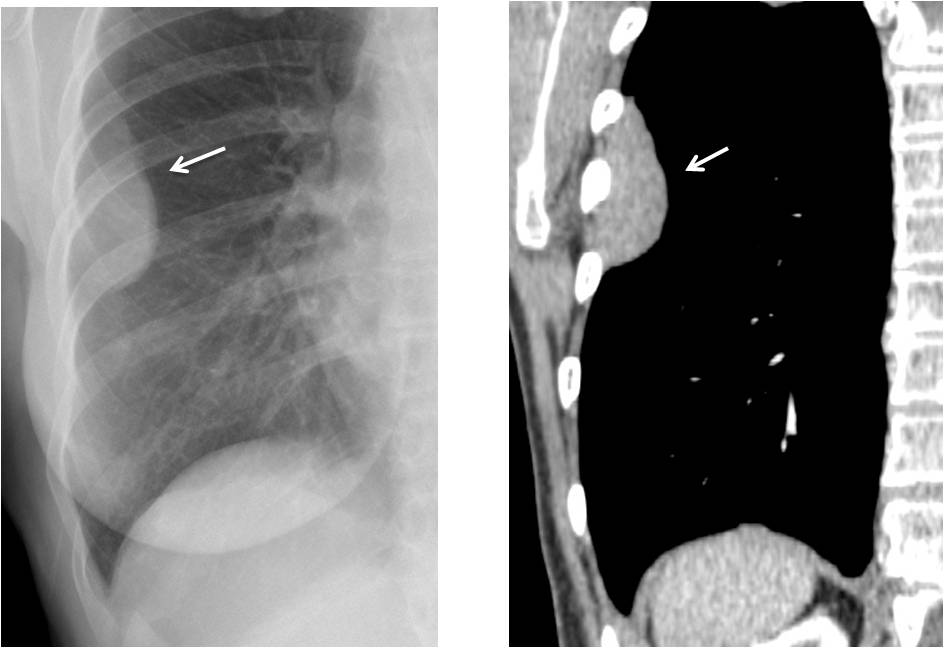
Fig. 1
Fig. 1. Typical extrapulmonary lesion (A, B, arrows) with elongated appearance, well-defined border, and tapering distal edges. Diagnosis: pleural metastasis from thymoma.
Nonetheless, the pregnancy sign is sometimes ambiguous. In my experience, I mainly rely on a well-defined contour to differentiate intra from extra (Fig. 2).
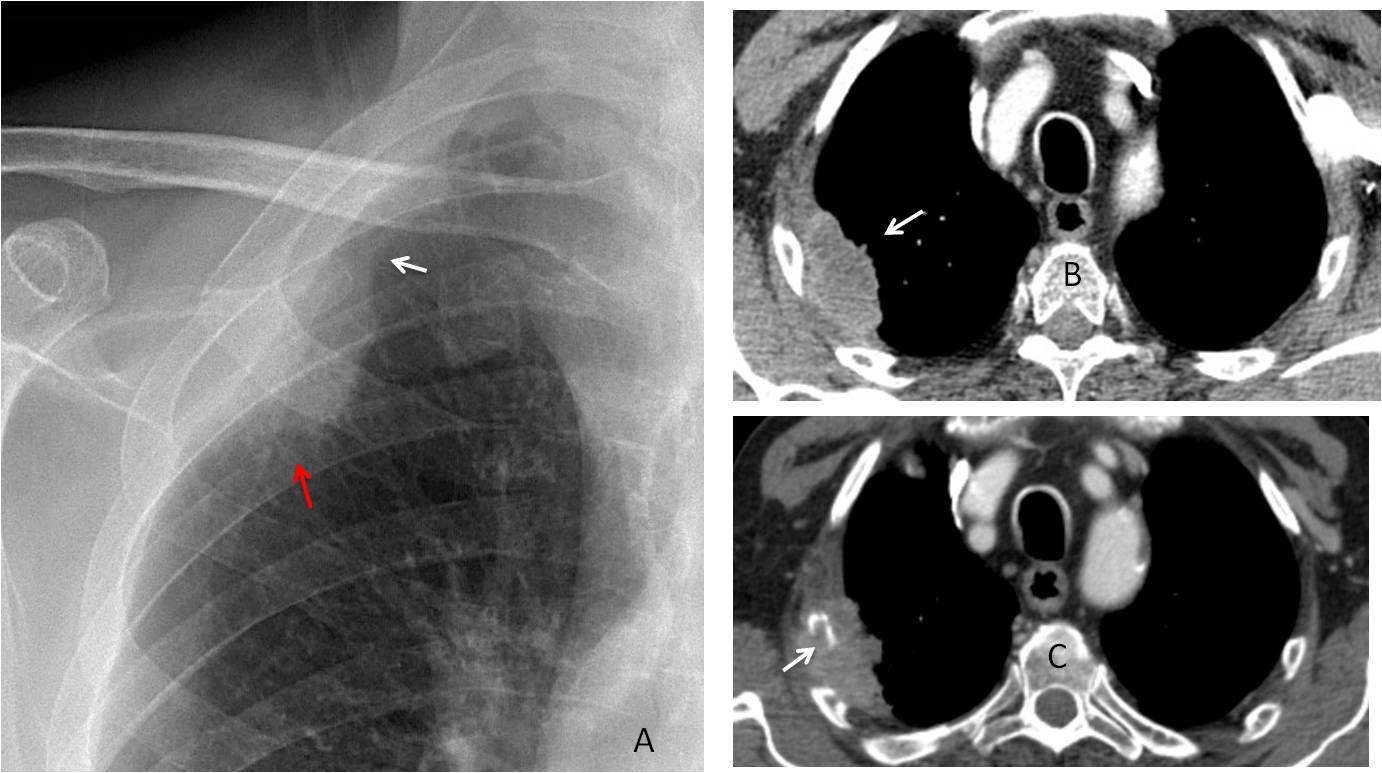
Fig. 2
Fig. 2. 54-year-old man with chest pain. PA radiograph shows a peripheral lesion with elongated appearance and an upper tapering edge (A, white arrow). However, the indistinct border (A, red arrow) favours an intrapulmonary lesion. Axial CT confirms a peripheral lung carcinoma (B, arrow). Four months later, CT shows invasion of the underlying rib (C, arrow).
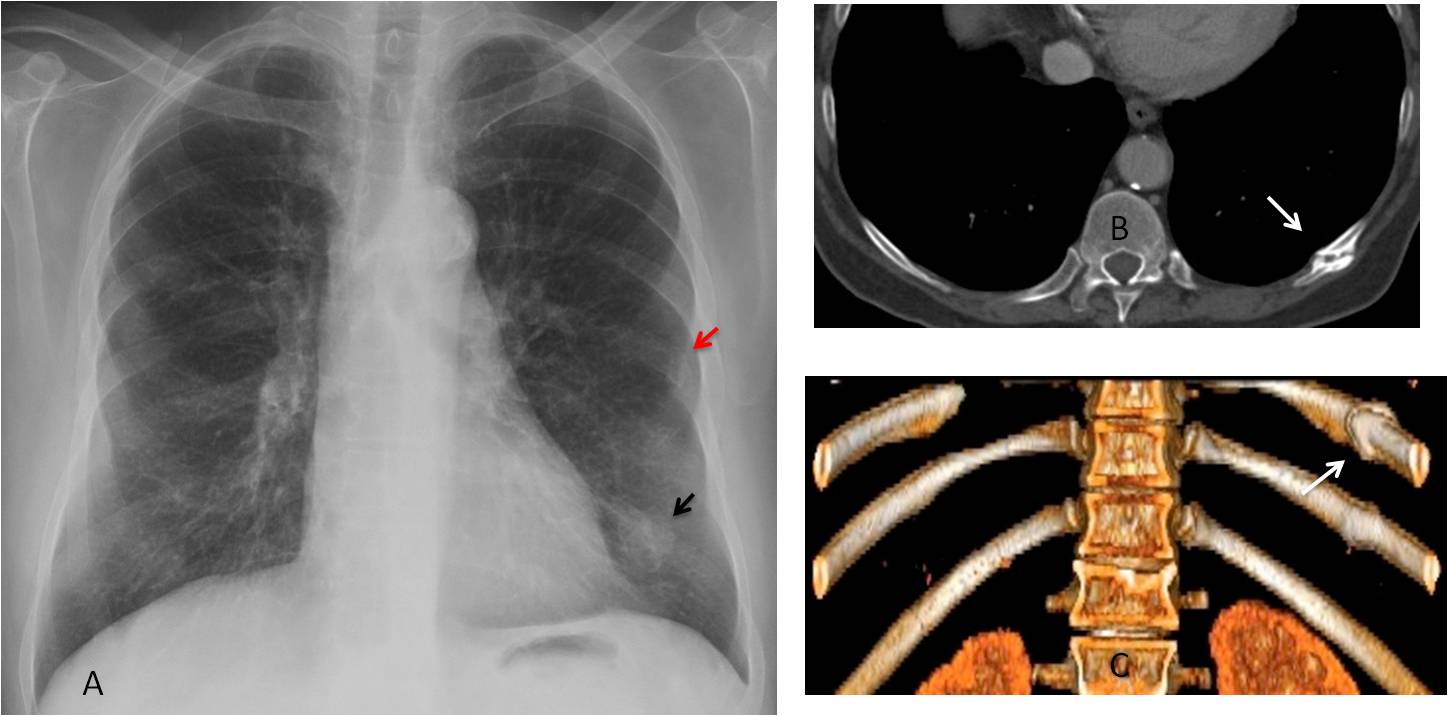
Because of the curvature of the thoracic cage, a lesion may be oblique to the X-ray beam. In these cases the mass is projected into the lung, which outlines only the inner border. The lateral outline of the lesion disappears because it is in contact with the chest wall (incomplete border sign) (Fig. 3).
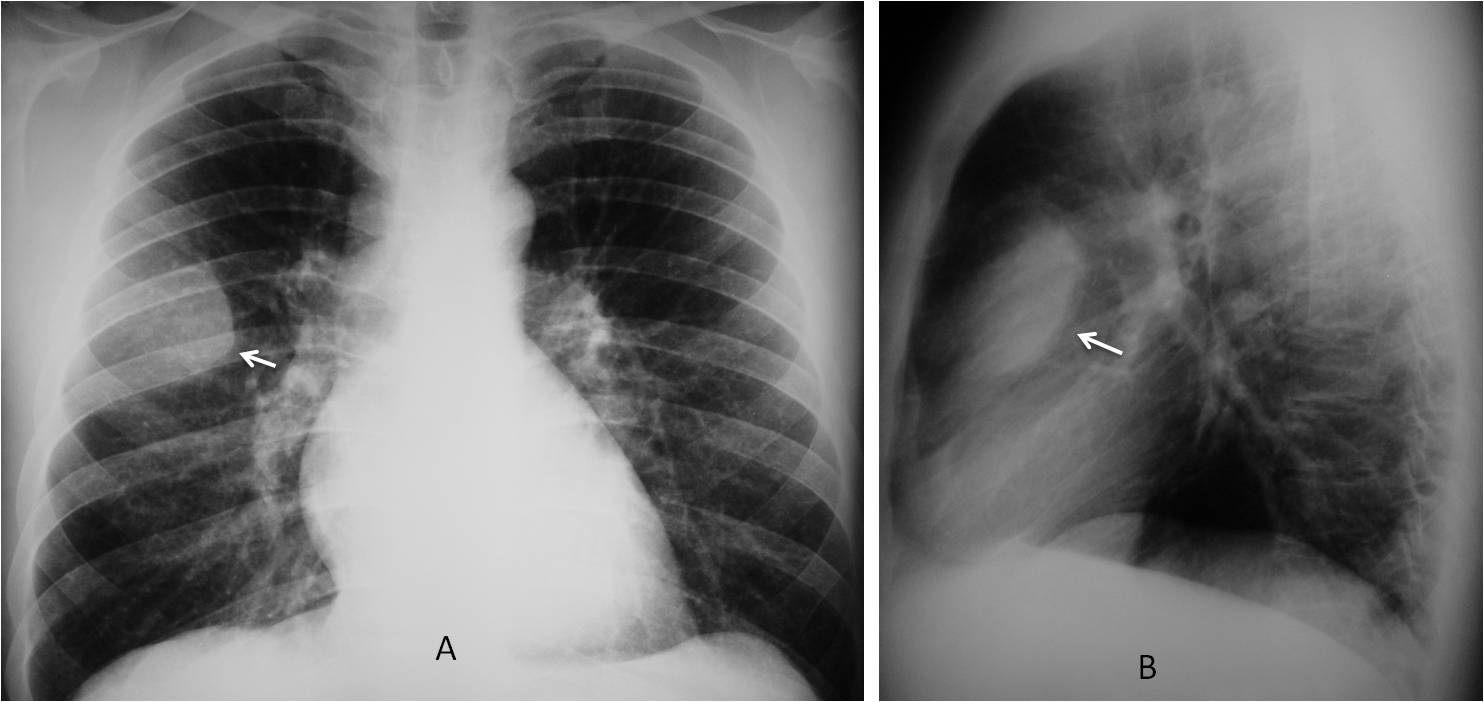
Fig. 3
Fig. 3. 54-year-old man with pain in the right hemithorax. PA radiographs show an apparent intrapulmonary lesion which is only well-defined in the inner aspect (A, arrow). The outer border is indistinct because it merges with the chest wall. The same occurs in the lateral view (B, arrow).
CT clearly explains the incomplete border sign. The inner border is visible because it’s outlined by air (C,D, arrows). The outer border is fuzzy because it meets the chest wall. Diagnosis: metastasis to anterior 4th rib.
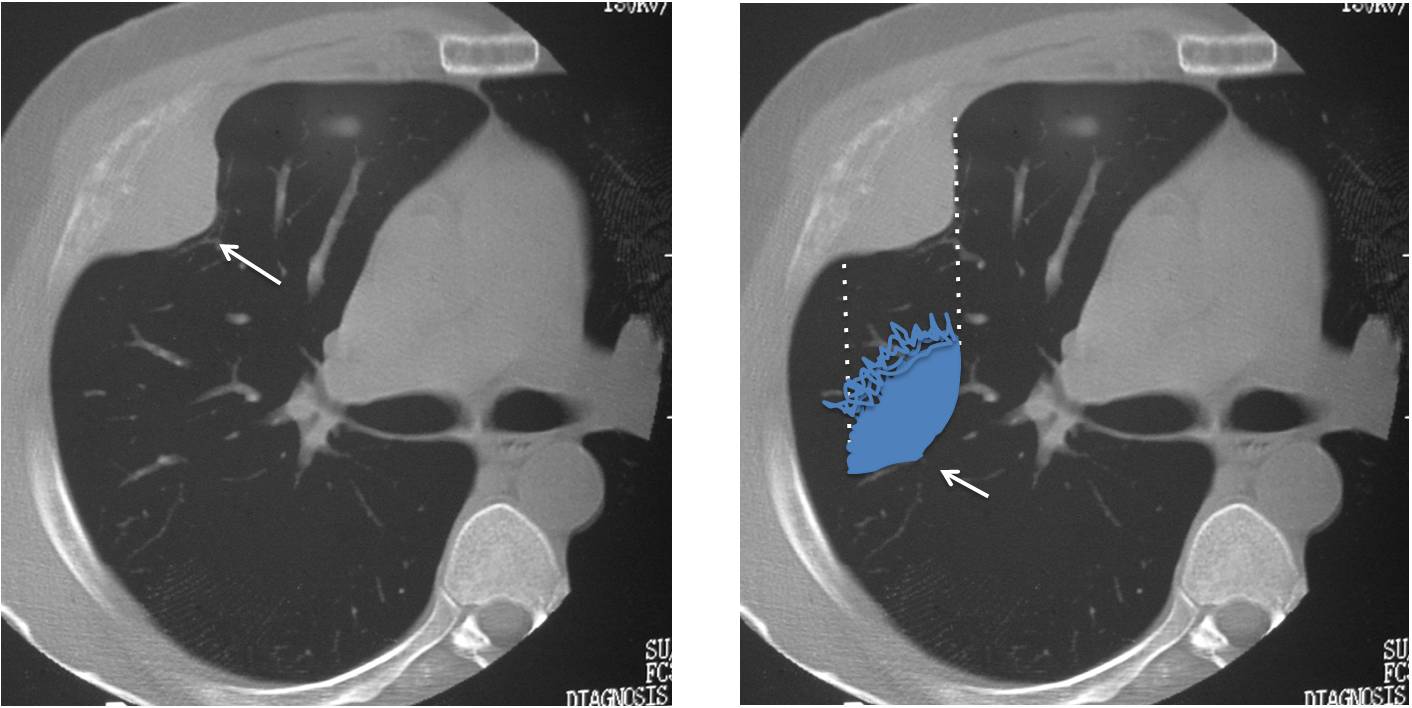
Fig. 3
Finally, when the lesion is in the anterior or posterior chest wall, it projects en face in the PA view. As a result, the borders are not tangential to the x-ray beam, becoming indistinct and simulating air-space disease. The lateral view helps demonstrate the typical extrapulmonary appearance (Fig. 4).
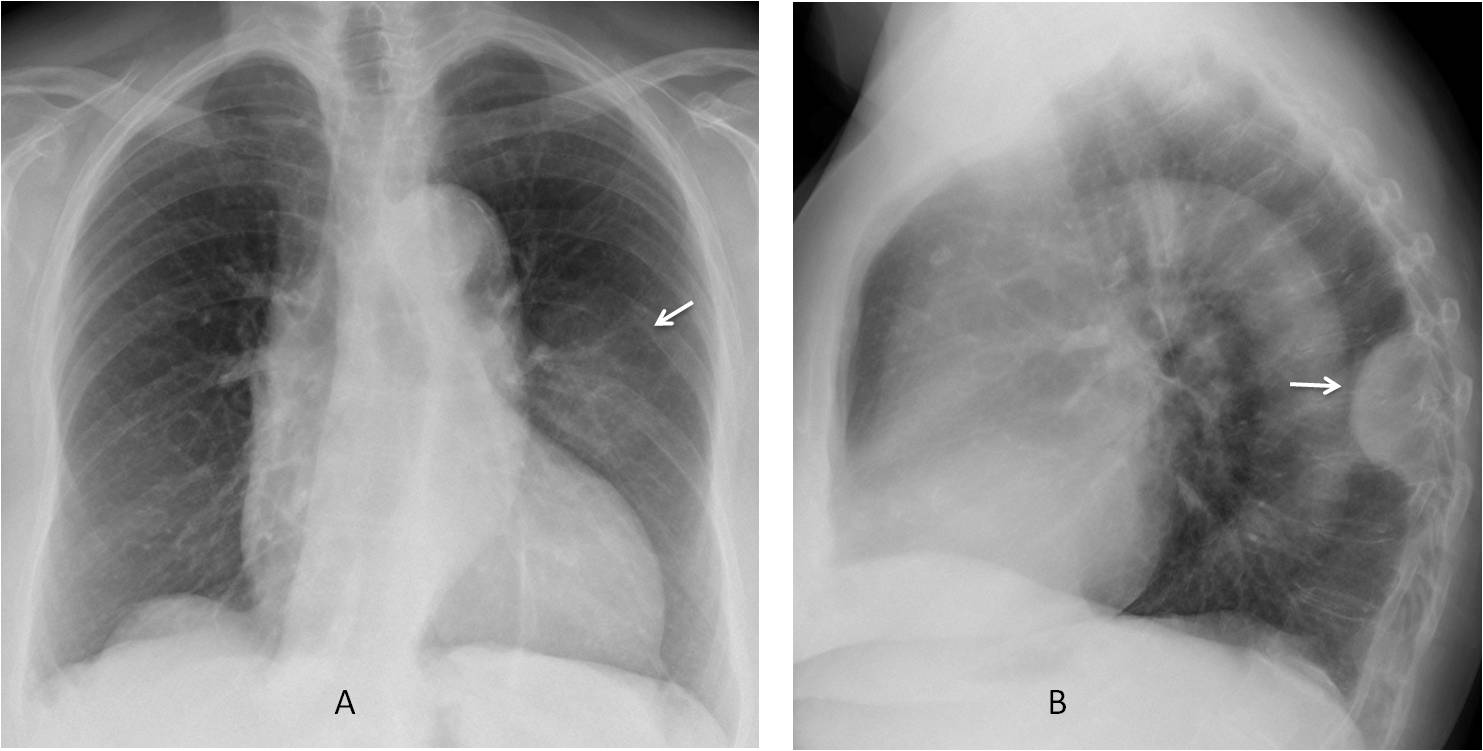
Fig. 4
Fig. 4. 76-year-old woman with lymphoma. PA radiograph shows an ill-defined opacity in the left lung (A, arrow) that looks like air-space disease. The lateral view show a well-defined extrapulmonary lesion (B, arrow). Without the lateral view, the lesion would be placed in the wrong compartment.
Enhanced axial CT confirms the extrapulmonary location of the lesion (C and D, white arrows). Note the intercostal artery displaced forward by the extrapleural component of the mass (C and D, red arrows). Diagnosis: chest wall lymphoma.
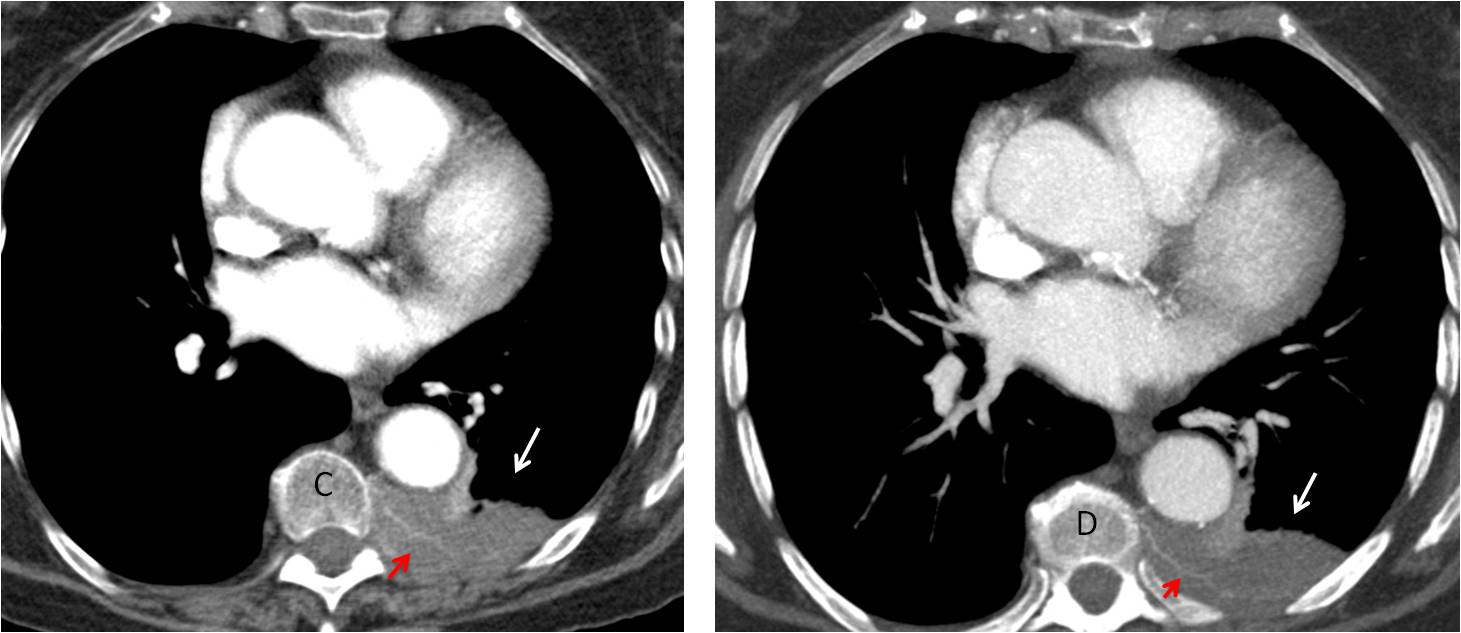
Fig. 4
Rib and pleural lesions may project over the lung, simulating a lung abnormality. Most rib lesions are old fractures or bone islands (Fig. 5). It is interesting to note that the curvature of the rib cage may lead to an intrapulmonary appearance of the lesion in both the PA and lateral views (Fig. 5, drawing).
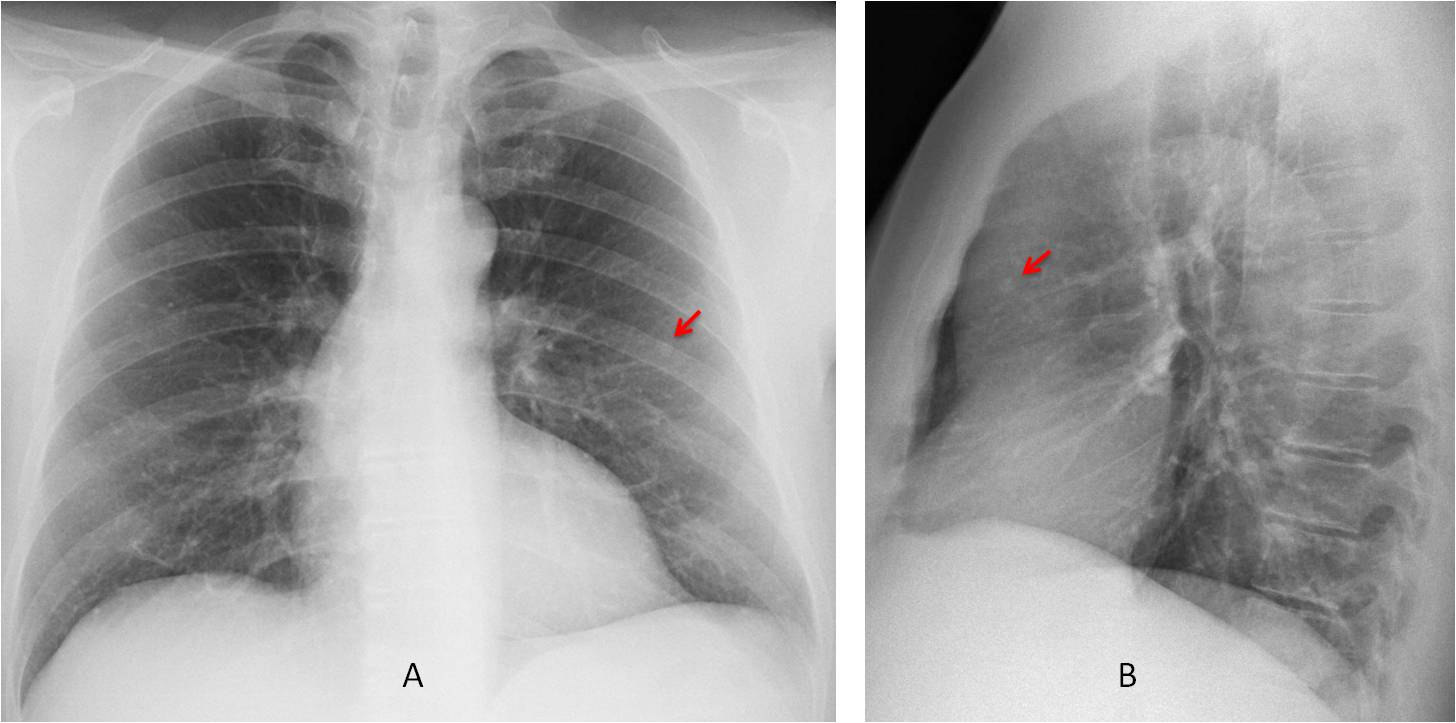
Fig. 5
Fig. 5. Pre-op radiographs for renal carcinoma. PA and lateral views show a tiny nodule in the middle lung field that seems intrapulmonary (A and B, arrows).
Axial CT demonstrates that the apparent pulmonary nodule corresponds to a bone island in a rib (C and D, arrows). The perpendicular lines in D explain how the curvature of the chest wall projects the bone island into the lung in the PA and lateral views.
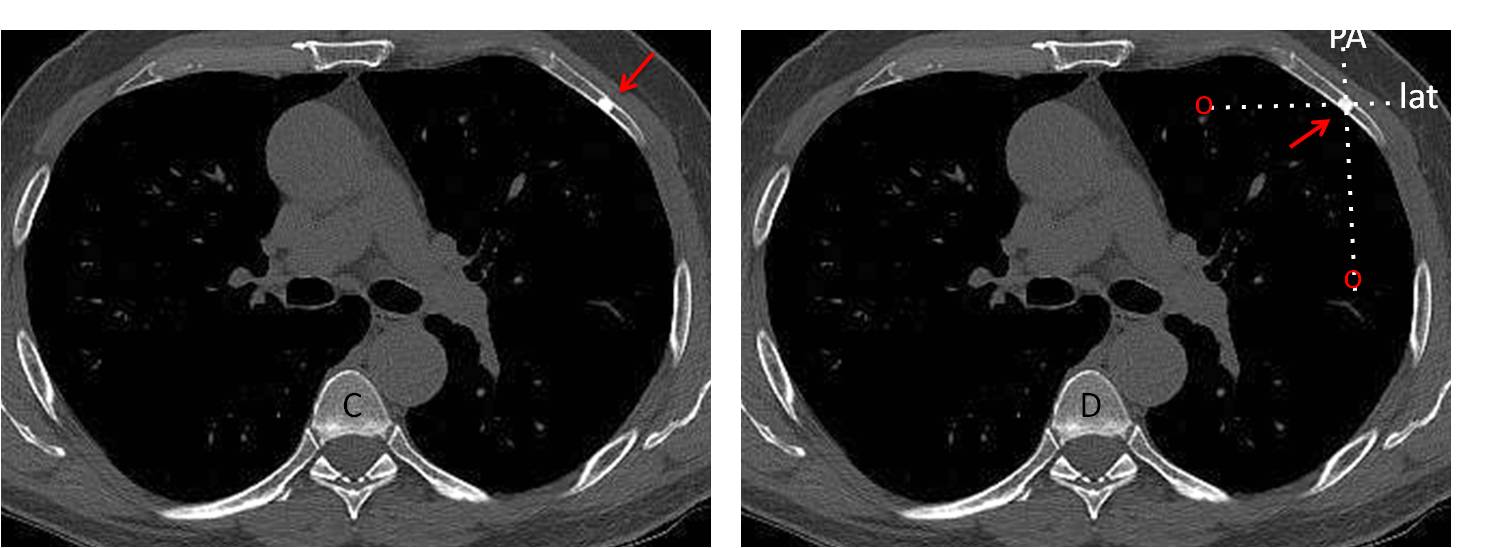
Fig. 5
Pleural calcifications may project over the lung in the PA view, simulating intrapulmonary disease. They are easily identified in the lateral film (Fig. 6) and confirmed with CT in case of doubt (Fig. 7).
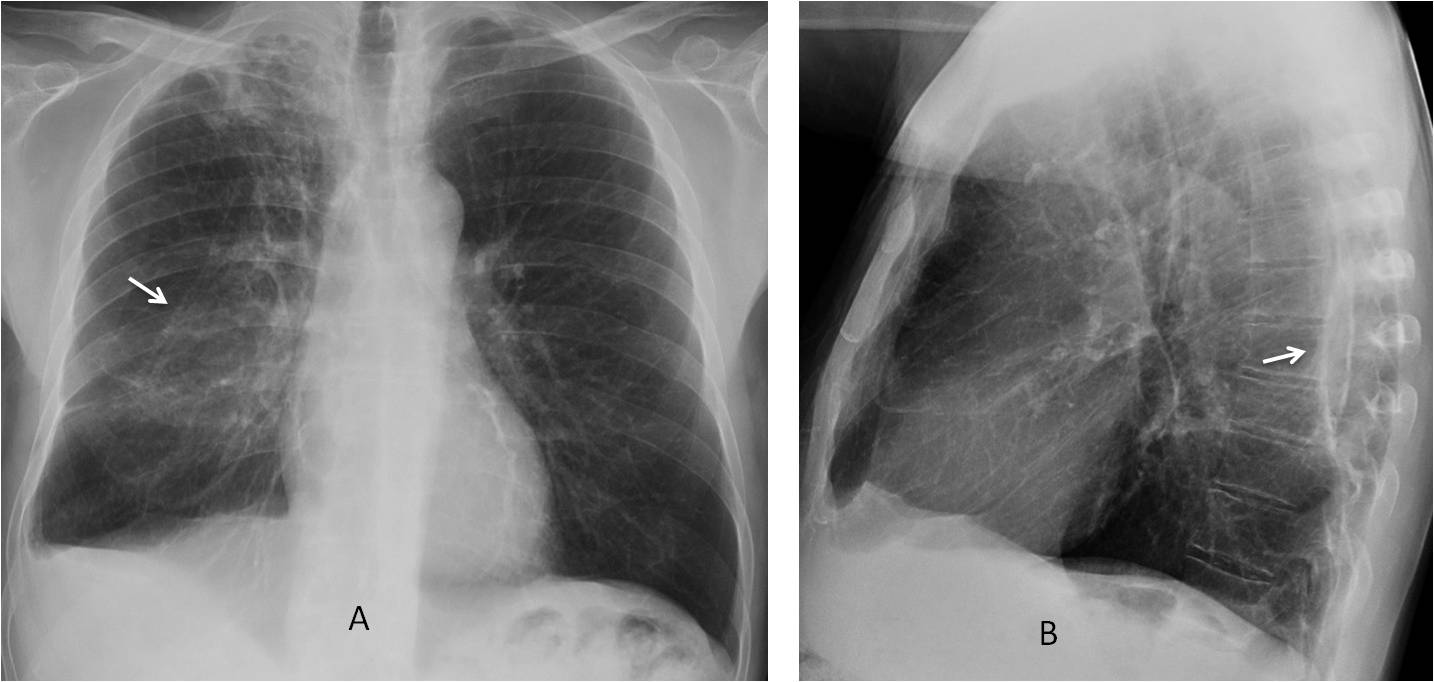
Fig. 6
Fig. 6. 57-year-old man with previous history of TB. PA radiograph shows chronic apical changes and an apparent pulmonary opacity in the right lung (A, arrow). Lateral view shows that the posterior pleura is calcified (B, arrow). Note the blunting of the right costophrenic angle.
Coronal and sagittal CT confirm the marked calcification of the posterior pleural layer (C and D, arrows), which simulates a pulmonary opacity in the PA chest film.
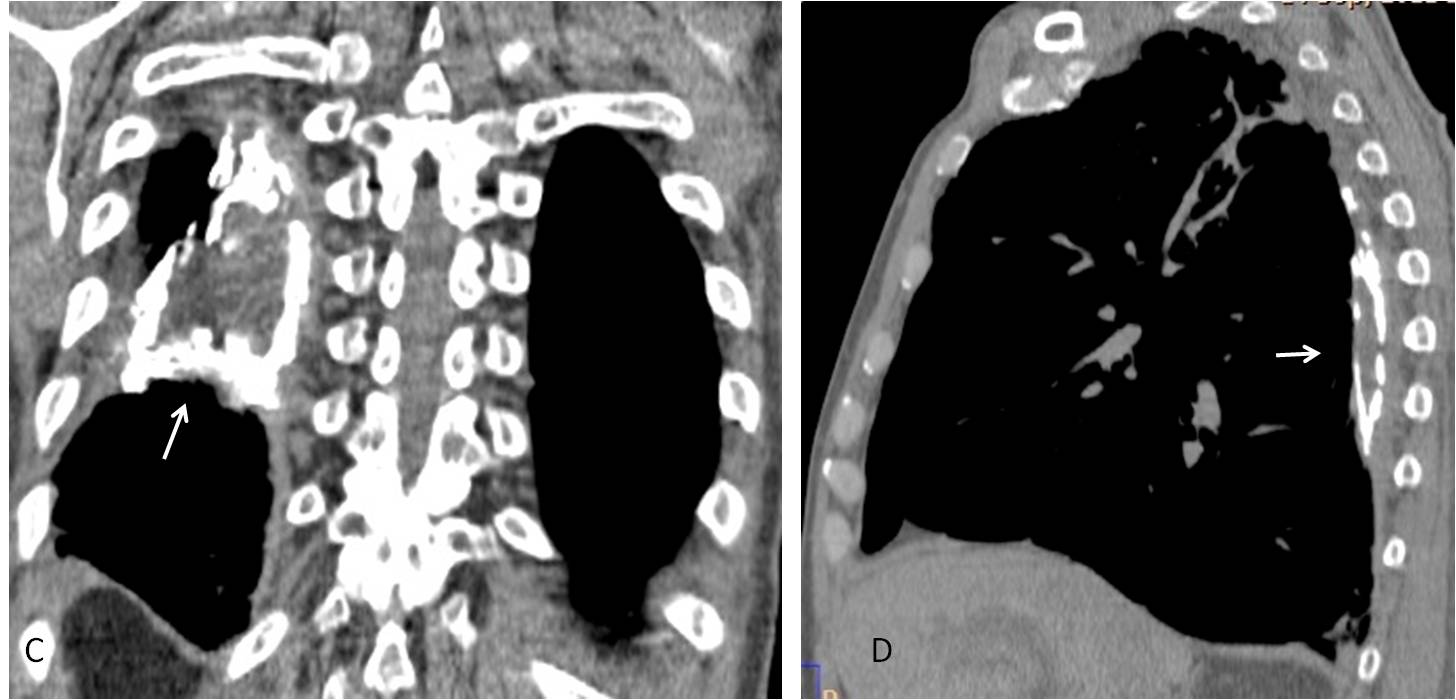
Fig. 6
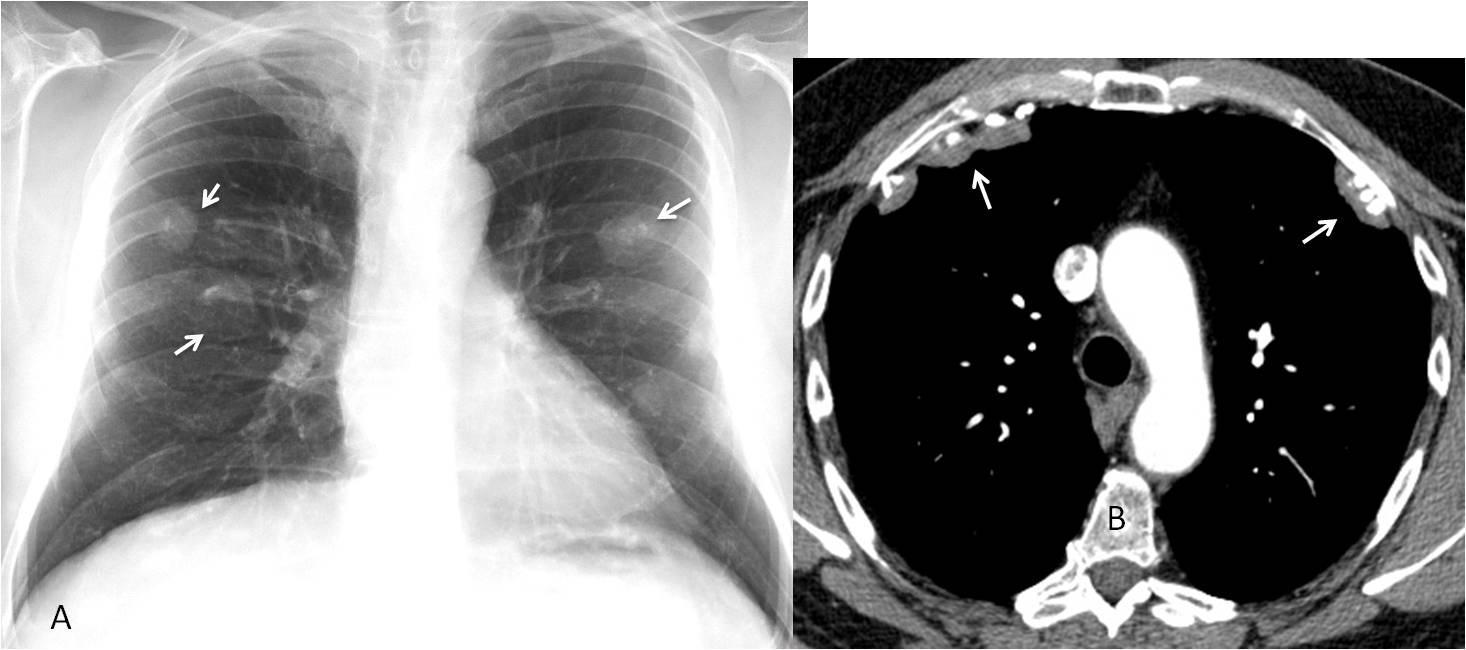
Fig. 7
Fig. 7. PA chest radiograph shows calcified nodules (A, arrows), apparently in an intrapulmonary location. Axial CT demonstrates that the nodules correspond to calcified pleural plaques located in the anterior aspect of the chest (B, arrows). Diagnosis: calcified pleural plaques in asbestos-related disease.
In conclusion, when a chest abnormality is found, it is important to determine if it is intra- or extrapulmonary.
To do that, we should be familiar with the various presentation forms of extrapulmonary masses.
And we should be aware that lesions in the chest wall or pleura may project over the lung parenchyma and simulate a lung lesion.
Next time, I will address the third question: “What does the lesion look like?”

Dr. Pepe’s Teaching Points
1. When a chest abnormality is discovered, determine whether it is intra or extrapulmonary.
2. Extrapulmonary lesions are recognized by the pregnancy sign and the incomplete border sign.
3. Lesions in the chest wall/pleura may simulate intrapulmonary lesions.


I am missing the lateral views, but if I have to say something my opinion is:
Case 1. Extrapleural left lesion
Case 2: Probably intrapulmonary LLL lesion, but it would be a costal lesion too.
Did not show lateral views because they didn’t add any additional information.;-)
Dear Professor, we think both are extra pulmonary lesions.
Case 1: there is pleural base in the lesion with an obtuse angle in the margins.
Case 2: there are peripheric calcifications in the lesion, in LLL indicating rib origin, since it is in the projection of the anterior costal arch.
Good answer in case 2, but you missed the other rib fractures.
Avoid satisfaction of search 😉
…scusa se ho “saltato” la lezione precedente….ero al nostro congressso nazionale SIRM a Napoli.Le lesioni sono entrambe extrapolmonari….la prima, con un angolo di raccordo ottuso superiore è un fibroma solitario della pleura….la seconda sono di pertinenza costale….frattura posteriore della 7 sx….riassorbimento litico della 8 e callo osseo della 9…Sempre nel cuore!
You were missed. Welcome back!
1st is extrapulmonary
2nd is intrapulmonary
Hello.
I think the first one could also be a hampton hump, thus intrapulmonary.
Dear Professor – you are a real inspiration. Thank you.
1. First extrapulmonary – but no definite rib erosion. DD – mets myeloma/ plasmacytoma / fibroma. Would CT this to narrow differential.
2. Second extrapulmonary – Fractured left 7th to 9th rib. The nodule is due to hyperostosis of a healed posterior 9th fracture. Would not CT this.
I rather be an inspiration than an expiration 😉
Are you sure of your first diagnosis?
I think case 1 shows an extrapulmonary lesion with obtuse margins in the left lateral upper lung field, which could be due to an pleural / rib lesion. I suggest rather a malignancy – is there any clinical information, which would be a clue?
The ovoid lesion of case 2 seems to be intrapulmonary in the LLL with rim calcification, which suggests radiographically a benign entity (harmatoma, calcified granuloma etc.). Healed rip fracture is a differential because there are konsolidated rip fractures of the 7th and 8th rip…
In case 1 the patient had pain in the upper left hemithorax. Is the lesion well defined throughout?
Answer case 2 is correct
In my opinion the lesion in case 1 is well circumsribed and smooth with obtuse angels, which clearly goes against an intrapulmonary origin. Therefore I would suggest an pleural lesion, the underlying rib seems to be intact. Therefore pleural fibroma, DD: pleural lipoma would be in my differential. Nevertheless a malignant lesion (pleural metastases of CUP, pleural fibrosarcoma etc.) I wouldn`t definitively exclude before CT-scan, knowing they are quite unlikely…
thanks a lot professor for the solution and explanations….
Hello dear Professor !
Case 1 shows extrapulmonary mass ( pregnancy sign). Anterior aspect of 2 and 3 rib is not visible – malignant costal lesion.
As algoritem – CT
[…] Is there any visible abnormality? (Chapter 1) b) Is it intra or extrapulmonary? (Chapter 2) c) What does it look […]
[…] we’ve looked at the three key questions to ask when facing a chest radiograph (chapters 1, 2 and 3), we move on to the interpretation of pulmonary […]