B-0625 Features on MRI after transanal endoscopic microsurgery in patients with rectal cancer
L.A. Heijnen, M. Maas, M.H. Martens, D.M.J. Lambregts, J.W.A. Leijtens, W. Deserno, G.L. Beets, R.G.H. Beets-Tan | Sunday, March 10, 10:30 – 12:00 / Room A
Purpose: Transanal endoscopic microsurgery (TEM) is a minimal invasive technique for local resection of T1 and selected T2 tumours and is also an emerging option for good-responders after chemoradiation. In most centres follow-up includes regular MRI. This study aimed to describe the MR morphology of the rectal wall during follow-up in patients that received TEM.
Methods and Materials: Forty-nine patients underwent a post-TEM MRI in our centre. For 21 patients only one post-operative MRI was available. For 28 patients >1 MRIs were available. The MR morphology of the TEM-site was studied on the consecutive MR examinations. 32 patients were primary treated with TEM, 17 patients underwent chemoradiation followed by TEM.
Results: We identified three morphological patterns: (1) rectal wall thickening with or without fibrosis, (2) a notch at the TEM-location, and (3) irregular delineation of the rectal wall. Multiple patterns could occur within one patient. 32 patients (65%) had rectal wall thickening, 17 patients (35%) a notch, and 28 patients (57%) irregular delineation of the rectal wall. In addition to these patterns, oedema (due to chemoradiation) persisted in post-chemoradiation TEM-patients. Ten patients had dehiscence after TEM post-chemoradiation (n=58%). Six luminal recurrences occurred; 3 had rectal wall thickening, 3 a notch, and 5 an irregular rectal wall.
Conclusion: Three patterns were identified on MRI after TEM. This enables radiologists to monitor this group of patients more accurately. Since minimal invasive techniques are gaining, it is very important for radiologists and surgeons to have knowledge about the normal follow-up findings after TEM.

Watch this session on ECR Live: Monday, March 11, 08:30–10:00, Room N/O
Tweet #ECR2013NO #SF16B
Organ-sparing surgery and radiation treatment such as intensity-modulated radiotherapy (IMRT) – often combined with chemotherapy – have increased the need for advanced imaging in the head and neck during pre-treament and post-treatment stages. Precision is vital as any tumour that remains undetected outside the treatment field could adversely affect the patients’ prognosis and survival, according to Professor Vincent Vandecaveye, from the department of radiology at the University Hospitals Leuven in Belgium.
It is important to spot any tumour recurrence as early as possible, especially in the post-treatment phase, in order give the patient the best possible chance of salvage treatment. The most common imaging methods in the head and neck area remain CT, MRI and PET-CT; each comes with its own advantages and disadvantages.
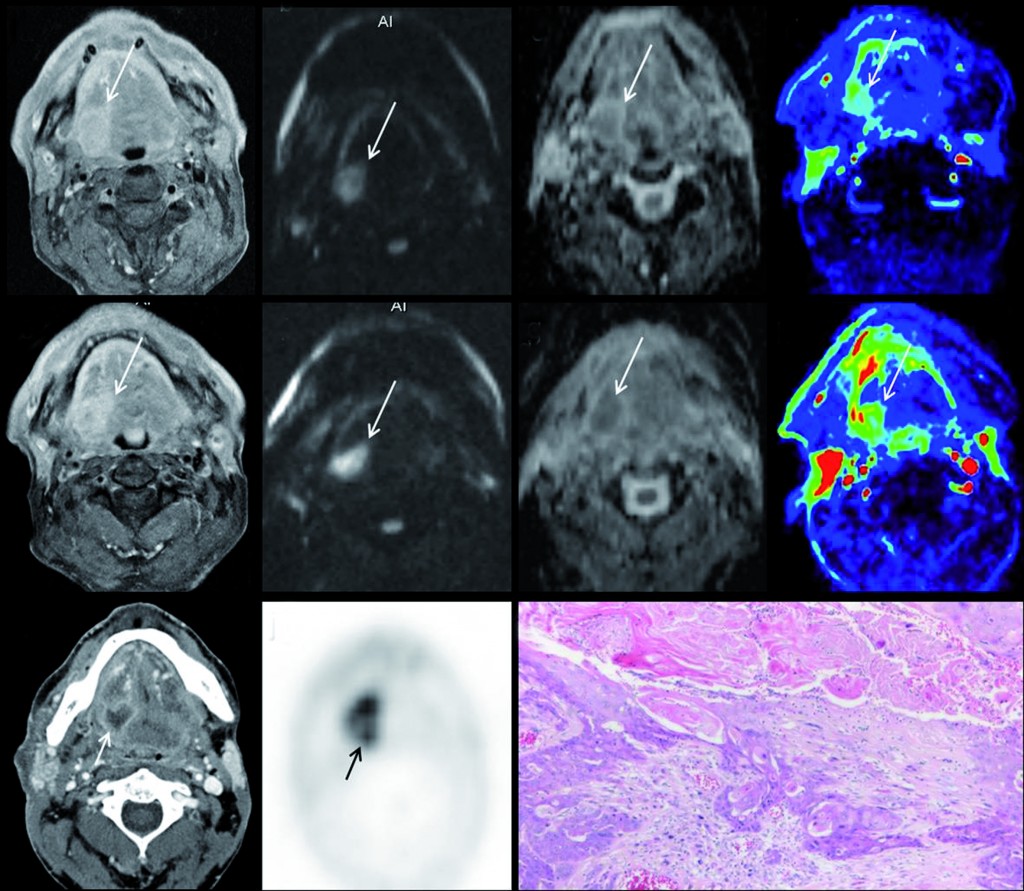
Multiparametric MRI for early treatment prediction of chemoradiation in oropharyngeal cancer: Upper row is pre-treatment MRI of right base of tongue cancer (a=contrast enhanced T1 as anatomical correlate; b=native b1000 diffusion-weighted image; c= ADC-map; d=perfusion-map of IUAC). Middle row is 2 weeks during chemoradiation: same imaging sets, tumour volume will not help. No significant change in b1000, ADC nor perfusion-MRI indicate non-response and thus high risk of tumour relapse after end of treatment. Tumour relapse at PET-CT 8 months after end of treatment, proven by histology (k). (Provided by Professor Vincent Vandecaveye)
Read more…
Watch this session on ECR Live: Friday, March 8, 08:30–10:00, Room F1
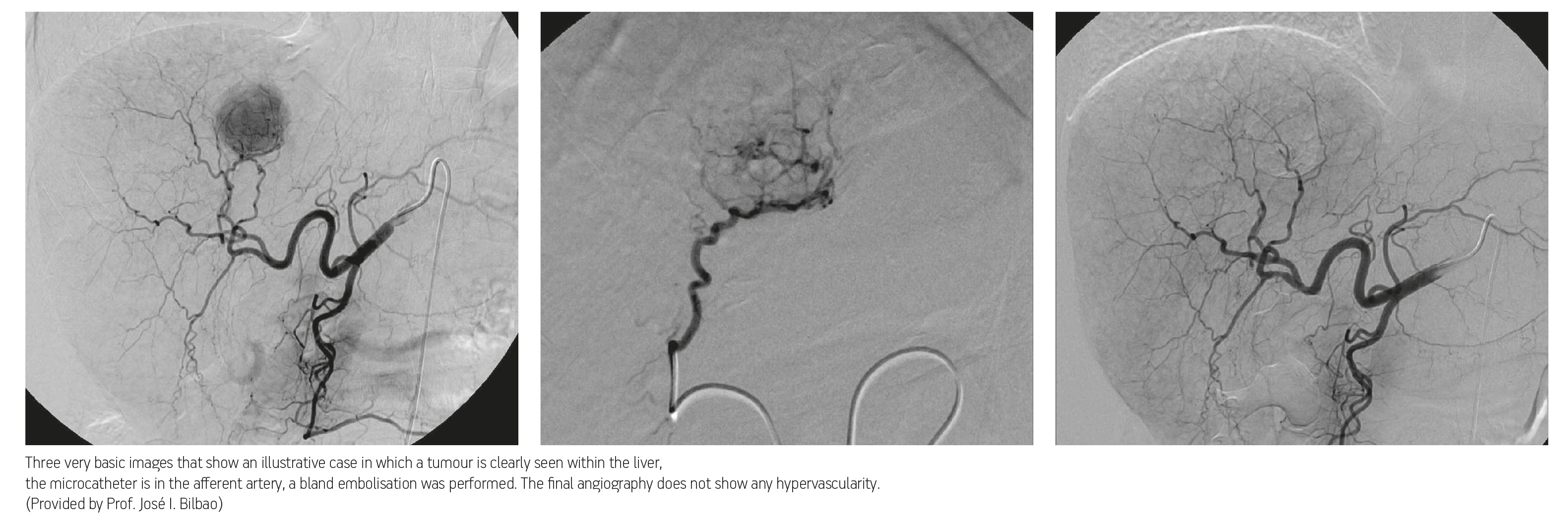
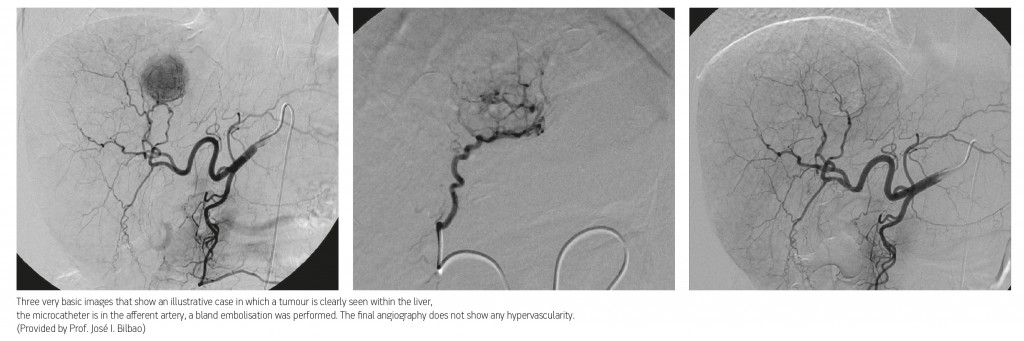
There are a wide range of treatment options available when dealing with hepatocellular carcinoma (HCC), ranging from interventional and endovascular procedures to surgical interventions such as liver transplantation. The main reason for performing endovascular procedures when treating patients with hepatocellular carcinoma is the fact that liver neovascular networks are nourished exclusively by the arteries.
Liver tumours, both primary and metastatic, are almost entirely supplied by branches known as neo-vessels, which originate in the hepatic arteries. The surrounding peritumoural liver parenchyma is vascularised mainly by portal vein branches. When an HCC is larger than two centimetres in diameter the afferent vessel can be identified and then targeted via an arterial endovascular approach. These unique characteristics – dual vascular supply and the ability to identify the afferent vessels – are the rationale behind the use of endovascular treatments, and several different techniques have been developed over the last 30 years. Among the most frequently used are the infusion of chemotherapy and the introduction of particles, either as occluding devices or as carriers of an active agent, which attacks the tumoural cells and surrounding neovessels.
Read more…