Dr. Pepe’s Diploma Casebook: Case 96 – A painless approach to interpretation (Chapter 3) – SOLVED!
Dear Friends,
I hope you remember the three questions to ask when facing a chest radiograph:
a) Is there any visible abnormality? (Chapter 1)
b) Is it intra or extrapulmonary? (Chapter 2)
c) What does it look like?
To discuss the third question, I’m showing chest radiographs of a 36-year-old woman with chest pain.
What does the lesion look like?
1. Pericardial fat pad
2. Thymic tumour
3. Pericardial cyst
4. Any of the above
Check the two images below, leave your thoughts in the comments section and come back on Friday for the solution.


Findings: PA radiograph shows a mediastinal mass at the right cardiophrenic angle (A, arrow), poorly seen in the lateral view (B). All the diagnoses offered are likely, as thymic tumours can migrate downwards. The correct answer is: 4, any of the above.
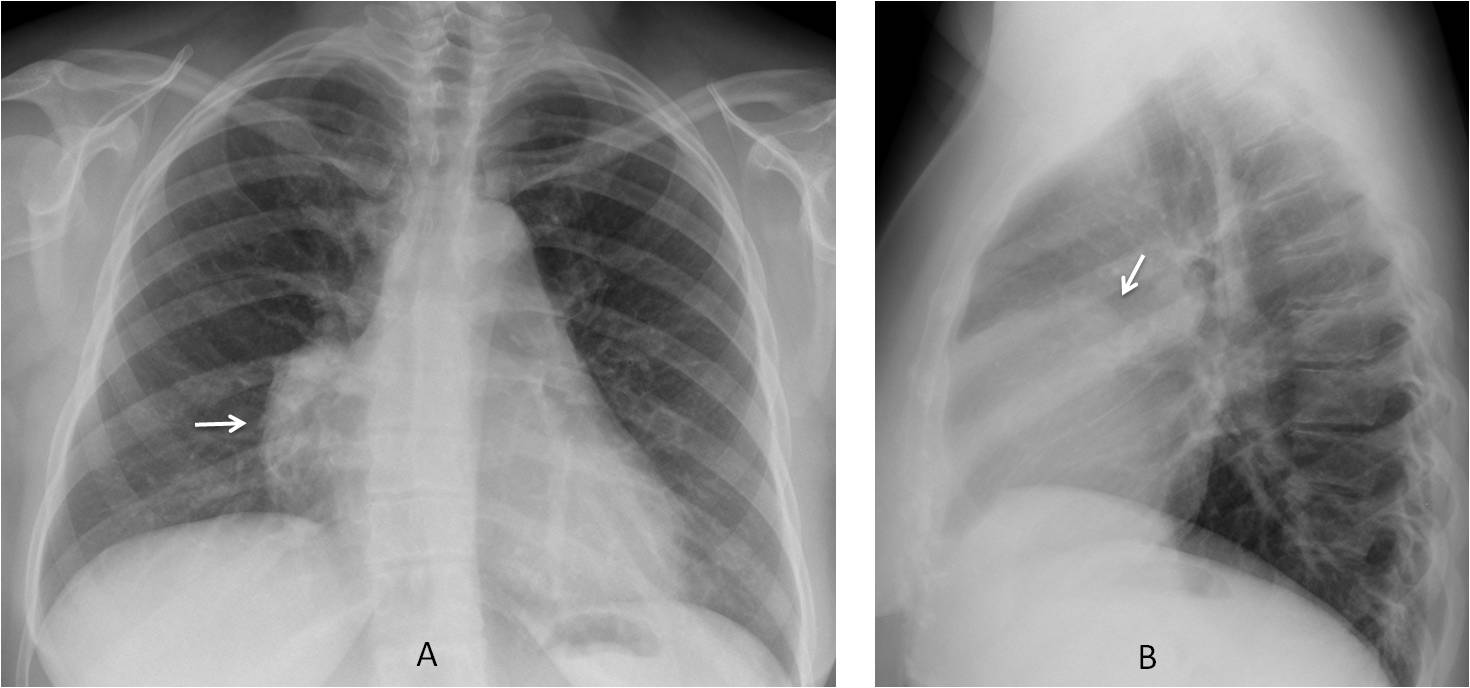
Enhanced CT shows an irregular soft-tissue mass (C and D, arrows) occupying the anterior mediastinum. There is invasion of the sternum (E, arrow). Histologic examination after surgery discovered a lymphoma of the thymus gland.
Final diagnosis: Thymic lymphoma
Third question: What does the lesion look like?
Once the lesion has been identified and placed in a specific chest compartment (mediastinal, extrapulmonary, or pulmonary), recognising its appearance is the final step to begin the diagnostic process.
In this chapter I would like to focus on the detection and management of mediastinal and extrapulmonary lesions, leaving the pulmonary lesions for next week.
Most mediastinal lesions are discovered in the PA radiograph. Broadly speaking, they look like soft-tissue ‘bumps’ in the mediastinum (Fig. 1), identified by the typical pregnancy sign (Diploma Casebook case 95). Since the great majority have no specific characteristics, the role of the chest radiograph is to place the lesion in one of the mediastinal compartments (see Diploma Casebook case 41).
The next step is to perform enhanced CT, which will determine the density of the lesion (fat, fluid, or soft-tissue), narrowing down the possible diagnosis (Figs. 1-3) and discover arterial or venous lesions simulating mediastinal masses (Fig. 4).
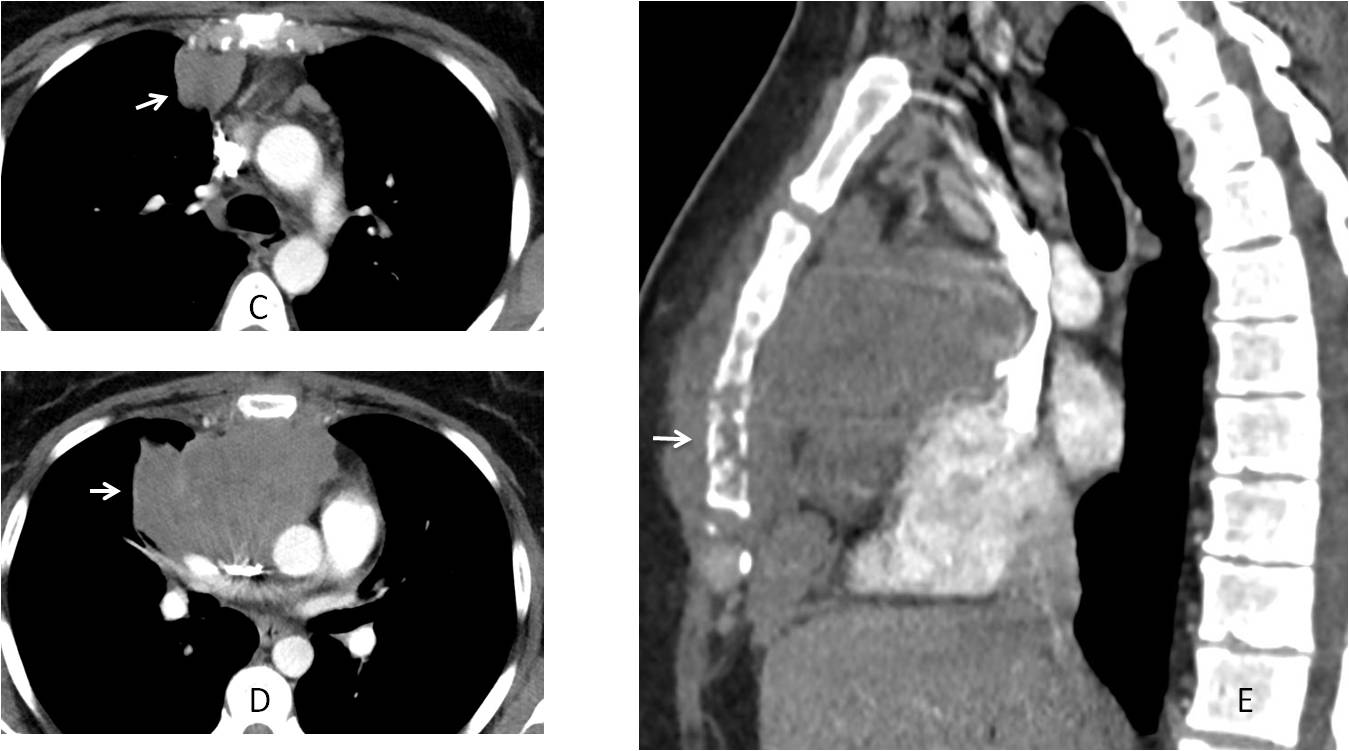
Fat detection in a mediastinal lesion brings to mind three possibilities: mediastinal fat, tumors with fat content, and fatty abdominal hernias (Fig. 1).
Fig. 1
Fig. 1: 45-year-old man with malaise and weight loss. Chest radiographs show an upper anterior mediastinal mass (A and B, arrows). The most likely diagnoses are thymoma, teratoma, or lymphoma. Enhanced axial CT shows fat within the mass (C, asterisk), confirming the diagnosis of teratoma, which was proven malignant at surgery.
Fluid-filled lesions of the mediastinum have two main etiologies: cystic tumours and duplication cysts (Fig. 2).
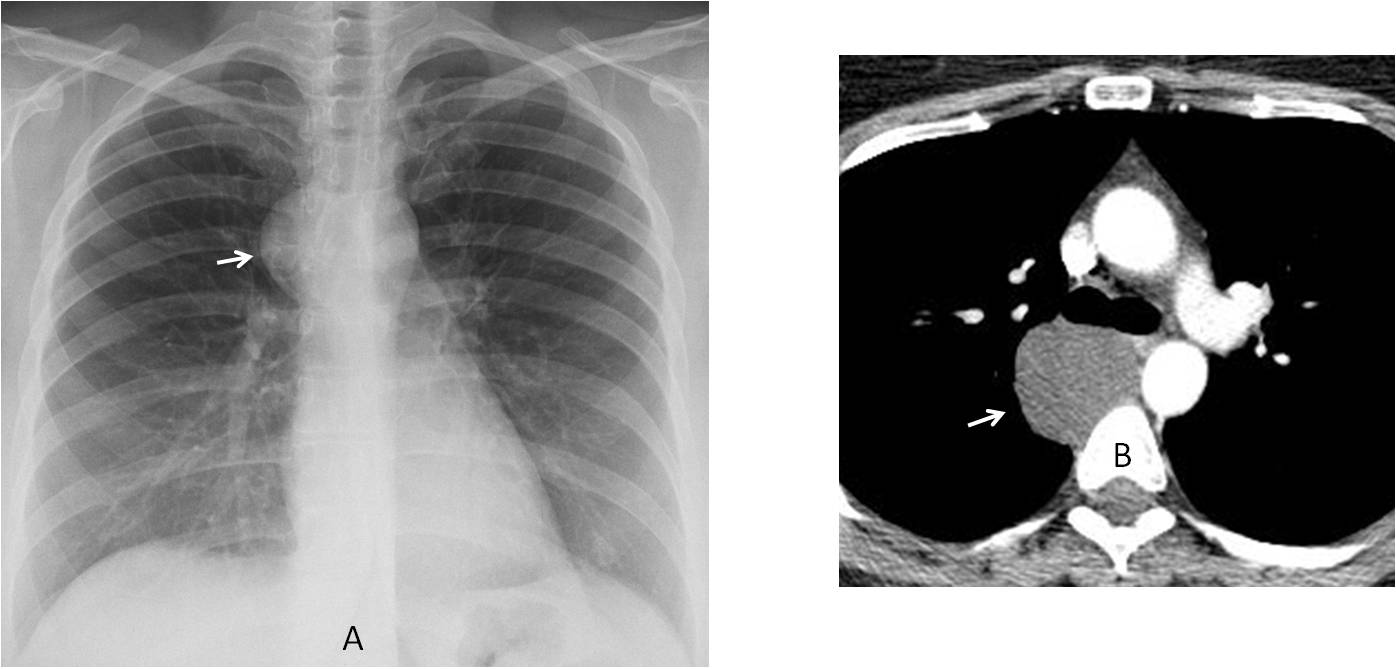
Fig. 2
Fig. 2: Asymptomatic 45-year-old woman with a mediastinal mass (A, arrow), probably located in the right middle mediastinum (no lateral view available). The likely diagnoses are endothoracic goiter, lymph nodes, or duplication cyst. Enhanced CT shows a non-enhancing middle mediastinal mass with fluid content (B, arrow), confirming the diagnosis of duplication cyst.
Soft-tissue masses indicate a solid tumour. The etiology varies depending on the mediastinal compartment: The ‘three Ts’ in the anterior mediastinum, endothoracic goiter in the middle, neurogenic tumours in the posterior, and lymph node disease in all of them.
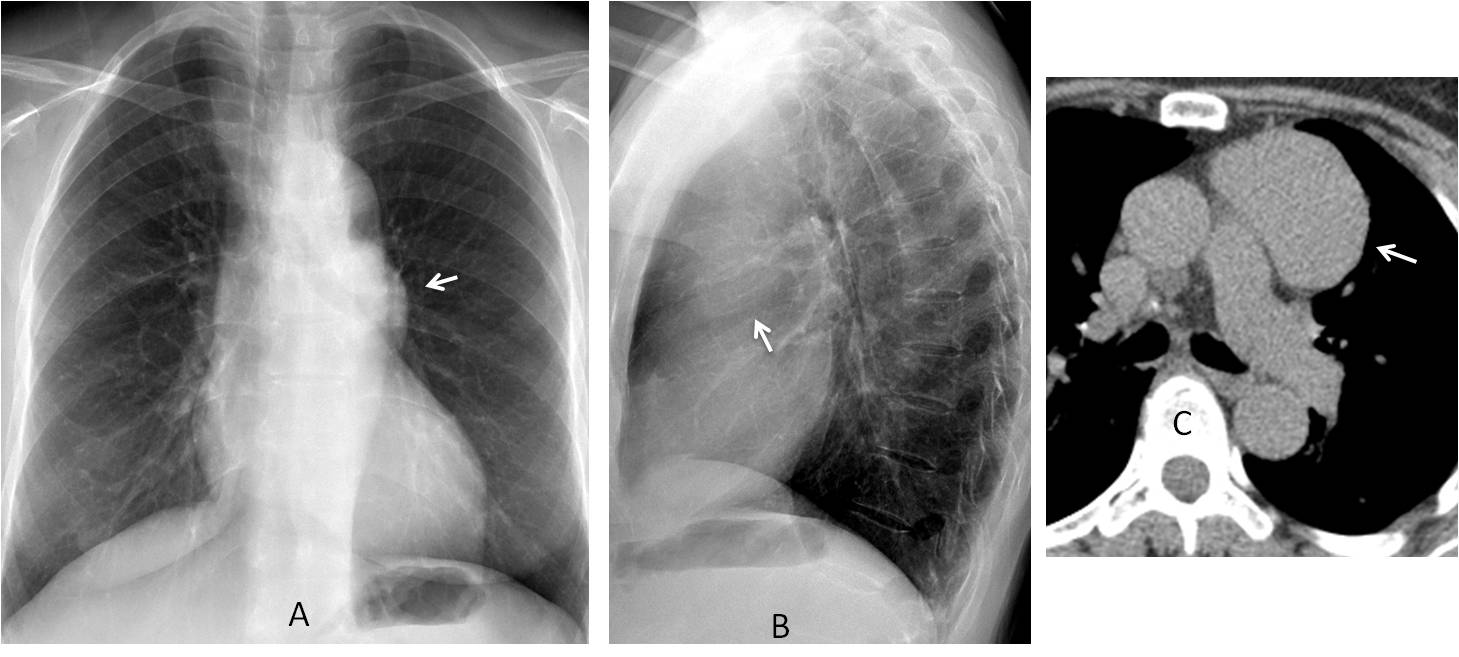
Fig. 3
Fig. 3. Preoperative chest radiograph in a 72-year-old woman shows an unsuspected anterior mediastinal mass (A and B, arrows). Unenhanced CT shows a well-defined soft-tissue mass (C, arrow). Since the patient is asymptomatic, the differential diagnosis falls between thymoma and teratoma. A thymoma was found at surgery.
Enhanced CT should always be done in mediastinal masses to exclude a vascular origin (Fig. 4).
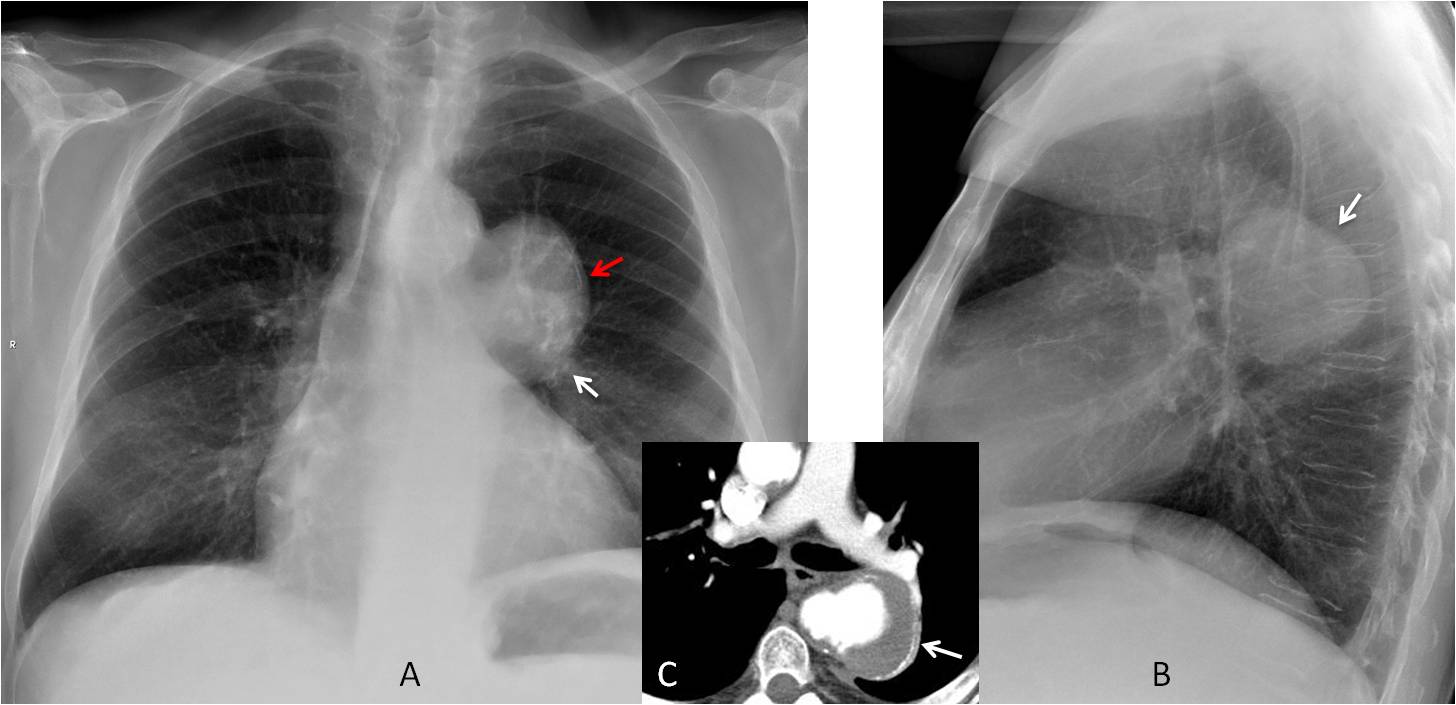
Fig. 4
Fig. 4. Chest radiographs show a middle mediastinal mass (A and B, arrows) with a peripheral lineal calcification in the PA view (A, red arrow). This type of calcification suggests a cyst or a vascular lesion. Enhanced CT confirms a saccular aneurysm of the descending aorta, (C, arrow).
Extrapulmonary lesions occur in the periphery of the chest and are identified by the pregnancy sign and its variants (Diploma Casebook case 95). The diagnostic approach depends on whether the underlying rib is affected. If it is, the main diagnoses in adults are metastatic disease or myeloma (Fig. 5), with primary rib lesion a distant third.
If no rib lesion is present, CT should be done to evaluate the density of the lesion, which will determine the most probable diagnosis:
1. Fat density represents extrapleural fat, a clinically non-significant finding (Fig. 6)
2. Fluid density occurs in loculated pleural fluid (Fig. 7)
3. Soft tissue density represent a solid tumor, with two main possibilities: fibrous tumour of pleura or pleural metastasis (Fig. 8).
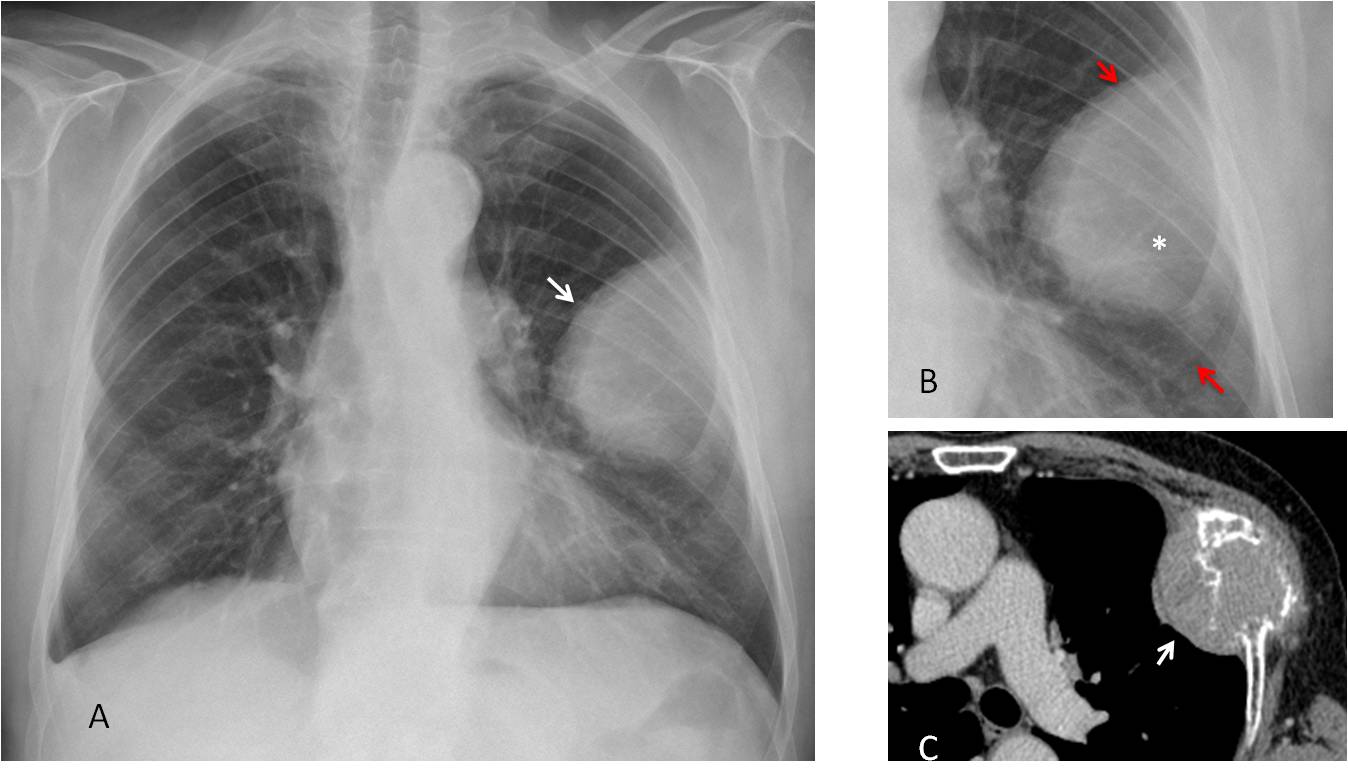
Fig. 5
Fig. 5: 56-year-old man with liver cirrhosis. PA radiograph depicts an extrapulmonary mass (A, arrow). Cone down view demonstrates that the underlying rib is missing (B, asterisk), whereas the ribs above and below are clearly seen (B, arrows). CT confirms the rib lesion (C, arrow). Final diagnosis: metastasis from hepatocarcinoma.
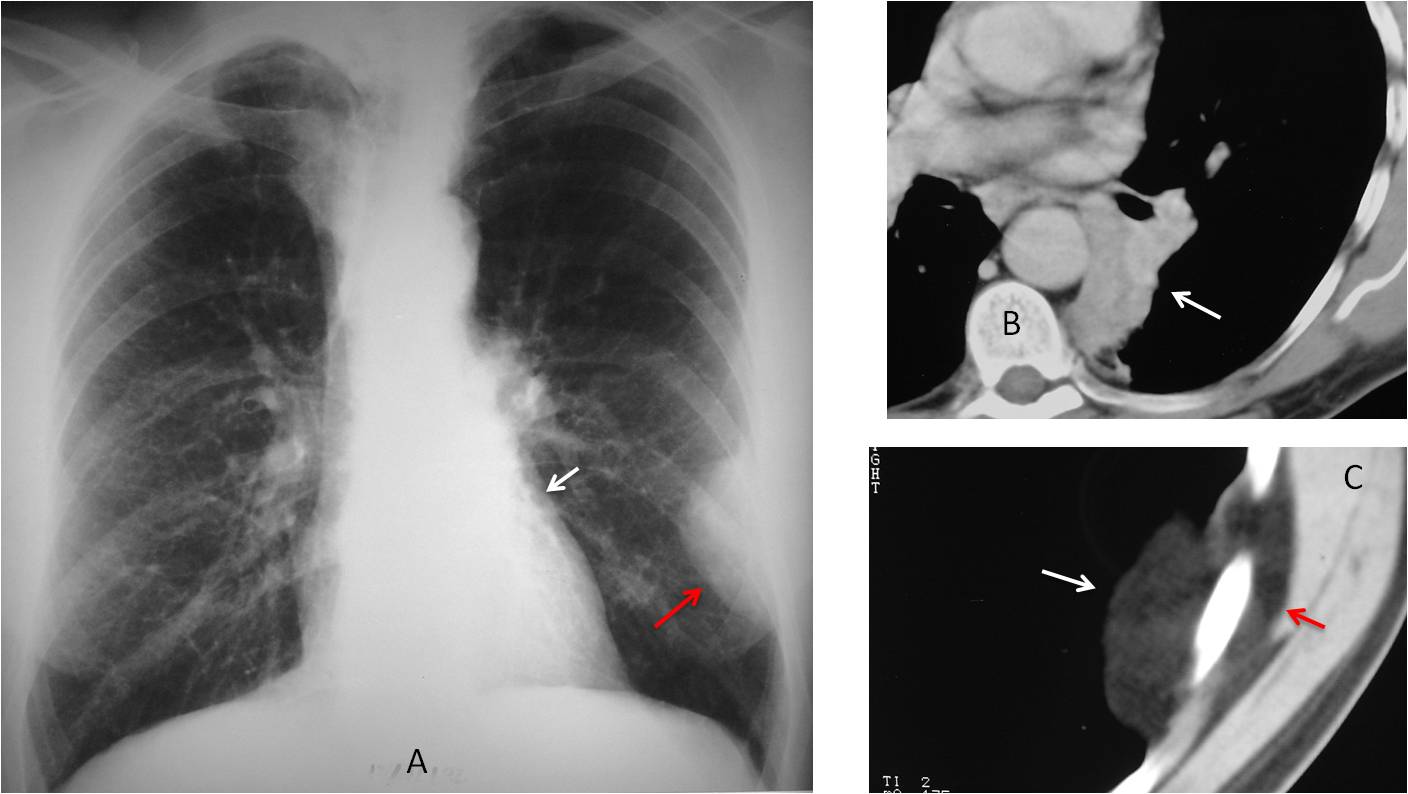
Fig. 6
Fig. 6: 57-year-old man with LLL collapse (A, white arrow) and a typical left extrapulmonary lesion (A, red arrow). Axial CT confirms the LLL collapse (B, arrow), secondary to carcinoma. The peripheral lesion (C, white arrow) represents extrapleural fat and is, therefore, innocuous. Note the parietal fat component (C, red arrow).
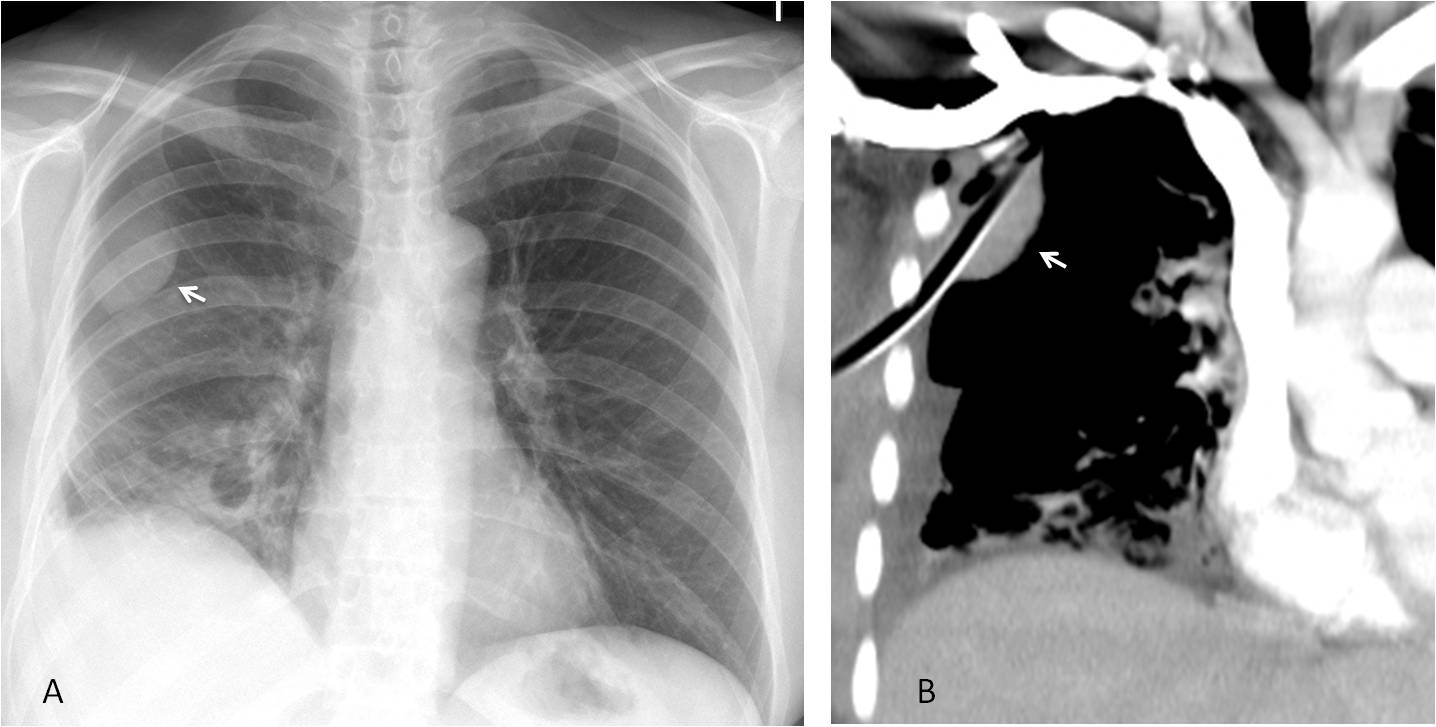
Fig. 7
Fig 7: 42-year-old man with pneumonia and pleural effusion. PA radiograph shows an extrapulmonary lesion with an incomplete border sign (A, arrow), most likely loculated pleural fluid. Enhanced coronal CT shows the draining tube in the loculation (B, arrow).
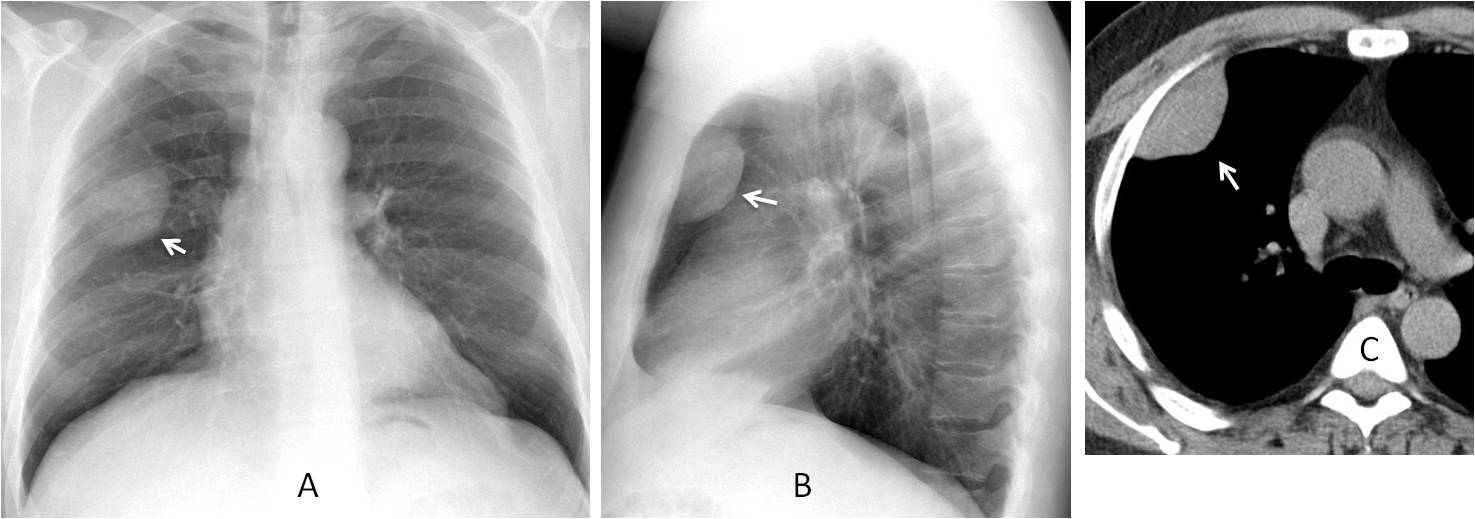
Fig. 8
Fig. 8: 45-year-old man with mild cough. Chest radiographs show an extrapulmonary mass (A and B, arrows), with an incomplete border sign in the PA view. Unenhanced CT depicts an extrapulmonary soft-tissue mass (C, arrow). Fibrous pleural tumour is the most likely diagnosis, confirmed at surgery.
In conclusion, once we know the location and appearance of a lesion, we can determine the most likely diagnosis and further management.
Mediastinal lesions are identified by the pregnancy sign in the chest radiograph. Enhanced CT determines the density of the lesion (fat, fluid, or soft-tissue) and excludes arterial or venous conditions mimicking a mediastinal mass.
Extrapulmonary lesions are identified by the pregnancy sign and incomplete border sign. In adults, destruction of the underlying rib suggests myeloma or metastasis. When the rib is intact, CT determines the density of the lesion and the likely diagnosis: extrapleural fat, loculated pleural fluid, or a solid lesion (fibrous pleural tumor vs. metastasis).
Next week I’ll discuss the patterns in pulmonary lesions.

Dr. Pepe’s teaching points:
1. Mediastinal lesions are discovered in the chest radiograph and are diagnosed by enhanced CT.
2. In extrapulmonary lesions, identify the underlying rib. If it is not affected, CT will determine the density of the lesion and the most likely diagnosis.


Hi, have a nice week.
4. Any of the above-Differential diagnosis of right cardiophrenic angle mass
CT to differentiate fat vs fluid vs solid component, for example
Fat (pericardial fat pad, lipoma, thymolipoma, liposarcoma usually in posterior mediastinum)
Fluid (pericardial cyst)
Solid (thymoma, lymphoma)
The PA view shows a paracardiac right increased density (silhouette sign) with an hilum overlay sign, that we can locate anterior in the lateral view. In this proyection the retrosternal space is obliterated. We have a thickening of the right paratracheal line but it will be secundary to scoliosis with dorsal right convexity is seen in the PA view.
I think that it is an anterior mediastinum mass (diferential diagnosis in this case would be: lymphoma, pericardial cyst, teratoma).
Dear professor, in PA view we see a lesion with undefined margins but with hilum overlay sign, which may correspond an anterior or posterior origin. Also cardiac silhouette is obliterated. In lateral view we cannot say there is a posterior lesion. So, we think it`s anterior. It could be any of the options given: Pericardial fat pad; Thymic tumour; Pericardial cyst
It looks like right middle lobe collapse.
Of differential listed above, pericardial fat pad is most likely as it has ill define margin.
Both thymus tumor and pericardial cyst should have well defined margin which is not the case here.
A fairly well defined smooth opacity is seen obscuring the right heart border with broad base towards the mediastinum. Vessels are seen through the mass s/o Anterior mediastinal mass.
DD: Pleuropericardial cyst,Pericardial fat pad.
….l’opacità sembra del mediastino antero-inferiore: cisti peluro-pericardica.
Do you think that cyst is the only cause?
Greetings from Lisbon
….ritorno venoso anomalo parziale…s. Della scimitarr? Ma il polmone non è’ ipogenetico…..Lisboa è’ romantica …prof.,…attento….!
Correct answer is 4. Any of the above. More information tomorrow.
Congratulations to Panagiotis, MK and UFTM radiogroup, in that order.
[…] looked at the three key questions to ask when facing a chest radiograph (chapters 1, 2 and 3), we move on to the interpretation of pulmonary […]